
Abstract
Objective
To evaluate long-term predictors of remission in patients with medication-overuse headache (MOH) by prospective cohort study.
Background
Knowledge regarding long-term predictors of MOH outcome is limited.
Methods
Two hundred and forty MOH patients recruited from 2000 to 2005 were included in a one-year follow-up study and then subsequently followed until 31 December 2013. The median follow-up was three years (interquartile range, three years). Predictive values of selected variables were assessed by the Cox proportional hazard regression model.
Results
At the end of follow-up, 102 (42.5%) patients were in remission. The most important predictors of remission were lower number of headache days per month before the one-year follow-up (HR-hazard ratio = 0.936, 95% confidence interval (CI) 0.884–0.990, p = 0.021) and efficient initial drug withdrawal (HR = 0.136, 95% CI 0.042–0.444, p = 0.001). Refractory MOH was observed in seven (2.9%) and MOH relapse in 131 patients (54.6%).
Conclusions
Outcome at the one-year follow-up is a reliable predictor of MOH long-term remission.
Introduction
In the general population, the prevalence of medication-overuse headache (MOH) is 1–2%, varying in different parts of the world from 0.5% to 7.2% (1). These patients comprise the majority of those treated in secondary and tertiary care centers due to headache, frequent headaches and reduced quality of life, as well as multiple treatment failures (2). A consensus regarding the best treatment for MOH has not yet been achieved. However, most headache experts regard withdrawal of the overused medications (3), with or without the administration of prophylactic medication, as the treatment of choice, as in most cases this leads to a decrease in headache frequency with discontinuation of the medication overused.
High relapse rate of MOH is the major treatment problem occurring, according to published studies, mainly within the first year or even during the first six months after analgesic discontinuation (4). Thus, the mean relapse rate is estimated to be 20–40% during the first year (5), and between 20–50% according to follow-up studies of longer duration (4–11). These values are even higher when MOH patients who failed to cease overuse are taken into account.
Knowledge regarding predictors of MOH outcome is limited, especially long-term data. Several studies have used gender, type of primary headache disorder, overused medication, and anxiety and depression scores at baseline as predictors of MOH long-term outcome (4,7–11). Previously, we performed a prospective study of MOH patients and analyzed clinical features predicting treatment outcome at one-year follow-up (12). The main findings of the study were a high relapse rate of 39.6% at first-year follow-up and independent predictors of treatment failure (frequency of primary headache disorder, ergotamine overuse and disability of chronic headache estimated by MIDAS) (12).
The aims of the present study were to evaluate the outcome in the same group of MOH patients previously included in the one-year follow-up study (12), and the potential long-term predictors of remission.
Patients and methods
We prospectively followed an initial cohort of 240 MOH patients recruited between January 2000 and July 2005 and diagnosed according to the Headache Classification (13). These patients had previously been included in a one-year follow-up study (12) and then subsequently followed by regular control examinations until 31 December 2013 (Figure 1).
CONSORT flow diagram of patient disposition.
Demographic data, the features of the chronic headache disorder, type and daily drug intake of overused medication(s) were obtained from headache diaries kept at least three months prior to recruitment. The diagnosis and features of the primary headache disorder, as well as age at headache onset were obtained from medical records. The collected features of the primary or chronic headache disorder frequency were expressed in days with headache during a month, intensity measured by VAS 0–10, daily headache duration expressed in hours, and disability assessed by MIDAS. Concomitant use of benzodiazepines and daily intake of caffeine (caffeine abuse was defined as daily intake of more than three cups of coffee), smoking and lack of physical activity, as well as positive family history for headaches were also recorded. To assess physical activities, study participants were asked if they did moderate activities for at least 10 minutes at a time, such as brisk walking, cycling, swimming, or any other activity that causes some increase in breathing or heart rate. Smokers were defined as persons who reported smoking every day during a 60-day period prior to completing the questionnaire.
The patients were treated in the Headache Center, Clinic of Neurology, Clinical Center of Serbia in Belgrade by in- or out-patient withdrawal of overused drug(s) and the simultaneous administration of headache prophylactics. The inclusion and exclusion criteria, as well as the treatment protocol provided in our Center were described in detail previously (12). All patients were instructed to keep headache diaries. The efficacy of treatment was assessed at follow-up after one year. A decrease in headache frequency ≥ 50% or return of headache features to the primary headache disorder associated with discontinuation of medication overuse, was considered an effective treatment. The results of the one-year follow-up were also included in the final analysis.
At each follow-up, days with headache during a month, intensity measured by VAS 0–10, disability measured by MIDAS; as well as relapses of MOH with type of overused medication(s), and treatment efficacy were recorded as the outcome measures. At the end follow-up performed for each patient, the actual headache diagnosis according to Headache Classification (14), days with headache during a month, and disability measured by MIDAS were noted.
This study was approved by the Institutional Review Board.
According to the results at the end follow-up, three possible outcomes were registered: Remission, relapse and refractory MOH disorder. Remission was defined if the patient was without chronic headache and without medication overuse, relapse as the presence of MOH in a patient who did not have MOH in the previous period. Finally, refractory MOH was defined as MOH without any improvement during the total follow-up. Follow-up time was calculated from the end of initial treatment.
Statistical analysis
Predictive values of selected variables were assessed by the Cox proportional hazard regression model, using the hazard ratio (HR) with 95% confidence intervals (CI) as the outcome measure. Additionally, we included continuous variables in the model without their dichotomization. Therefore, our predictive model demonstrated that one-unit increase in the value of certain variable resulted in increasing/decreasing HR for certain percentage over the studied period. In the Cox proportional hazard model analyses we defined the end of treatment as zero time. The end point time in this analysis was MOH remission. Univariate Cox regression analysis was used for testing the influence of different variables on the outcome of MOH in our study. As a final step, the variables that had reached significance at the 0.05 (alpha level) in the univariate analysis were further analyzed in the multivariate Cox proportional hazard regression model. The selected predictors are combined into a model by using the forward stepwise method. The data analyzed met the assumptions of the tests used to analyze them.
In the hypothesis testing, two-tailed directions were used. The SPSS 17.0 statistical software package (SPSS Inc, Chicago, IL, USA.) was used to perform the statistical analysis. A p < 0.05 was considered statistically significant.
Results
Baseline characteristics of 240 patients with MOH.

More than half of the patients, 132 (55.0%), were overusing one medication for acute migraine treatment, while the others overused two or more different compounds at a time. The most commonly overused agents were non-steroidal anti-inflammatory drugs, overused by 147 (61.3%), and combined analgesics by 147 (61.3%) patients. Ergotamines were overused by 55 (22.9%) patients, triptans by 21 (8.8%) and opioids by seven (2.9%). Fifty (20.8%) patients reported concomitant use of benzodiazepines. The mean number of tablets overused by a patient during a month was 53.9 ± 43.0 (range 15–300).
At the one-year follow-up, 137 (57.1%) patients were without chronic headache and without medication overuse, eight (3.3%) patients did not improve after withdrawal, and 95 (39.6%) relapsed, developing recurrent overuse within the first year following treatment.
Only 39 (16.3%) of patients were lost after the first-year follow-up, while 121 of them were followed for three years after treatment, and 33 (13.8%) of them were followed for ten years or more, some even for 13 years. The median follow-up was three years (interquartile range, three years). Figure 2 shows the distribution of the length of follow-up, expressed in years.
Percentages of MOH patients according to the duration of follow-up periods.
Variables extracted by univariate and multivariate analysis as predictors of MOH remission.

Hazard ratio, **95% confidence intervals, bold values denote statistical significance.
The probability of MOH remission is presented by Kaplan-Meier curve (Figure 3).
Probability of MOH remission.
Refractory MOH, i.e. without any improvement, was observed in seven (2.9%) patients at the end follow-up. This group included three (42.9%) women and four (57.1%) men with a mean MOH duration of 4.9 ± 2.3 years (range 2–8 years). Tension-type headache was the primary headache disorder in five (71.4%) patients and migraine in two (28.6%). Due to the small number of patients in this sub-group, we did not analyze predictive variables.
One hundred and thirty one (54.6%) patients had MOH relapse(s) during the follow-up period. This group consisted of 107 (81.7%) females and 24 (18.3%) males with a mean MOH duration of 5.7 ± 5.7 years (range 1–26 years). The primary headache disorder was migraine in 89 (67.9%) patients and tension-type headache in 42 (32.1%) patients. During the follow-up period, 131 patients experienced 160 MOH relapses. One hundred and ten patients (45.8%) experienced one relapse, 13 (5.4%) had two, and eight (3.3%) had three MOH relapses. The majority of MOH relapses, 95 (59.4% of all MOH relapses) occurred during the first year after treatment and were noted at the one-year follow-up. First MOH relapse occurred in 36 patients (15.0%) 3.86 ± 2.86 (range 2–12) years after treatment. The second relapse occurred in 21 (8.75%) patients 5.29 ± 3.05 (range 2–13) years after treatment and the third in eight (3.3%) patients 10.0 ± 2.14 (range 6–13) years after treatment. The time distribution of MOH relapses is shown in Figure 4.
Time distribution of MOH relapses.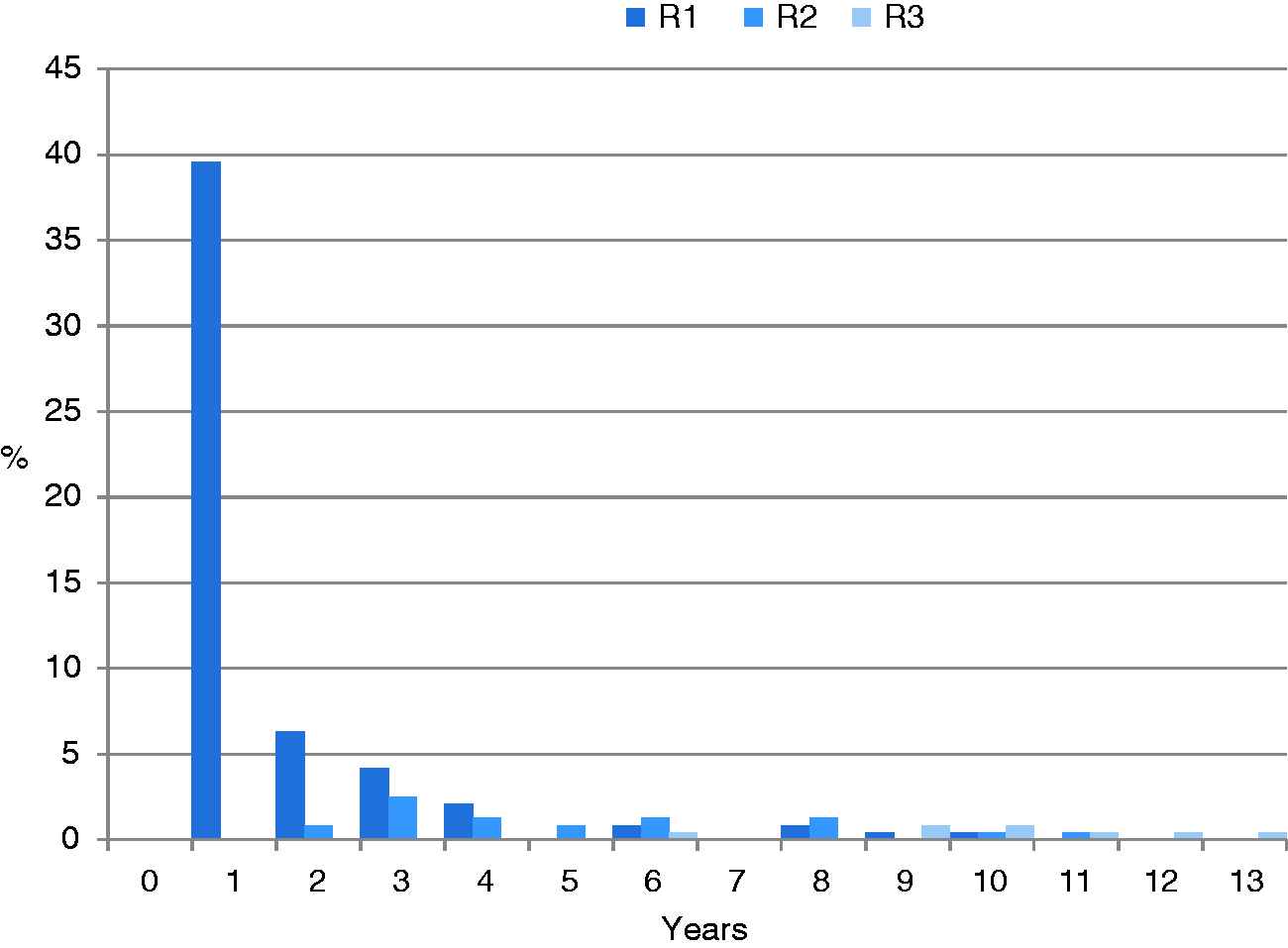
Medications overused in MOH relapses were the same as the medications overused at the time when the MOH diagnosis was established in the majority of MOH relapses, 134 (83.75%).
Discussion
This study analyzed long-term MOH outcome in a tertiary referral center, where a group of patients was treated in the same manner with overused drug withdrawal and prophylactic medication. The overall result of the study was that less than half of MOH patients had recovered without MOH recurrence at long-term follow-up. A high number of MOH sufferers, in spite of treatment attempts, make MOH the most disabling condition among the headache disorders. Although MOH was not part of the final analysis in the latest Global of Burden of Disease Study (15), the high prevalence of this disorder marked by the highest MIDAS scores (16) led to the assumption that MOH causes a highly significant number of years of life with disability (17,18).
The prediction of long-term outcome and determination of predictive factors could help to improve the treatment strategy for MOH patients, indicating particularly vulnerable groups with unfavorable outcomes.
The results of our study support the heterogeneity of the MOH population. Some authors, based on clinical experience and without firm pathophysiological correlates, divided MOH patients into two groups, simple and complicated (19). Patients with longer duration of the disorder, a high number of overused drugs, and the coexistence of psychiatric disorders, as well as a history of relapse after withdrawal are often treatment resistant (20). The relapse rate of MOH was high, recorded in 39.6% of patients at the one-year follow-up in our previous study (12). This is in accordance with the results of other studies, which estimated the occurrence of relapse to be 20–40% during the first year of detoxification (21–25). Long-term follow-up of our patients revealed that while the majority of patients had recurrence of MOH at one-year follow-up, some had multiple relapses during the subsequent course of the disorder, and MOH relapse could occur even 12 years after successful detoxification. The relapse rate of the examined group, at the end of the observational period, was 54.2%. Studies analyzing the outcome after at least four years estimated the relapse rate to be 20–50% (4–11). Overuse of the same drug in multiple MOH relapses, noted in more than 80% of our patients, could point to a hereditary susceptibility or dependence behavior, two still-debated issues in MOH pathogenesis (26).
Refractory MOH, i.e. MOH without any remission, was observed in almost 3% of our patients. The exact number of patients with refractory MOH is not known, since there are no studies specifically dealing with these patients. The patients with withdrawal failure are usually added to the patients with MOH relapses, and thus are included in the total number of patients with treatment failure in outcome studies. The current concept of refractory chronic migraine (27) excludes patients with medication overuse. The concept of refractory MOH has not yet been defined. All our patients were treated with discontinuation of the offending drug(s) and initiation of prophylactics. It has been shown that a multidisciplinary treatment approach with various pharmacological and non-pharmacological strategies and their combinations can improve the outcome of chronic primary headache disorders and MOH (28). Pain relief can be achieved by invasive or non-invasive neuromodulation approaches for patients with chronic cluster headache and chronic migraine (29). The efficacy of these methods has not been investigated in MOH patients, and it is possible that our “refractory” MOH patients could benefit from these treatments. Reduced activity in the right supramarginal gyrus and in the superior and inferior parietal cortex, and changes in pain perception caused by medication overuse, were noted in MOH patients (30,31). These changes are reversible and improve with discontinuation of overuse (30,31). We can only speculate that patients with refractory MOH have permanent damage to pain networks. It is worth noting that one patient who was not successfully detoxified during treatment and so was labeled as refractory MOH at one-year follow-up, spontaneously reduced headache frequency and drug intake during the subsequent course of the headache disorder. The positive effect of drug withdrawal during the course of the disorder, even without immediate MOH resolution, has also been demonstrated in other studies (5,11).
After treatment, 42.5% of our patients were without chronic headache and without medication overuse until the end follow-up. The predictors of a favorable outcome were a lower number of headache days per month before the one-year follow-up (p = 0.021) and efficient initial drug withdrawal (p = 0.021). According to our results, the outcome at one-year follow-up is a reliable indicator of the long-term outcome for patients who recover from MOH.
Possible limitations of the present study are worth noting. Firstly, the study was conducted in a tertiary care center and may reflect a selected headache population. In Serbia, the health-care organization of patients with headache enables self-registration of all patients, thus the patients treated in our Headache Center were not selected according to the burden of headache. The advantage of these circumstances is that MOH diagnosis is reliable, established by a headache expert after careful examination and necessary diagnostic procedures. The second limitation could be the unequal duration of follow-up periods, which we resolved by applying the Cox regression model for analysis. Thus, the results obtained in our study cannot be directly compared to the results of other long-term studies (32), regarding the proportion of patients with a particular duration of follow-up periods.
Recently, in headache chronification research, special attention has been paid to the fact that measurements of interest are imperfectly reliable and may be burdened by some measurement errors (33). This is especially true in survey research of headache frequency, because its quantification requires retrospection. Such retrospection is challenging to complete with accuracy, and can be influenced by a host of factors including intervening life events, affective distress, time since last headache, length of the actual retrospective period, and memory capacity. Difficulties also arise from the distinction between enumerating headache attacks vs. days wherein any headache pain was experienced. Due to these measurement limitations, headache frequency reporting is imperfectly reliable, but even more problematic when assessed in a study that has initially relied on extreme score selection and two measurement occasions. Finally, in headache chronification studies, there is a problem of degree of regression artifacts (regression to mean) (33).
In conclusion, our results support the notion that the outcome at the one-year follow-up is one of the most important elements for early detection of MOH patients susceptible to MOH recurrence. Therefore, these MOH patients should be recognized early, closely monitored and appropriately treated. However, the reduction of the probability of MOH remission over time could reflect biological difference in MOH patients compared to other chronic headache disorders.
Clinical implications
At the last follow-up, 102 (42.5%) patients were in remission, continuous MOH was noted in seven (2.9%) patients, and MOH relapses were observed in 131 (54.6%) patients. The most important long-term predictors of remission were the lower number of headache days per month before the one-year follow-up and efficient initial drug withdrawal. The majority of MOH relapses occurred during the first year after drug withdrawal, and were noted at the one-year follow-up; medications overused in MOH relapses were the same as the medications overused at the time when the MOH diagnosis was established in the majority of patients.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Ministry of Education, Science and Technological Development of the Republic of Serbia (grant numbers 175022 and 175087).