
Abstract
Background
Some patients with spontaneous intracranial hypotension have a ventral spinal cerebrospinal fluid (CSF) leak and these CSF leaks may be associated with calcified disk herniations. Identifying these calcifications is helpful in directing treatment. We report here the unusual case of a patient with a ventral CSF leak in whom the associated calcification absorbed over a five-month period.
Case report
A 42-year-old woman developed orthostatic headaches and bilateral abducens nerve palsies. Magnetic resonance imaging of her brain showed typical findings of spontaneous intracranial hypotension. Magnetic resonance imaging of her spine showed an extensive cervicothoracic CSF leak. Computed tomographic myelography showed calcification at the Th1–2 disk space. Three epidural blood patches were performed, but her symptoms persisted. Digital subtraction myelography performed five months later showed an upper thoracic ventral CSF, but the calcification was no longer present. A dural tear, found at surgery at the Th1–2 level, was repaired and the patient made an uneventful recovery.
Discussion
The resorption of calcifications at the level of a ventral spinal CSF leak could explain the absence of any calcifications in at least some patients with such leaks and demonstrates the usefulness of reviewing previous imaging in patients with ventral CSF leaks if the exact site of the leak remains unknown.
Introduction
Spontaneous intracranial hypotension is an important and increasingly recognized cause of secondary headache (1). Some patients with spontaneous intracranial hypotension have a ventral spinal cerebrospinal fluid (CSF) leak and these CSF leaks may be associated with calcified disk herniations or calcifications of the posterior longitudinal ligament (2–6). Such calcifications have been reported in up to two-thirds of patients with spontaneous intracranial hypotension (6). In patients with spontaneous intracranial hypotension that does not resolve with conventional epidural blood patching, identifying these calcifications is often helpful for directed treatment of the CSF leak, including directed epidural blood patching, percutaneous fibrin glue injections, and microsurgical repair of the dural tear (6).
We report here the unusual case of a patient with spontaneous intracranial hypotension and a ventral spinal CSF leak in whom the associated calcification absorbed over a five-month period prior to surgical intervention. Identification of the exact site of the dural tear was difficult using digital subtraction myelography (DSM), but a review of the previous post-myelogram computed tomography (CT) scan showing the calcification allowed surgery to proceed with confidence.
Case report
A 42-year-old woman reported the sudden onset of posterior neck pain and stiffness, nausea, and vomiting. There was no history of trauma. Twenty-four hours later she developed an orthostatic headache associated with light sensitivity, clogged hearing, and dysequilibrium. Two weeks later the patient noted the gradual onset of horizontal diplopia. The neurological examination was normal except for bilateral abducens nerve palsies. Magnetic resonance imaging (MRI) of her brain showed pachymeningeal enhancement, brain sagging, and pituitary enlargement (Figure 1). MRI of her spine showed an extrathecal, mainly ventral cervicothoracic collection of fluid. A lumbar epidural blood patch was performed and this resulted in a resolution of symptoms for 24 hours. CT myelography was then performed 10 weeks after the onset of symptoms and showed a ventral extrathecal collection of fluid extending from C5 to Th5. A midline calcification was also noted at the posterior edge of the Th1–2 disk space (Figure 2). Two further epidural blood patches (one thoracic and one lumbar) were performed, which resulted in the good, but incomplete, relief of symptoms. MRI of her spine showed a persistent ventral extrathecal collection of fluid. DSM was performed five months after the CT myelogram, but the exact site of the CSF leak could not be pinpointed. The first definite collection of extrathecal ventral contrast extended from Th1 to Th3. A ventral extrathecal CSF could again be demonstrated on the post-DSM CT, but the calcification at Th1–2 was no longer present (Figure 2).
(a) T1-weighted sagittal MRI scan showing brain sagging and pituitary enlargement. (b) Coronal T1-weighted gadolinium-enhanced MRI scan showing diffuse pachymeningeal enhancement. (a) Sagittal and (b) axial post-myelogram CT scans showing calcification at the Th1–2 level (arrows). (c) Sagittal and (d) axial post-DSM CT scans performed five months later showing the disappearance of the calcification. (e) Intraoperative photograph showing a 5 mm ventral dural defect.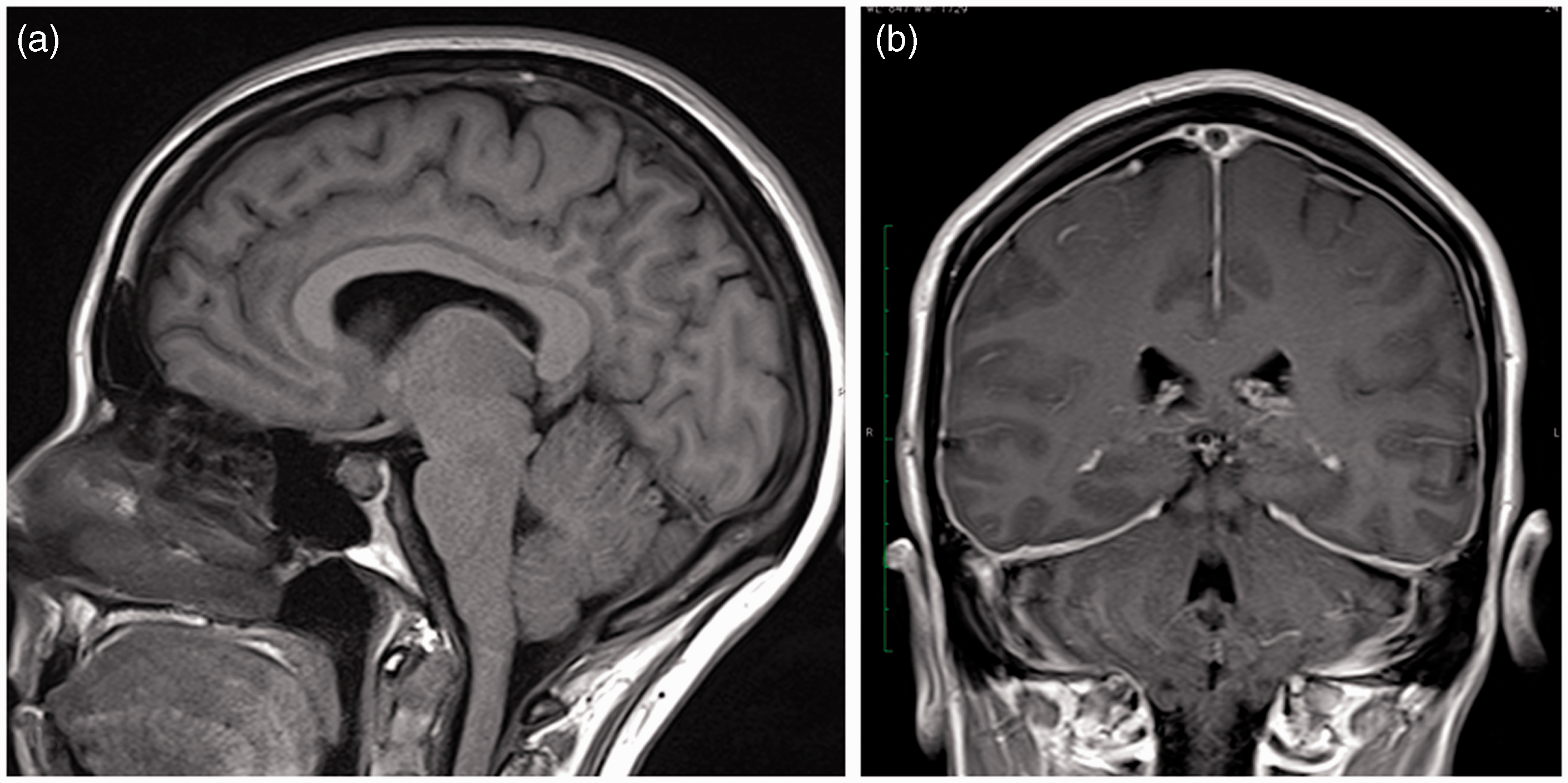

The patient underwent an uneventful Th1–2 laminectomy and, through a transdural posterior approach, a dural defect measuring about 5 mm was noted at the level of the Th1–2 disk space (Figure 2). Because of the midline location of the dural defect, suturing of the dural tear was not performed, but an autologous muscle graft was placed within the dural defect. The patient recovered well from the surgery with complete resolution of symptoms. MRI examination of her brain and spine showed complete resolution of the previously noted abnormalities. The patient has remained symptom-free during four months of follow-up.
Discussion
Ventral spinal CSF leaks have a propensity to become chronic and these CSF leaks have been reported to be the underlying cause of a wide variety of neurological syndromes, including superficial siderosis, spontaneous spinal cord herniation, an amyotrophic lateral sclerosis-like syndrome (bibrachial amyotrophy), and diffuse non-aneurysmal intracranial subarachnoid hemorrhage (7–10). The anatomical location of the dural tear in patients with ventral spinal CSF leaks is almost always at the level of the disk space, although calcified lesions are certainly not always visualized at the site of the CSF leak (4,6,7). Spontaneous resolution of calcified disk herniations much larger than those seen in this patient has been described previously (11–13). The pathophysiology of the spontaneous regression of calcified disk herniations is poorly understood, but may involve an inflammatory response and pulsatile CSF flow (11–13). Such an inflammatory process in combination with pulsatile CSF flow may be more robust in patients with a ventral spinal CSF leak because of the presence of CSF in contact with the calcified disk herniation. Spontaneous resolution of the calcified fragments of the relatively small size seen in our patient – as frequently found in other patients with ventral spinal CSF leaks – may be a relatively common occurrence, possibly explaining the absence of any calcified lesions at the level of the dural tear in a significant number of patients with ventral spinal CSF leaks.
The detection of calcifications associated with ventral spinal CSF leaks may be crucial in confidently identifying the exact site of the dural tear. Reviewing the initial post-myelography CT scan showing the calcification was particularly useful in this patient because DSM was unable to exactly pinpoint the site of the dural tear. A potential limitation of DSM is that visualization of the contrast material may be impaired at the cervicothoracic junction because of the density of the shoulders (3).
Clinical implications
Ventral spinal cerebrospinal leaks may be associated with calcifications, generally at the level of the disk space. These calcifications are important to recognize because they can guide directed treatment for the cerebrospinal leak. These calcifications may resolve spontaneously, making directed treatment more difficult and possibly explaining the absence of any calcifications among patients with chronic ventral spinal cerebrospinal leaks.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.