
Abstract
Background
We describe a four-generation Italian family with familial hemiplegic migraine (FHM) and epilepsy due to a novel ATP1A2 missense mutation (R1007W).
Case results
Mutational analysis revealed a heterozygous nucleotide substitution c.3019C>T resulting in the missense substitution p.Arg1007Trp (p.R1007W) in seven subjects: Three individuals had hemiplegic migraine, two exhibited a clinical overlap between migraine and epilepsy, one had migraine and one was unaffected. The identified ATP1A2 mutation was not found in an ethnically matched control population of 190 individuals and was not reported in a polymorphisms database.
In two-electrode voltage-clamp experiments on Xenopus oocytes, the ATP1A2 R1007W mutant showed (i) reduced ion pumping activity due to a more profound voltage dependence and (ii) decreased apparent affinity for extracellular K+ at voltages around the cellular resting potential. This distinct type of loss of function has not been reported for other FHM2 mutations and can lead to impaired K+ clearance and elevated K+ levels in the CNS.
Conclusions
The functional data and clinical evidence suggest that in FHM2 migraine and epilepsy may originate from the same pathogenic mechanisms associated with genetically determined alterations of ion channels and pumps. Our data also support the hypothesis that the new mutation R1007W in our family may be a susceptibility factor for epilepsy.
Keywords
Introduction
The mechanisms underlying the association between epilepsy and migraine are still to be explained, although several studies have supported the idea that an induction of neuronal hyperexcitability would better indicate a pathological mechanism shared by the two disorders (1). Migraine and epilepsy may be linked by genetic and molecular substrates in some clinical conditions. Current molecular genetics insight into the pathophysiology of migraine predominantly comes from studies of a rare monogenic subtype of migraine with aura defined as familial hemiplegic migraine (FHM) and characterized by transient hemiparesis during the aura (2). Three genetic subtypes of FHM have been identified. FHM1 or FHM type 1, which accounts for approximately 50% of FHM patients, is caused by mutations of the CACNA1A gene, coding for the alpha 1A subunit of the voltage-dependent, P/Q-type calcium channel (3). FHM2 or FHM type 2, which accounts for <25% of FHM cases, is caused by mutations of the gene ATP1A2, encoding the Na+/K+–ATPase α2-subunit (4). FHM3 or FHM type 3, is a rare subtype of FHM and is caused by mutations of the SCN1A gene encoding the neuronal voltage-gated sodium channel α-subunit (5). These three genes do not account for all cases of FHM, suggesting the existence of at least one additional locus (6). Many of the nonfamilial cases of hemiplegic migraine (sporadic hemiplegic migraine) are also caused by mutations of these three genes. The clinical presentation of sporadic and familial cases with identified mutations varies from pure hemiplegic migraine to severe early-onset forms with recurrent coma, cerebral edema, and permanent cerebellar ataxia (7), and comorbidity with epilepsy has been reported previously (8–10).
The ATP1A2 gene, which is mutated in FHM2, is predominantly expressed in astrocytes (4). The Na+/K+–ATPase belongs to the P2C subfamily of P-type ATPases; its functional unit consists of a large catalytic α-subunit and a smaller accessory β-subunit. It is an electrogenic ion transporter, which utilizes the free energy of ATP hydrolysis to export 3 Na+ ions and import 2 K+ ions per ATP molecule, thus maintaining the physiological gradients for Na+ and K+ ions. The pump is therefore crucial for the activity of secondary active transporters, which utilize these gradients for transport of other solutes like Ca2+ ions or neurotransmitters, but also for ion channels that are active during action potentials or set the threshold of neuronal firing. FHM2 mutations either cause complete loss of function, decrease catalytic activity or induce complex changes in ion transport, voltage dependence or cation affinities (11). The link between Na+/K+–ATPase dysfunction and headache is still poorly understood. It is assumed that most of the aura symptoms are linked to the phenomenon of cortical spreading depression (CSD), which emerges from a certain focus on the neocortex forming a slowly spreading front of neuronal excitation that encloses an area of long-lasting depression (12).
Mutations in each of the three FHM-associated genes might induce not only CSD, but also abnormal neuronal discharges leading to epilepsy in some patients (7). Seizures occurring independently from hemiplegic migraine attacks have been reported in more than 60 familial and sporadic cases with mutations of the CACNA1A, ATP1A2 and SCN1A genes.
We describe the clinical, genetic and functional study of a four-generation Italian family with a novel ATP1A2 mutation. We studied 11 individuals; the proband had hemiplegic migraine (HM) and benign myoclonic epilepsy, another member had HM and benign rolandic epilepsy, three had HM only, one had migraine and five individuals were unaffected.
Materials and methods
Patients
The family was ascertained through the proband, referred to the Epilepsy Unit of Child Neurology and Psychiatry Department of Cagliari University Hospital (Sardinia, Italy). Eleven family members were studied (four unaffected and seven affected) (Figure 1(a); II:1; II:2; II:3; III:1; III:2; III:3; III:4; IV:1; IV:2; IV:3; IV:4). All participating individuals and parents, in the case of minors, gave informed consent. This study was undertaken with the approval of the Human Research Ethics committee of the Cagliari University Hospital. The diagnosis of FHM followed the criteria of the International Headache Society (IHS) second edition (13). Seizure types and epilepsy syndromes were classified according to the International Classifications of Epilepsy Syndromes (14). The proband (IV:1) is a 16-year-old boy. After a normal neurological development, at 18 months he manifested myoclonic seizures during drowsiness with generalized polyspike and waves on ictal-electroencephalogram (EEG). Cognitive level and brain magnetic resonance imaging (MRI) were normal. Seizures disappeared with valproic acid treatment and never relapsed. Treatment was stopped after two years and a diagnosis of benign myoclonic epilepsy was made. From the age of six years, attacks of migraine without aura appeared. At the age of 12, he had his first HM attack characterized by right hemiparesis, paresthesia, dysarthria and impaired consciousness. Neurological symptoms were accompanied by severe headache in the left parietotemporal region, nausea and vomiting. With intravenous ketoprofen treatment, symptoms disappeared within 24 hours from the onset. Cranial computed tomography (CT) during the attack was normal, but brain MRI, performed four days after the attack, showed brain edema in the left centrotemporal region. Brain MRI, repeated away from the attacks, was normal. The patient presented another episode of HM two weeks later, a third episode one year later and various sporadic episodes of migraine without aura.
Pedigree and schematic representation of the ATP1A2 protein. Reaction cycle of the Na+/K+–ATPase and localization of R1007 on the 3D structure. Electrophysiological characterization of ATP1A2 mutant R1007W.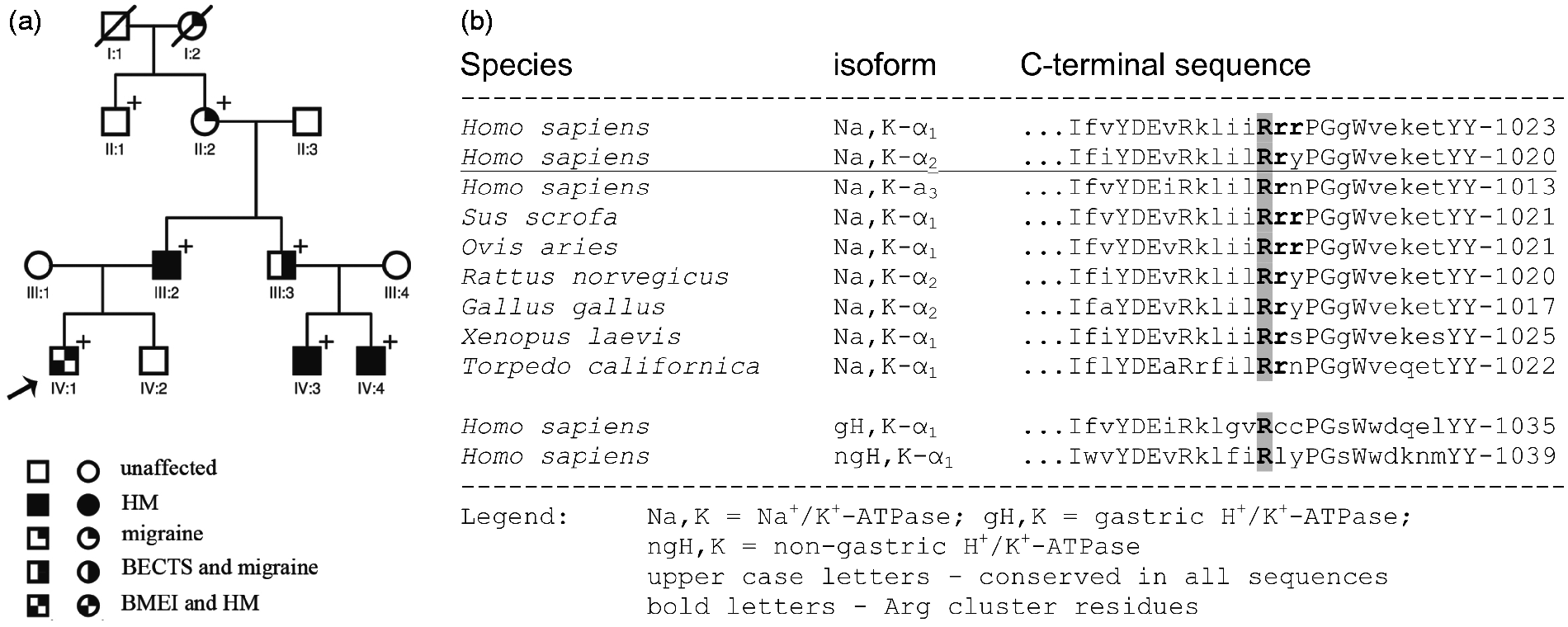


Patient IV:3, a 20-year-old man, experienced attacks of migraine without aura since the age of 14 years and an episode of HM at the age of 15 years. During the aura he experienced motor deficit of the right upper limb, which then extended to the right hemiface and was accompanied by paresthesia and dysarthria, followed by intense right frontal headache. The frequency of HM was about one every two months. EEG has never been recorded.
Patient IV:4, a 21-year-old man, has had sporadic episodes of HM since he was 15 years old. The aura is characterized by right upper limb weakness subsequently spreading to the right hemiface, accompanied by paresthesia, dysarthria, blurred vision and phosphenes followed by intense frontal headache. The frequency of attacks is about one every four months. EEG was never recorded.
Patient III:2, a 56-year-old man, presented episodes of migraine with aura at the age of 41 years, accompanied by dysarthria and paresthesia, starting from the right upper lip and then spreading to the ipsilateral hemiface and arm. Subsequently, he manifested episodes of right frontotemporal headache associated with vomiting. Cranial CT was normal. EEG was not performed.
Patient III:3, a 54-year-old man, had sporadic nocturnal seizures at the age of 7 years with centrotemporal spikes on the EEG. A diagnosis of benign rolandic epilepsy was made. At present he experiences sporadic attacks of migraine without aura.
Patient II:2, an 81-year-old woman, suffers from migraine without aura.
Patient I:2, a deceased woman, had episodes of migraine without aura.
Patients I:1, II:1, II:3; III:1, III:4 and IV:2 never had epilepsy or migraine.
ATP1A2 Mutation analysis
Peripheral blood samples were obtained from probands and available relatives (11 living subjects as in Figure 1(a)). Genomic DNA was extracted using an automated DNA isolation robot, according to the manufacturer’s protocol (QIAsymphony, QIAGEN, Germany). The 23 exons covering the coding regions of ATP1A2 (Entrez Gene, GeneID: 477, Accession Number: NM_000702.3) and their respective intron-exon boundaries were amplified by polymerase chain reaction (PCR) and cycle sequenced using the BigDye Terminator v.1.1 chemistry (Applied Biosystems, Foster City, CA, USA). The sequence reactions were analyzed on a 3130XL ABI Prism DNA sequence (Applied Biosystems, Foster City CA, USA). Primer sequences and PCR/sequencing conditions are available on request.
cDNA constructs
Human Na+/K+–ATPase α2- and β1-subunit cDNAs were used as described in Tavraz et al. (11). ATP1A2 carried mutations Q116R and N127D for ouabain resistance and is referred to as ATP1A2 WT herein. Mutagenesis used the QuikChange site-directed mutagenesis kit (Stratagene, La Jolla, CA, USA) and was verified by sequencing (Eurofins MWG Operon, Ebersberg, Germany).
Ethics statement for experiments on animals
Surgical removal of ovary tissue from adult Xenopus laevis females followed protocols approved by the local state authority (LAGeSo Berlin, Reg. No. O 0308/06) and the ethics committee in accordance with the German Animal Protection Act. Animals were anesthetized by immersion in water containing 0.2% w/v MS-222 (Sigma, Deisenhofen, Germany) for five minutes, and placed on ice during surgery to minimize suffering.
cRNA synthesis and oocyte treatment and electrophysiology
cRNA was synthesized with the T7 mMessage mMachine kit (Ambion, Austin, TX, USA), 25 ng α2-subunit and 2.5 ng of β1-subunit cRNA were injected per oocyte. Preceding experiments, intracellular (Na+) was elevated as described previously (11). Currents were recorded using the two-electrode voltage-clamp (TEVC) technique with a Turbotec 10CX amplifier (NPI instruments, Tamm, Germany) and pClamp 7 software (Axon Instruments, Union City, CA, USA) at room temperature (21–23℃). Solutions used were (in mM): Na-buffer (100 NaCl, 1 CaCl2, 5 BaCl2, 2 MgCl2 and 2.5 MOPS, 2.5, TRIS, pH 7.4), K-buffers with certain (K+) (x KCl, 100 NaCl, 5 BaCl2, 2MgCl2, 1 CaCl2, 2.5 MOPS, 2.5 TRIS, pH 7.4). All buffers contained 10 µM ouabain to inhibit the endogenous Na+/K+–ATPase. All methods are described in detail in Tavraz et al. (11).
Results
ATP1A2 Mutation analysis
Mutational analysis in the proband (see family pedigree in Figure 1(a)) revealed a heterozygous nucleotide substitution c.3019C > T resulting in the missense substitution p.Arg1007Trp (p.R1007W) affecting a highly conserved Arg residue (Figure 1(b)) located at the intracellular end of transmembrane segment M10 (see also Figure 2(b), (c)). Six family members, including the two patients exhibiting both migraine and epilepsy (II:2, III:2, III:3, IV:1, IV:3 and IV:4) and one unaffected individual (II:1) were mutation positive. The identified ATP1A2 mutation was not found in a control population of 190 ethnically matched subjects and was not reported in polymorphisms database queried by the Kaviar2 tool (http://db.systemsbiology.net/kaviar/cgi-pub/Kaviar2.pl).
Electrophysiological studies
We expressed ATP1A2 WT and the R1007W mutant in Xenopus oocytes, and compared the voltage-dependent Na+/K+ pump currents at different [K+]ext, as well as ouabain-sensitive pre-steady state currents in the absence of K+ext (at [Na+]ext = 100 mM). Whereas the average Na+/K+ pump current at 10 mM K+ and 0 mV was comparable (means ± S.D. for WT: 183 ± 78 nA; for R1007W: 217 ± 93 nA; N = 10–14 cells from two batches), the current-voltage curve at [K+]ext = 10 mM of the R1007W mutant exhibited a steeper voltage dependence, thus decreasing more profoundly at voltages below −20 mV compared to WT (Figure 3(a)). Of note, at [K+]ext = 0, the ouabain-sensitive stationary currents of R1007W were indistinguishable from WT (Figure 3(a)) showing that R1007W, unlike other FHM2 mutations within the C-terminal region reported previously (16–19), does not induce Na+-dependent proton “leak” currents. Besides the current-voltage curves, the voltage dependence of the K0.5[K+ext] curve of R1007W is also different, which represents the values for the apparent affinity for extracellular K+. The of ATP1A2 WT (Figure 3(b)) determined from the [K+]ext-dependent current amplitudes at each holding potential (Supplementary Figure 1) exhibits a minimum (i.e. maximal apparent K+ affinity) around 0 mV and increases with de- and hyperpolarization. For the WT, the K0.5 values increase at positive potentials, since positive membrane voltage counteracts the weakly electrogenic binding of extracellular K+ ions, whereas the strongly voltage-dependent competition of extracellular Na+ with K+ accounts for the K0.5 increase at negative potentials. Compared to WT, the K0.5 values of R1007W are larger in the range of physiological potentials (−60…+40 mV, Figure 3(b)) indicating a decreased apparent K+ affinity. Below -80 mV, the K0.5 values of R1007W are smaller than WT values, despite large errors bars due to the small current amplitudes (Supplementary Figure 1). Also, ouabain-sensitive pre-steady state currents of mutant R1007W show differences. These transient currents contain information about kinetics and voltage dependence of the enzyme’s interaction with extracellular Na+ during the E1P(Na+) ↔ E2P(Na+) ↔ E2P + Na+ reaction branch (gray in Figure 2(a)). The voltage dependence of the translocated charge (Q(V) curve) from these currents (Figure 3(d)) for mutant R1007W is shifted by about +17 mV compared to WT. Since reverse binding of extracellular Na+ to the binding pocket saturates already at more positive potentials, this shift could be interpreted as an increased apparent affinity for extracellular Na+, but equally well with a change in kinetics that leads to a destabilization of E2P (or stabilization of E1P). Indication for a kinetic change stems from the increased rate constants of the transient currents for R1007W compared to WT (Figure 3(e)). Since the increase is more pronounced at negative potentials, the preferred acceleration of the E2P + Na+→ E2P(Na+) backward reaction may enhance the voltage-dependent uptake of extracellular Na+.
Discussion
We describe an Italian family with FHM and epilepsy, segregating as an autosomal dominant trait, in which we demonstrated a novel ATP1A2 missense mutation (R1007W). Diverse lines of evidence support the hypothesis that the mutation is responsible for the disease: its cosegregation in the FHM phenotype; its absence in the matched control population; the fact that the mutation lies within a highly conserved and functionally C-terminal portion of the α2-subunit (Figure 1(b)) and causes functional changes that can be linked to mechanisms of migraine triggering. Other FHM2 mutations localized in the C-terminal region are D999H (20), R1002Q (21) and X1021R (22). Functional analysis of mutations R1002Q (18) and X1021R (representing a stop codon mutation leading to a C-terminal expansion by 28 amino acids) (11) showed a reduction in the apparent Na+ affinity and changes in the voltage dependence and the kinetics of transient currents. In addition, sporadic HM mutations, K1003E (10) and Y1009X (23), have been reported. D999H and Y1009X have been described in families where there is also a co-occurrence of HM and epilepsy, suggesting that mutations in this region may represent susceptibility factors for HM and epilepsy.
In this family with FHM2 and epilepsy, the R1007W mutation is also present in individuals with migraine with and without aura, suggesting that ATP1A2 gene mutations might be implicated in the pathogenesis of most common forms of migraine. A single individual with the R1007W mutation had neither migraine nor epilepsy. This finding might be explained with low penetrance of ATP1A2 mutations, as previously described (6,24), and by their remarkable variability of phenotypic expression, depending on the genetic or environmental background (25). Previous studies have demonstrated a frequent association with ATP1A2 gene mutations and epilepsy (7,8,23). In the family we are describing, two individuals exhibited an epilepsy phenotype consistent with idiopathic syndromes with benign course, benign myoclonic epilepsy and benign rolandic epilepsy. Epilepsy is a common comorbidity of FHM, and has been previously reported both in FHM1 and FHM2. Vanmolkot and colleagues (8) reported a partial cosegregation of FHM2 and benign familial infantile seizures, but his data have not been confirmed in further studies (26), indicating epilepsy as a part of this phenotypic spectrum.
Our functional study of the R1007W mutant in Xenopus oocytes shows distinct changes in the voltage-dependent interactions with transported cations. The reduced amplitudes and K0.5[K+ext] values from Na+/K+ pump currents of the R1007W mutant within the range of physiological voltages (−70 mV to +20 mV) can explain a loss of function within a systemic context. The reduced K+ affinity and transport capacity would impair K+ clearance from the extracellular fluid, eventually causing hyperkalemia, a condition known to be a trigger for CSD and migraine (27). Altered voltage dependence with decreased apparent affinity for extracellular K+ at voltages around the resting potential of cells has not been observed in other electrophysiological studies on ATP1A2 mutations so far (11,15), thus the R1007W mutation adds a novel facet to the functional changes in FHM2. The R1007W mutation is located in the cytoplasmic C-terminal portion of α2-subunit (Figure 2(b, c)), and affects the most conserved within a cluster of two (human ATP1A2) or three (human ATP1A1) Arg residues that were initially suspected to act in voltage sensing (15). Morth and colleagues (15), studying pig ATP1A1, found no significant change in the voltage dependence of stationary pump currents on simultaneous mutation of all three arginines in ATP1A1 to alanine. Although no K0.5[K+ext] values were determined from pump currents in this study, the K0.5 values reported for the K+ dependence of ATPase activity were 0.669 mM for ATP1A1 WT and 0.843 mM for the RRR-AAA mutant (15). Although biochemical and electrophysiological results are not directly comparable, at least by trend these data are similar to the increased K0.5[K+ext] values of the R1007W mutant at 0 mV (1.67 ± 0.16 mM) compared to WT (1.10 ± 0.05 mM), indicating that mutation of the first conserved Arg is crucial for the effect.
The C-terminus of the Na+/K+–ATPase is important for enzyme function since it plays a role in the regulation of voltage dependence and affects the apparent cation affinities, with special emphasis on its stabilizing role for the third, unique Na+ binding site (11,15–19). Recent data have shown that the C-terminus is pivotal for a previously unrecognized cation translocation pathway (18) that interconnects the third Na+ binding site with the occlusion mechanism (17–19). Mutational interference with a network of interactions stabilizing the C-terminal structure, which involve the C-terminal tyrosines Tyr-1019 and Tyr-1020 as well as Arg-937 and Asp-999, was shown to induce Na+-dependent, mainly H+-carried “leak” currents occurring in the absence of extracellular K+ (16,17,19), which were related to a destabilization of cation occlusion (19). We did not observe such “leak” currents for mutant R1007W, in line with the notion that the side chain of Arg-1007 is not involved in the aforementioned network within the crystal structure. However, our analysis shows that the R1007W mutation modifies the voltage-dependent interactions of the ion pump with its cationic substrates. Such changes in kinetics of partial reactions or apparent cation affinity are frequently observed as a result of other, structurally unrelated mutations (11). Thus, although these effects do not necessarily prove an involvement of Arg-1007 in voltage sensing, they further highlight the fundamental importance of the α-subunit’s C-terminus for the ion transport mechanism.
Since ATP1A2 is mainly expressed in glia cells, it plays a vital role in the removal of extracellular K+, thus preventing depolarization of neurons under conditions of high neuronal activity. The Na+ and K+ gradients generated by the enzyme are also important for the reuptake of glutamate from synaptic space via the Na+/glutamate exchanger and for intracellular Ca2+ homeostasis through the Na+/Ca2+ exchanger. Thus, loss of Na+/K+–ATPase activity can lead to neuronal hyperexcitability and eventually facilitate seizures genesis as well as CSD that is typical for migraine. The α2-isoform of Na+/K+–ATPase has a different expression profile during development: It is present in neurons throughout the brain at birth, while in the adult is found only in astrocytes. This different developmental expression of the α2-isoform can explain the different clinical manifestations of ATP1A2 mutations throughout life: Very young patients could have infantile epilepsy caused by hyperexcitability of neurons (neuronal expression of mutated α2-isoform) and adults could develop HM because of the low threshold of CSD, linked to the expression of glial α2-isoform. All these functional data together with clinical evidence suggest that mutations in the FHM2 gene can determine a variable degree of epileptic susceptibility and also support the hypothesis that migraine and epilepsy are part of the same pathogenic mechanisms associated with genetically determined alterations of ion channels and pumps.
Our data also support the hypothesis that the novel mutation R1007W may be a susceptibility factor for idiopathic epilepsy, although its causative role in determining these syndromes needs to be corroborated by further studies.
Clinical implications
Familial hemiplegic migraine (FHM) and epilepsy with a new ATP1A2 mutation (R1007W). Functional study of mutation showed a loss of function not previously reported. FHM2 gene supports the hypothesis that migraine and epilepsy are part of the same pathogenic mechanisms associated with genetically determined alterations of ion channels and pumps.
Footnotes
Acknowledgments
The authors thank Ina Seuffert for technical assistance and Dr Neslihan Tavraz for valuable discussions.
Funding
TF and SS are supported by funding from the German Research Foundation (Cluster of Excellence “Unifying Concepts in Catalysis”).
Conflict of interest
None declared.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.