
Abstract
Objectives
Few studies have addressed central sensitization symptoms and pain processing in childhood migraine. Our aims were to examine pain sensitivity and responses, including habituation, evoked by CO2 laser stimuli (laser-evoked potentials (LEPs)) in a cohort of children with migraine compared to non-migraine controls and to determine the correlation between LEP features and signs of central sensitization.
Methods
Thirty-five patients 8–15 years of age with migraines without aura were evaluated during the inter-critical phase and were compared to 17 controls. LEPs were analyzed, and their main features were correlated with clinical symptoms including allodynia and pericranial tenderness.
Results
The laser-evoked pain threshold was lower and the N2P2 vertex complex amplitude was higher in children with migraines. Furthermore, habituation of vertex waves of LEPs clearly showed a tendency toward progressive amplitude enhancement in the migraine group. Acute allodynia and inter-critical pericranial tenderness correlated with trigeminal LEP features, particularly with the abnormal habituation pattern.
Discussion
Abnormalities of pain processing and symptoms of central sensitization appear to be characteristics of children with migraine. Reduced habituation and progressive amplification of cortical responses to laser stimuli indicate an overactive nociceptive system at the onset of migraine, and this hyperactivity may subtend allodynia and pericranial tenderness. Future prospective trials may aid in the early identification of clinical phenotypes that display a tendency to develop into the chronic form of migraine, warranting a timely therapeutic approach.
Introduction
Migraine is a disabling disorder of neurovascular origin. Abnormal neuronal excitability, largely based on genetic factors, is a predisposing factor for the onset of migraine attacks (1). Although juvenile migraine may represent a model to test the early phase of the disease, few studies have addressed nociceptive system function in childhood in general or specifically in children with migraine. Reduced habituation to multimodal repetitive non-nociceptive stimuli was observed in childhood migraine (2,3). This pattern of reduced habituation to nociceptive stimuli may favor the increase in pain and the phenomenon of central sensitization. Allodynia, a frequent and incapacitating symptom of migraine attack (4), has never been evaluated in children, although the enhanced expression of symptoms of central sensitization may indicate a possible unfavorable outcome (5,6). The few studies reported on pericranial tenderness in children with migraine confirmed a low pressure pain threshold at pericranial sites (7), which is also a sign of persistent trigeminal and cervical nociceptive neuronal activation, supporting evolution into the chronic form (8). The early detection of symptoms of central sensitization at the onset of migraine, as well as the study of nociceptive pathway function at juvenile age, may improve the understanding of the mechanisms of migraine and the prevention of its evolution into the chronic form. Previous studies performed on the trigeminal reflexes showed abnormal function of the trigeminal system immediately at the onset of migraine attacks and even in pre-symptomatic migraines (9,10). Reduced habituation of the nociceptive trigeminal reflex response was found to be an endophenotypic marker of migraine that is also detectable in asymptomatic first-degree relatives of patients with migraine (10). Blink reflex abnormalities as an early appearance of the ultra-late R3 component suggested a dysfunction of the inhibitory control system in the trigeminal networks of juvenile patients with migraine (9). In a P300 odd ball paradigm where normal and migraine children had to respond to rare targets (tones) and ignore frequent painful or non-painful mechanical standard stimuli, migraine patients exhibited larger P300 amplitudes at significantly shorter latencies in response to both low- and high-intensity mechanical stimuli, suggesting an attentional bias toward real or potential pain (11). Important data about pain processing in adult patients with migraine were obtained from the application of evoked responses to the selective stimulation of nociceptive afferents.
Laser-evoked potentials (LEPs) are a useful tool to examine the function of nociceptive pathways due to their high selectivity for a-delta and C fibers (12). In adult migraine, responses obtained stimulating a-delta fibers were found to increase in amplitude during the attack, with a tendency toward reduced habituation during both the acute and inter-critical phases (13–16). The few studies about LEPs in infancy suggested increased amplitudes of N2P2 vertex complex in normal children compared to healthy adults; this result was interpreted as a sign of incomplete maturation of thermoalgesic system sensory processing (17). The first aim of our study was to examine pain sensitivity and responses including habituation at somatic and trigeminal sites evoked by CO2 laser stimuli in a cohort of children with migraine compared to age- and sex-matched non-migraine controls. The second aim was to determine the correlation between LEP features and the clinical profile of migraine, including signs of central sensitization such as allodynia and pericranial tenderness.
Methods
Cases
Demographic and clinical features in migraine children and controls. No significant difference was detectable between patients and controls in regard to age and sex. The two sides Student’s t test for equal variance and the Chi square were employed.
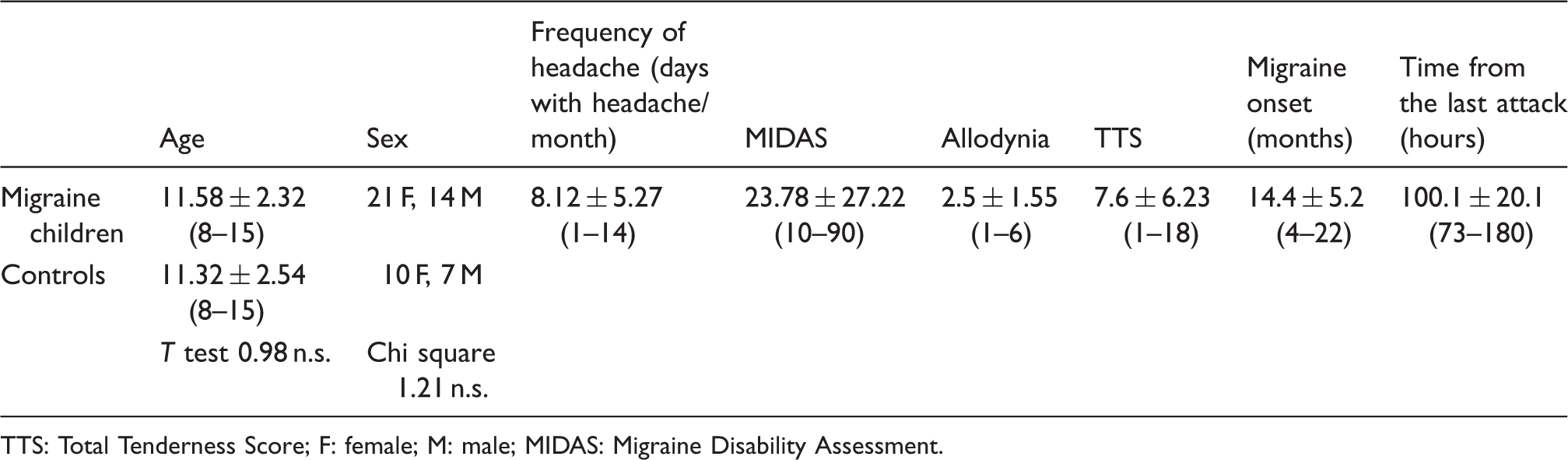
TTS: Total Tenderness Score; F: female; M: male; MIDAS: Migraine Disability Assessment.
Procedure
Clinical assessment
All migraine patients and their parents were carefully interviewed by neurological and psychological staff at their first visit to our center. A second appointment was then scheduled for the neurophysiological assessment at least one month after the first visit, during which the mothers were requested to complete the allodynia questionnaire for each migraine attack (19). The allodynia questionnaire is not presently adapted for children, so we suggested the parents sign “not applicable” on questions specific to adults. Then, the average score for different attacks was considered. The frequency of headache was computed at the moment of the neurophysiologic procedure as the average number of days with headache in the last three months. At the same time, in all young patients, the Migraine Disability Assessment (MIDAS) score on the childhood version of the test was applied (20), and pericranial tenderness was evaluated (21,22). Recordings were performed during the interictal phase, at least 72 hours after the most recent attack and 48 hours before the next one, as ascertained by a telephonic interview.
LEP stimulation procedure
The pain stimulus consisted of laser pulses (wavelength 10.6 lm) that were generated by a CO2 laser (Neurolas Electronic Engineering, Florence, Italy). The stimulation site was visualized using an He–Ne laser beam. After each stimulation, the laser beam was slightly shifted to a nearby site to avoid nociceptor sensitization and skin damage.
The diameter of the laser beam was 2.5 mm, and the duration of the stimulus pulse was 30 ms. To define the pain threshold, single stimulus pulses were presented in a random order at four to five different intensities at 1.5 W intervals. The participants were requested to report the quality of the sensation and the pain threshold, which was expressed as the laser intensity (expressed in Watts) that produced a pinprick sensation followed by a burning sensation. Thirty consecutive laser stimuli were then delivered to any stimulation site at an intensity level set one step (1.5 W) above the pain threshold at an inter-stimulus interval of 10 seconds. We evaluated LEP habituation within single trials (13) in accordance with previous studies to minimize exam duration and distress. The dorsum of the right hand and the right supraorbital zone were stimulated in all patients and controls. The order of site stimulation was randomized across participants. The patients were requested to rate the laser pain intensity at the end of the stimulation series according to a 0–100 visual analog scale (VAS) in which 100 represented maximal pain, shown in an intense red color.
Recording procedure
Each individual was seated in a comfortable position in a quiet room with an ambient temperature of 21–23℃ in an awake and relaxed state with eyes open. All participants and observers wore protective goggles during data acquisition. The children were always recorded in the presence of the mother.
In addition to the 19 standard positions of the international 10–20 system, 37 electrodes were placed on the x, y, and z coordinates instructed by Advanced Source Analysis (ASA) software (ASA version 4.7; ANT Software, Enschede, The Netherlands; http://www.antneuro.com). The reference electrode was placed on the nose, the ground electrode was in Fpz, and one electrode was placed above the right eyebrow for electro-oculographic (EOG) recording. Impedance was maintained at 10 kΩ or less. The electroencephalogram (EEG) and EOG signals were amplified using a bandpass filter of 0.5–80 Hz, digitized at 250 Hz, and stored on a biopotential analyzer (Micromed System Plus; Micromed, Mogliano, Veneto, Italy; www.micromed-it.com).
In the present study, we examined waves obtained from the Cz position of the 10–20 International System (impedance below 5000 Ω), referred to the nasion, and those obtained from T3 derivation, referred to the Fz position, with the ground electrode at Fpz (12).
LEP analysis
An investigator who was blinded to the clinical condition analyzed the LEP recordings of one second, including 100 ms of pre-stimulus time, at a sampling rate of 256 Hz. All LEP recordings containing transient signals that exceeded 65 mV in any recording channel were excluded from the average by an automatic artifact rejection algorithm. Other artifacts were visually inspected. For each stimulation site, we evaluated the averages of at least 21 valid (artifact-free) responses. The LEPs were identified on the basis of their latency and distribution; three responses (N1, N2 and P2) were labeled according to the procedure of Valeriani et al. (23). The N1 component was analyzed at T3 Fz, and the N2 and P2 components were analyzed at the vertex (Cz-nasion) (12,23). The absolute latencies of the scalp potentials were measured at the highest peak of each response component. The amplitude of each wave was measured from the baseline, which was measured automatically by calculating the average signal on the entire sweep and subtracting this average signal from the trace (ASA v.4.6 by ANT software; Advanced Neuro Technology, Enschede, The Netherlands). The peak-to-peak amplitude was taken into consideration for the vertex biphasic LEP component (N2–P2). To assess N2P2 habituation, we decided to consider only the initial and final block of single responses, considering that in adult migraine the trend of LEPs amplitude changes is quite irregular in the course of the stimulation, while reduced habituation is expressed by the lack of significant amplitude modification between the first and the last responses (14). We simplified the habituation pattern computing the percentage difference between the LEP amplitudes obtained in the first and third blocks of the averaged responses relative to the first block (first response-third response × 100/first response). This value was defined as the habituation index (HI).
Statistical analysis
The two-tailed Student’s t test assuming unequal variances was performed to compare the LEP features between the patient and control groups. The p values used for statistical significance in this analysis was a two-sided alpha of 0.05, without adjustment for multiplicity. The Pearson test was used to evaluate the correlations between the main clinical data and the LEP features in the migraine group.
Results
Clinical features
The clinical features of the children with migraine are reported in Table 1. For all included participants, the allodynia questionnaire was efficaciously completed for at least two attacks. All children with migraine reported at least one allodynia symptom during their migraine attacks, whereas pericranial tenderness varied from total absence (in four cases) to clear presence (score of 18 in one case). The frequency of headache was also quite variable, ranging from 1.5 to 15 days with headache/month (Table 1).
Laser pain threshold and evoked responses
Laser-evoked potentials features in migraine patients and controls (mean and standard deviations): Results of Student’s t test for independent data are reported.

PT: pain threshold; VAS: visual analog scale; Hab: habituation index (first response-third response × 100 /first response).

Grand average of laser-evoked potentials (LEPs) across 17 non-migraine (black track) and 35 children with migraine without aura (blue track) obtained via stimulation of the right hand and the right supraorbital zone.

Grand average of the first (black track) and the third (blue track) blocks of laser-evoked potentials (LEPs) obtained from migraine patients and controls.

Box blots of the habituation index in migraine patients (MIG, n = 35) and controls (CON, n = 17).
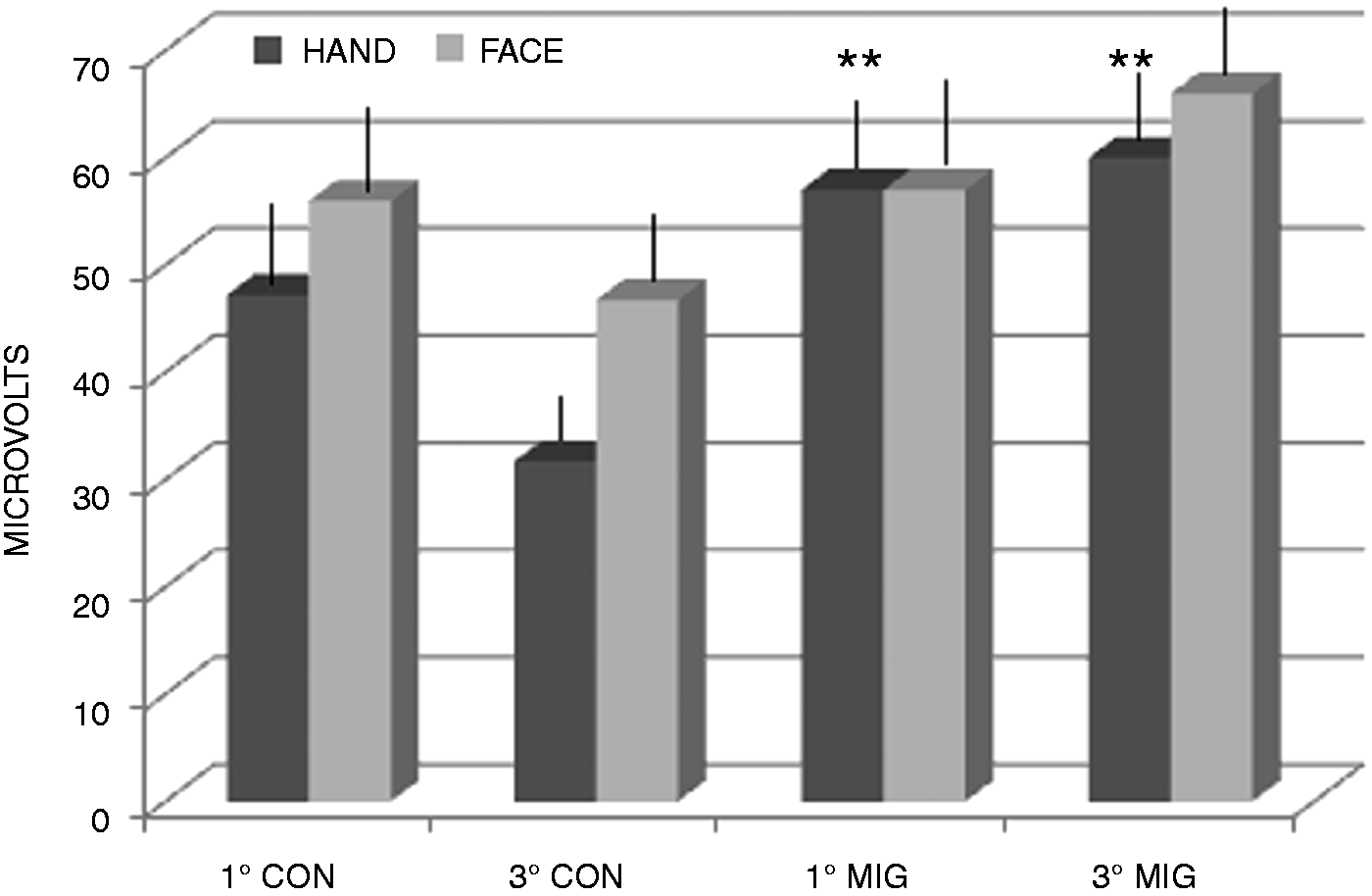
Mean values and standard errors of the N2P2 amplitude obtained for the first and third blocks of averaged laser-evoked responses among the control participants (CON, n = 17) and migraine patients (MIG, n = 35). The first and third blocks of LEP responses were compared between the two groups, and the results of the Student’s t test were reported as follows: **p < 0.01.
Regarding the correlation of various characteristics, we considered statistical significance only above a p value of 0.01 to correct for the high number of statistical comparisons. Aside from the expected positive correlation between the MIDAS score and the frequency of headache (r 0.572, p < 0.01
The trigeminal HI correlated with the severity of acute allodynia (r 0.800, p < 0.01). In addition, children with larger trigeminal vertex LEPs more frequently experienced migraines (r 0.486, p < 0.01) and exhibited more severe pericranial tenderness (r 0.584, p < 0.01).
Discussion
This study employed for the first time laser-evoked responses to examine the nociceptive system in children with migraine. Our results indicated that children with migraine exhibited a lower pain threshold, at least at the hand level, with the same tendency at the trigeminal level. The somatic N2P2 vertex complex was significantly increased, with a similar trend at the trigeminal level. In addition, LEP vertex waves showed a progressive amplitude enhancement in most of the migraineurs, in contrast to the reduction observed in the controls. Acute allodynia and inter-critical pericranial tenderness, which were detected in our children with migraine, correlated with the trigeminal LEP amplitudes and an abnormal habituation pattern.
Clinical symptoms of central sensitization in children with migraine
Few studies related to the symptoms of central sensitization in childhood headache are available. In our migraine cohort, pericranial tenderness was present in the most cases, in accordance with previous reports (7). Considering its correlation with MIDAS scores, it is a symptom that may correlate with migraine severity, characterizing children with an over-active trigeminal nociceptive system, as suggested by its positive correlation with the vertex N2P2 amplitude following supraorbital stimulation (see below). To the best of our knowledge, allodynia was not previously evaluated in childhood migraine. Its assessment is presently limited to the use of a questionnaire validated in adult migraine, although many items may be adapted to children (24). Other limitations include the compliance of the mothers and their influence on the interpretation of the symptoms of migraine attacks. Considering all of these aspects, children with migraine appeared to experience at least one allodynia symptom during migraine attacks, confirming that acute central sensitization is an intrinsic feature of the disorder, which is even more evident at developmental age than at adult age. In fact, in a large cohort of adults with primary headache, allodynia was reported in approximately 70% of episodic migraine and 90% of chronic migraine sufferers (4,6,25). Although the present data require further confirmation in larger samples, the clear correlation between allodynia and amplification, not habituation, of trigeminal LEPs may suggest that hyperactivity of the trigeminal nociceptive system may support the clinical symptoms of central sensitization (see below).
Laser pain threshold and sensitivity
Although the LEP pain threshold must be cautiously considered because of age-related variability (26), a lower pain threshold emerged at the hand level in children with migraine, although no significant difference was observed at the trigeminal level. In a previous study performing quantitative sensory testing (QST) on children with migraine, the mechanical pain threshold was reduced, whereas the heat threshold was within normal limits (27). In the same study, the pain threshold changed in relation to sex and the presence of the mother; specifically, the pain threshold was lower among females and was higher when the mother attended the experimental session. The small sample did not enable us to perform reliable comparisons between sexes, but our impression is that the reliability of the subjective evaluation of pain intensity by young people is questionable (26,28–30). Nevertheless, the reduced pain threshold detected at the hand level in young migraineurs, regardless of migraine severity and headache duration, may confirm early changes in the nociceptive system that are potentially intrinsic to migraine. The variability in maturational changes in the nociceptive system, as well as the variability in subjective judgment, may be higher at the face level (9), explaining the lack of a significant difference in the low trigeminal pain threshold between children with migraine and controls. Moreover, pressure pain, more so than heat pain, may be related to persistent pericranial tenderness, a sign of central sensitization, according to recent studies of children suffering from migraine (7) and tension-type headache (31).
LEP features
The amplitudes and latencies of the N2 and P2 vertex waves in the controls resembled the few available results in normal children (17). To the best of our knowledge, the early N1 component has not previously been evaluated in normal children. Considering the adult ranges observed by our laboratory (32), the present data suggest that this component also exhibited an age-related increase in amplitude, especially for trigeminal stimulation. Maturational changes in LEPs do not appear to involve latency modification (17); thus, the earlier appearance of N2 in response to hand stimulation in children with migraine may be subtended by a generalized facilitation of the somatosensory nociceptive system, potentially representing an intrinsic feature of migraine. The non-nociceptive somatosensory system appeared to be hyperexcitable in childhood migraine both at the cortical and sub-cortical levels (33). The possible variability in the trigeminal nociceptive system during normal development may also account for the lack of a significant difference in the trigeminal LEP latency between children with migraine and controls. Moreover, the inclusion of controls with possible subsequent migraine appearance cannot be excluded, which is a real limitation in studies of juvenile age unless prospective observation is performed. The N2P2 complex amplitude was also increased in migraine children to a significant extent at the hand level, further supporting the possible early dysfunction of nociceptive pathways in this disorder. The LEP vertex complex represents the activation of cortical zones devoted to the arousal response to and the salience detection of pain stimuli (34,35), and its amplitude was found to be increased in adult migraineurs, especially during the critical phase, both for trigeminal and hand stimulation (13,15). Interestingly, in our children with migraine, the trigeminal N2P2 amplitude, which was not significantly different compared to that of the controls, positively correlated with headache frequency and pericranial tenderness but was independent of migraine duration. This result may be explained by the existence of clinical phenotypes resulting from an overactive trigeminal system and a predisposition to central sensitization and severe migraine outcome. The relationship between trigeminal pain-related responses amplitude and headache frequency is also in agreement with functional magnetic resonance imaging (fMRI) studies conducted in adult migraineurs, describing a cycling behavior of the spinal trigeminal nuclei over the migraine interval, with higher level of activation in proximity of attacks (36).
The most apparent abnormality observed in children with migraine was the lack of a progressive reduction in LEP amplitude. Habituation is a physiological phenomenon that occurs during multimodal sensory processing, which contrasts with the tendency toward a progressive increase in neuronal activation, e.g. sensitization (1,3,37). Reduced habituation of multimodal sensory and cognitive processing is a characteristic of childhood migraine that unfortunately predicts an unfavorable migraine outcome (38). An abnormal pattern of habituation in the trigeminal nociceptive system is an endophenotypic marker of migraine (10), suggesting that the nociceptive system is prone to sensitization even before the clinical appearance of migraine. In adult migraine, we found that vertex cortical responses to laser-nociceptive stimuli did not habituate during either the interictal or the ictal phase and that this abnormal habituation pattern correlated with migraine attack severity (15,16). In normal children, we found that although the N2P2 amplitude in response to hand stimulation progressively reduced from the first to the last repetition by approximately 30%, at the trigeminal level, the habituation rate was limited to an average reduction of approximately 18%; this result may be a sign of sustained cortical activity in response to noxious face stimuli, which is also observed in healthy adults (16). Children with migraine exhibited an opposite tendency toward a progressive increase, rather than a decrease, in the N2P2 amplitude both at the somatic and trigeminal sites, confirming that reduced habituation is an endogenous trait of migraine (10), and this characteristic may be more evident at the developmental age. In fact, children with migraine showed a phenomenon of progressive amplification, rather than suppression, of cortical waves, which was less evident in adults with migraine (14,16). In accordance with previous findings concerning adult migraine (14–16), we did not detect a reduction in the N2P2 amplitude between the first and third blocks in children with migraine. This phenomenon, which has frequently been described for multi-modal non-nociceptive-evoked responses, has been attributed to a state of low cortical pre-activation (39). A peculiar mode of functioning in a persistent state of overactivation may thus characterize pain-related cortical zones even at the onset of migraine disorder. Moreover, our migraine group displayed variability between cases, ranging from slight habituation both at the somatic and trigeminal levels to clear vertex wave amplification. Although this variability was observed also in adult migraine (16), in children this may be further influenced by misdiagnosis with tension-type headache (30), in which the LEP habituation pattern appears to be normal (16). Another limitation of studies addressing childhood migraine may be the clinical evolution of aura symptoms, which, at the moment of study inclusion, were not sufficiently frequent to support an adjunctive diagnosis of migraine with aura. In previous studies, adults affected by migraine with aura exhibited a reduced tendency toward central sensitization symptoms (25,22). Thus, the possible existence of different pain processing phenotypes represents the topic for further studies in groups of children, including those with both types of migraine.
The correlation between trigeminal LEP amplification and allodynia confirms that the absence of compensatory mechanisms limiting the progressive increase in neuronal activation in response to sensory and particularly nociceptive stimuli may produce symptoms of central sensitization during migraine attacks. This result may support our impression that central sensitization symptoms are intrinsic to migraine, as they are evident at migraine onset, and correlate with nociceptive trigeminal system dysfunction.
Basing on present findings, specific mechanisms underlying central sensitization phenomena may be supposed in childhood migraine. Enhanced N2P2 amplitude by hand stimulation may be explained by sensitization at the thalamic level, which is involved in the phenomenon of extracephalic allodynia (40). The LEPs reduced habituation and even facilitation in the course of repetitive noxious stimulation, may be favored by a dysfunction of cortical zones regulating the endogenous pain control, as suggested by fMRI studies performed during long-term pain habituation trials (19).
Conclusions
Abnormalities of pain processing appear to be characteristic of children with migraine. Reduced habituation and progressive amplification of cortical responses to laser stimuli indicate an overactive nociceptive system immediately at the onset of migraine; these characteristics may subtend symptoms of central sensitization such as allodynia and pericranial tenderness. Variability in symptoms of central sensitization and in LEP abnormalities within the migraine group suggests the presence of clinical phenotypes with an early predisposition to develop the chronic form of migraine. Challenges for future studies include the early identification of such cases in prospective trials to customize a timely therapeutic approach.
Clinical implications
The early detection of symptoms of central sensitization at the onset of migraine, as well as the study of nociceptive pathway function at juvenile age, may improve the understanding of the mechanisms of migraine and the prevention of the evolution into the chronic form. Reduced habituation and progressive amplification of cortical responses to laser-evoked stimuli indicate an overactive nociceptive system at the onset of migraine, and these characteristics may subtend allodynia and pericranial tenderness.
Footnotes
Acknowledgement
Authors’ contributions are as follows:
Marina de Tommaso: study design and coordination and manuscript preparation; Vittorio Sciruicchio: clinical assessment and manuscript preparation’ Katia Ricci, Anna Montemurno, and Francesco Gentile: laser-evoked potential recording and analysis; Eleonora Vecchio: clinical assessment of patients; Maria Grazia Foschino, Michele Simeoni, Marvita Goffredo: psychological assessment of patients; Paolo Livrea: manuscript editing.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by Bari University Research Funds.