
Abstract
Background
Headache is the medical problem most commonly observed by neurologists. Non-pharmacological treatments are commonly demanded by individuals with headaches, but their evidence of effectiveness is conflicting.
Aim
The current review provides an updated discussion on what is supported by current scientific evidence about physical therapies for tension-type headache (TTH), migraine, and cervicogenic headache (CeH), and which gaps there still may be in our understanding of the interventions.
Methods
PubMed, MEDLINE, EMBASE, AMED, CINAHL, EBSCO, Cochrane Database of Systematic Reviews, Cochrane Collaboration Trials Register, PEDro, and SCOPUS were searched from their inception through March 2015.
Results/Discussion
Several physical therapies including spinal joint manipulation/mobilization, soft tissue interventions, therapeutic exercises and needling therapies are proposed to be effective for the management of headaches. Current evidence has shown that the effectiveness of these interventions will depend on proper clinical reasoning since not all interventions are equally effective for all headache pain conditions. For instance, evidence of physical therapy in migraine is more controversial than in TTH, since migraine pathogenesis involves activation of sub-cortical structures and the trigemino-vascular system, whereas pathogenesis of TTH is more associated with musculoskeletal disorders, e.g. muscle pain. It seems that multimodal approaches including different interventions are more effective for patients with TTH, migraine and CeH.
Keywords
Introduction
In the 21st century, headache is probably the most common medical problem observed in practice by neurologists, causes substantial pain and disability and is associated with a high burden and considerable cost (1). In fact, the cost computed in Europe in 2010 was €13.8 billion for headaches (2). Among headaches, migraine and tension-type headache (TTH) are the most common primary headaches, whereas cervicogenic headache (CeH) is one of the most common secondary headaches seen in clinical practice. Stovner et al. found that around 46% of the general population exhibits an active headache disorder and that headache is included within the 10 most disabling conditions for the World Health Organization (WHO) ranking of causes of disability (3).
Several therapeutic approaches are proposed for the management of these headaches, with pharmacological drugs, physical therapies, and cognitive/behavioral therapies being the most used. In fact, different studies revealed that alternative medicine therapies are the most used treatments requested by individuals with headaches (4,5). The existence of a wide range of therapies without clear clinical effectiveness can be, in part, consequence of an inconclusive understanding of the underlying pathophysiology of headaches. Furthermore, clinical and scientific evidence supports that proper management of patients with headache should be multimodal including appropriate use of pharmacological (i.e. acute/abortive and preventive drugs) and non-pharmacological (i.e. manual therapies, exercises, biofeedback, and needling therapies) interventions (6). Therefore, the challenge facing clinicians is to select the most proper treatment approach for each patient with headache. In fact, effectiveness of physical therapy is different on each headache; for instance, evidence in migraine is more controversial than in TTH since migraine pathogenesis involves the activation of sub-cortical structures as well as the trigemino-vascular system, whereas the pathogenesis of TTH is more associated with musculoskeletal disorders, e.g. muscle pain. It seems that individuals exhibiting neck musculoskeletal impairments, comorbid anxiety or mood states, problems for managing stress, significant headache-related disability or medication overuse may particularly benefit from these non-pharmacologic approaches (7,8).
Non-pharmacological therapies are generally included in clinical guidelines. The European Federation of Neurological Societies (EFNS) guideline has concluded that non-pharmacologic therapies should be considered in the management of patients with TTH, although their scientific basis is limited (9). Similarly, the Italian guideline for primary headaches reported that non-pharmacological techniques are a valid complementary treatment for headache patients, particularly indicated in cases of pregnancy, breast feeding, multiple therapies for comorbid diseases, poor tolerability of drugs, childhood and old age (10).
The current paper will discuss scientific evidence for the application of different physical therapies in TTH, migraine, and CeH based on a clinical rationale of nociceptive pain mechanisms. For that purpose, literature searches were performed on the following databases: PubMed, MEDLINE, EMBASE, AMED, CINAHL, EBSCO, PEDro, Cochrane Database of Systematic Reviews, Cochrane Collaboration Trials Register, and SCOPUS from their inception to March 1, 2015.
Effectiveness of spinal manipulation/mobilization in headaches
Among the different manual therapies proposed for headaches, cervical manipulation or mobilization are the most commonly used by physical therapists (11). Joint manipulation is defined as high-velocity, low-amplitude movement delivered at the end of restricted joint motion and within the normal anatomical range of motion (Figure 1), while joint mobilization is defined as a low-velocity, high-amplitude movement delivered at the end of the available restricted joint motion and within the normal anatomical range of motion (Figure 2). Spinal manipulation/mobilizations mainly target musculoskeletal disorders in the head/neck present in headaches (12). In fact, the rationale for application of manual therapies targeting the cervical spine in individuals with headache is that neck pain is present in almost all patients and is associated with higher peri-cranial tenderness in adults with migraine and TTH (13), and with headache unresponsive to analgesics in adolescents (14).
Upper cervical spine manipulation. The therapist uses the manipulative hand to localize the targeted segment (C1/C2) in rotation, and uses the hand to perform a high-velocity, low-amplitude technique directed up toward the patient’s contra-lateral eye. Posterior-anterior upper cervical spine joint mobilization. The thumbs of the therapist make contact over the C1/C2 zygapophyseal joint and a posterior-anterior glide is applied.

Scientific evidence of spinal manipulation/mobilization in headache is conflicting. The old Cochrane Review found that spinal manipulation showed: 1) no evidence of effectiveness for TTH; 2) weak evidence of short-term effectiveness for migraine; and 3) weak evidence for CeH (15). Other systematic reviews have also concluded that there was insufficient evidence to support or refute the efficacy of spinal manipulation in TTH (16,17). A more recent review has concluded that spinal manipulation may be effective when combined with pharmacological therapy for TTH, although evidence is inconclusive (18). Evidence on migraine is also conflicting. Posadzki and Ernst concluded that evidence does not support the use of spinal manipulation as an isolated intervention for migraine (19), whereas Chaibi et al. found that spinal manipulation and massage might be equally effective as propranolol and topiramate in the prophylactic management of migraine attacks (20). Discrepancies between conclusions of these reviews can be related to the fact that the methodological quality of randomized clinical trials analyzing the effects of manipulation/mobilization for headaches is low (21). Otherwise, spinal joint manipulation/mobilization may be not equally effective for all headaches (22). In fact, it seems more effective for CeH than for other headaches. A recent systematic review found six randomized controlled trials suggesting that spinal manipulation is more effective than gentle massage, drug therapy, or no intervention at all in patients with CeH (23). Racicki et al. also concluded that spinal manipulative therapy was effective for reducing the pain in CeH (24).
Nevertheless, an important limitation of spinal joint manipulation/mobilization studies included in previous systematic reviews (15–20) is that information on which specific spinal manipulation/mobilization technique was used, targeted level (upper, middle or lower cervical spine) applied by clinicians, and the direction of the manipulative intervention is lacking. In addition, most of the included trials combined the application of spinal manipulation with joint mobilization. For instance, in the highest-quality randomized controlled trial conducted on CeH, therapists applied cervical manipulation and/or mobilization at their discretion based on clinical findings (25). Moreover, in some studies spinal manipulation/mobilization techniques were combined with soft tissue interventions. Therefore, it is not possible to date to determine the real effect of either spinal manipulation or mobilization for the management of headaches.
Another relevant issue is that the use of spinal joint manipulations targeted to the upper cervical spine remains controversial because of the concerns about their safety (26). Adverse reactions to spinal manipulative therapy range from minor events consisting of stiffness, pain and limitation in range of motion (26), to more serious events such as permanent neurological deficits and dissection of carotid or vertebral arteries (27). If all contraindications and red flags are ruled out, there is potential for a clinician to prevent 44.8% of adverse events associated with upper cervical spinal manipulation; nevertheless, 10.4% of the adverse events, mostly minor events, are unpreventable so that cervical spine manipulation carries an inherent risk even after a thorough evaluation (28).
Spinal manipulation/mobilization would probably be effective when proper clinical reasoning is applied and the targeted tissue is appropriate. For instance, it is expected that spinal joint manipulation/mobilization would be effective for CeH because this headache is considered a referred pain elicited by nociceptive stimulation of upper cervical joints (C1–C3). Accordingly, individuals with proven painful disorders of upper cervical zygapophyseal joints may exhibit significant relief of the headache with treatment directed at cervical pain generators (29). On the contrary, since the pathogenesis of TTH is based on myofascial pain disorders (30), it would be expected that spinal joint manipulation would not be as effective as in CeH. Nevertheless, this hypothesis needs further clarification.
Effectiveness of soft tissue therapies in headaches
Soft tissue therapies such as compression (Figure 3) or strokes (Figure 4) have also been suggested to be effective for TTH pain. In such scenarios, the role of myofascial trigger points (TrP) in headaches, particularly TTH, is advocated (30). A previous review found no evidence that soft tissue manual therapies have a positive effect on the evolution of TTH (31); however, a more recent review has concluded that the efficacy of physical therapy including soft tissue interventions equals the efficacy of tricyclic antidepressants, although further studies are required to confirm this assumption (32).
Manual compression applied on upper trapezius muscle trigger point. Manual stroke addressing trigger points in the sternocleidomastoid muscle. The therapist’s fingers grasp the taut band from both sides with a pincer palpation, and stroke centrifugally away from the trigger point.

Some studies reported that multimodal manual therapies, including soft tissue therapy, were effective in reducing pain in chronic TTH (33–35). The only randomized controlled trial assessing the efficacy of TrP therapy for TTH found that patients receiving massage targeting active TrPs exhibited greater reduction in headache intensity and sensitivity than those receiving a placebo intervention (36). Nevertheless, a recent review has concluded that no single manual therapy is more effective than another and that effectiveness of manual therapies in general cannot be completely assessed owing to the heterogeneity in study designs, outcome measures, and different interventions (37). This conclusion has been partially refuted by the first meta-analysis on manual therapies in TTH. This meta-analysis concluded that multimodal manual therapies were more effective than pharmacological drugs for reducing frequency (weighted mean difference (WMD), −0.8036; 95% confidence interval (CI), −1.66 to −0.44), intensity (WMD, −0.5974; 95% CI, −0.8875 to −0.3073) and duration (WMD, −0.5558; 95% CI, −0.9124 to −0.1992) of the headache immediately after treatment, although there were no differences in the long term (38). Discrepancies between this meta-analysis and previous reviews can be related to the fact that former reviews included studies with several comparison groups whereas this meta-analysis considered pharmacological care only as a comparative treatment. In addition, even though manual therapies included in this meta-analysis were diverse, all of them shared common fundamentals: cervical joint manipulation and/or mobilization combined with soft tissue interventions and/or exercises (38). The combination of these interventions is justified by current theories supporting a potential role of different musculoskeletal disorders in TTH (39–41). This may explain why previous systematic reviews investigating the effectiveness of isolated interventions, i.e. spinal manipulation (15–24), did not reach firm conclusions.
The role of soft tissues has been also investigated in CeH, but to a lesser extent. One case report found that treatment of sternocleidomastoid muscle TrPs was effective for CeH (42). A randomized clinical study showed that manual therapy targeted to sternocleidomastoid muscle TrPs was effective for improving headache intensity in CeH (43). A recent systematic review has concluded that manual therapies targeted to either muscle or joints of the upper cervical spine might be an effective treatment for CeH, but this conclusion should be considered with caution since studies mostly included patients with infrequent CeH (44). It seems that patients with CeH will also benefit from a combination of different manual therapies targeting different tissues (45). Again, it would be important to identify the particular headache to determine where soft tissue interventions would be more effective.
Effectiveness of therapeutic exercise in headaches
Another therapy approach that is clinically used in the management of headaches is exercise (46). We will discuss the application of both aerobic exercise and the application of local exercises targeting specific musculoskeletal disorders within the cervical spine. It seems that exercise-induced hypoalgesia is related to activation of descending inhibitory pathways (47). This is in line with authors suggesting that clinical management of headache patients needs to extend beyond local tissue-based pathology by incorporating strategies directed at normalizing central nervous system excitability (48). However, as several potential pathogenic mechanisms are involved in headaches, the most appropriate therapeutic exercise program might differ in each one (49). Therefore, it is particularly relevant to consider that therapeutic exercise may be effective in TTH, CeH and migraine, but the kind of exercise is different. For instance, aerobic exercise would be the best option in migraine prophylaxis, whereas specific neck and shoulder exercises would be a better choice for TTH and CeH (50). This hypothesis is supported by the fact that inclusion of cranio-cervical flexion exercises was effective in reducing the frequency, intensity and duration of headache (51) and the fact that neck flexor musculature endurance mediates 24.5% of the effect of manual therapy in patients with TTH (52). Actually, a recent review concluded that therapeutic exercise is a safe treatment that provides beneficial effects in TTH (53). This is similar in CeH, where the application of muscle endurance and strength training exercises targeting the deep cervical flexor muscles was more effective than stretching exercises for reducing the pain (54). A recent Cochrane Review concluded that there is moderate quality evidence supporting cervico-scapulo-thoracic strengthening and endurance exercises for improving pain and function in patients with CeH, although further studies are needed (55). Therefore it is proposed that therapeutic exercise programs consisting of reeducation of the deep neck flexors (Figure 5) should be incorporated into the management of TTH and CeH.
Therapeutic exercise consisting of cranio-cervical flexion exercise targeting the deep neck flexor muscles.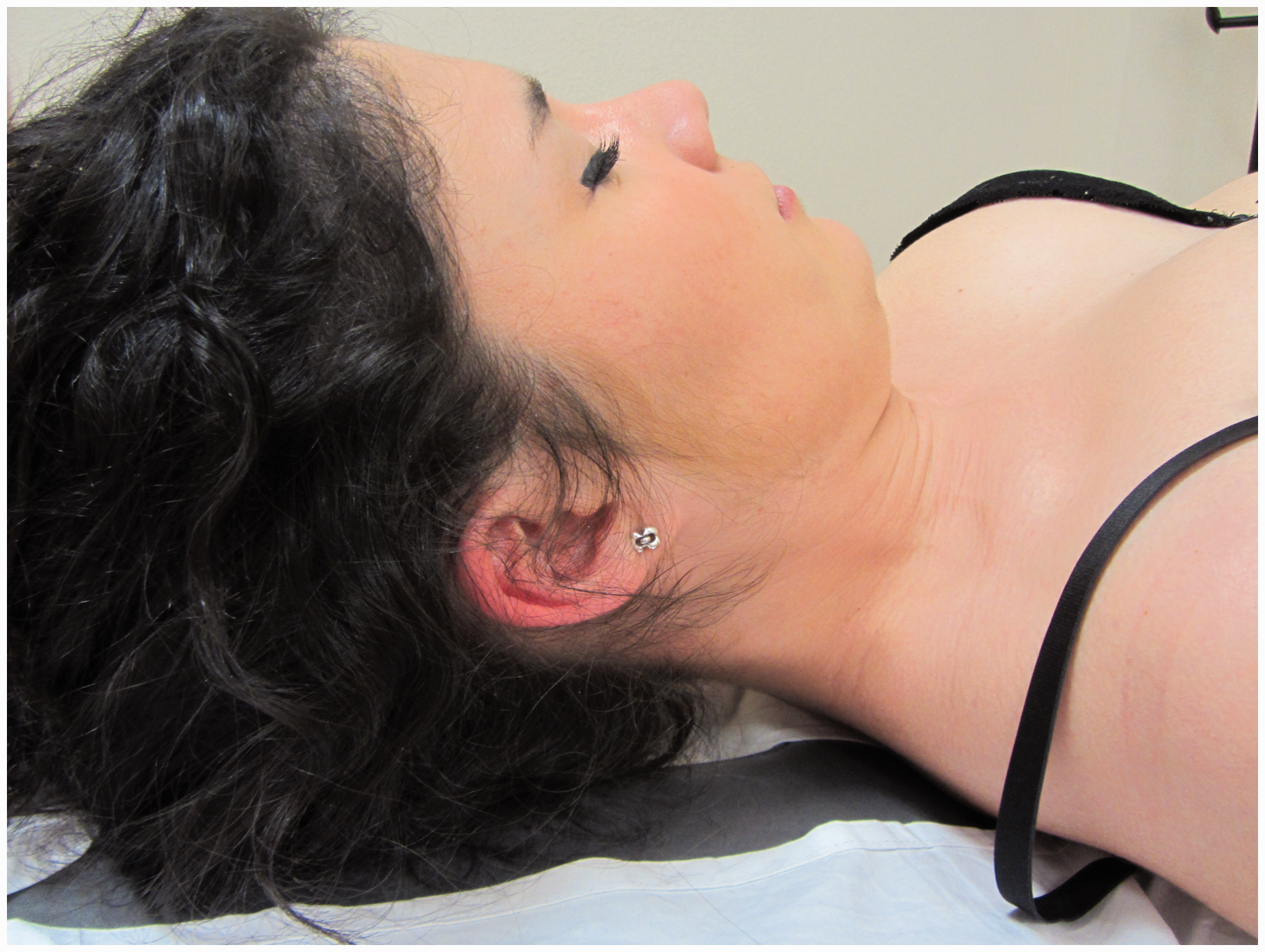
The role of exercise in migraine is highly controversial. The hypothesis is that exercise activates endogenous neurotransmitter signals that could be effective in reducing the intensity of migraine pain, though it may not have a direct effect on its overall frequency or duration (56). This theory is supported by a recent study showing that aerobic exercise influenced central information processing leading to clinical effects on migraine attacks (57). However, conclusions from systematic reviews are conflicting. A previous systematic review did not find a significant reduction of migraine frequency or duration but only indicated a reduction of pain intensity in individuals with migraine under regular exercise (58). In contrast, a recent review concluded that therapeutic exercise is clearly effective on migraine (53). Although no consensus exists about exercise and migraine, some authors suggest that aerobic exercise may be an option for the prophylactic treatment of migraine in individuals who do not benefit from or do not want to take daily drug medication (59). A recent review concluded that considering its effectiveness and safety, individuals with migraine should be encouraged to practice physical exercise with controlled intensity, frequency and duration to achieve the most beneficial outcome while preventing potential injuries and side effects (60). To determine the proper dose of exercise is highly relevant since prolonged or high-intensity exercise could precipitate migraine attacks in some patients.
Two important issues about therapeutic exercise are adherence and self-reported satisfaction. Gaul et al. found that adherence to lifestyle modifications, including proper and regular practice of exercise, predicted effectiveness of a multidisciplinary therapeutic program in TTH and migraine (61). These authors reported an adherence of 72% to aerobic endurance sports (61). Furthermore, physical training was chosen as preferable to pharmacologic treatment for the improvement of central nervous system-related symptoms and subjective well-being in TTH (62). In conclusion, exercise programs should be incorporated into multimodal therapeutic approaches for the management of headache patients, although proper exercises should be carefully selected based on proper clinical reasoning.
Effectiveness of needling therapies in headaches
Different needling therapies are currently used for the management of patients with TTH and migraine, and both acupuncture and TrP dry needling are the most commonly applied by physical therapists (63). The Cochrane review concluded that acupuncture could be a valuable tool in frequent episodic or chronic TTH (64). Likewise, the Cochrane review stated that there is consistent evidence showing that acupuncture provides additional benefit for the acute treatment of migraine attacks and is at least as effective as prophylactic drug treatment, causing fewer adverse effects (65). Nevertheless, other reviews have achieved more conflicting results. A meta-analysis found that acupuncture was able to reduce the number of headaches per month in the short term (WMD, −2.93; 95% CI, −7.49 to −1.64) and long term (WMD, −1.83; 95% CI, −3.01 to −0.64) compared to sham acupuncture (66). On the contrary, a more recent review showed no statistical significance between real and sham acupuncture (WMD: −0.31, −0.72 to 0.09) for the management of TTH (67).
Dry needling is used for inactivating myofascial TrPs in headaches (Figure 6). The main difference between acupuncture and dry needling is that this last technique inserts the needle on TrPs, and not in standardized acupuncture points. Although the literature suggests that dry needling may be a useful addition to physical therapy for the management of headache pain, further research with stronger methodological design is clearly required (68).
Dry needling applied over trigger points in the upper trapezius muscle.
Other physical therapy modalities
Other physical therapy modalities including biofeedback or transcutaneous electrical nerve stimulation (TENS) have also been assessed in patients with headache. The application of biofeedback is recommended in several European guidelines for the management of TTH and migraine (9,10). A review concluded that biofeedback exhibited medium to large effect sizes for the management of TTH and migraine for decreasing headache frequency (69). These results have been confirmed by two meta-analyses concluding that biofeedback is effective for reducing the intensity and frequency of the headache in the short and long term compared to headache monitoring or placebo in individuals with TTH and migraine (70,71). Since the objective of biofeedback is to teach the patients to decrease muscle tension in those activities that they associate with headache, this therapeutic option would be most effective in those patients whose headaches are precipitated by muscle tension. Relaxation and cognitive-behavioral interventions are also used for the management of headache. Although a systematic review found that cognitive-behavioral therapy may be better than no treatment, waiting list or placebo, no firm conclusions can be reached thus far (72).
Finally, the effectiveness of TENS has also been investigated in patients with chronic TTH (73,74), CeH (75,76), and migraine (77). Although these studies suggest that TENS may be a good alternative therapeutic option for headaches, their poor methodological rigor limits the conclusions that can be drawn at this time (78).
Conclusions
This paper summarizes updated data on physical therapy management for individuals with TTH, migraine and CeH. Appropriate therapeutic management of these patients should be multimodal and based on clinical neuro-physiological findings. It should target both peripheral and central sensitization mechanisms by including different physical therapy modalities.
Clinical implications
Several physical therapies including spinal joint manipulation and/or mobilization, soft tissue interventions, therapeutic exercises and needling therapies are proposed to be effective for the management of headaches. Current evidence has shown that the effectiveness of these interventions will depend on proper clinical reasoning since not all interventions are equally effective for all headache pain conditions. Multimodal approaches including different interventions seem to be more effective for patients with headache.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.