
Abstract
Background and objectives
The pathophysiology of tension-type headache is not well understood. Increased peripheral levels of pro-inflammatory cytokines may act as mediators of several chronic pain disorders. The aim of the present study was to investigate the peripheral levels of chemokines in patients with tension-type headache.
Methods
This was a cross sectional study evaluating serum levels of chemokines in age and sex-matched tension-type headache patients, ictally and interictally, and control participants. Beck Depression and Anxiety Inventories were recorded. Serum levels of monocyte chemoattractant protein-1, macrophage inflammatory protein 1α, regulated on activation, normal T cell expressed and secreted, eotaxin, eotaxin-2, interleukin-8, interferon gamma induced protein-10 were measured by enzyme-linked immunosorbent assay.
Results
A total of 96 participants (48 tension-type headache, 48 controls) were included. Interleukin-8 levels were significantly increased in patients with tension-type headache when compared to controls (413.8 (123.4–1756.3) and 329 (107.8–955.6), respectively, P = 0.025). Anxiety and depression scores were higher in patients with tension-type headache but interleukin-8 increase in tension-type headache patients persisted after controlling for anxiety and depression symptoms. Patients with headache at the time of assessment had increased monocyte chemoattractant protein-1 levels when compared with patients without headache (2809.3 (1101–6122.2) and 1630.2 (669.3–31056.8), respectively P = 0.026). Patients with episodic and chronic tension-type headache had no significant differences in serum chemokines levels.
Conclusion
Interleukin-8 was increased in tension-type headache and monocyte chemoattractant protein-1 was higher in tension-type headache patients with headache, suggesting that pro-inflammatory mechanisms may participate in tension-type headache pathophysiology.
Keywords
Introduction
Tension-type headache (TTH) is the most frequent form of headache; however, little is known about its physiopathology (1). Both peripheral and central mechanisms have been implicated. Increased myofascial pain sensitivity occurs in patients with TTH and peripheral sensitization of myofascial nociceptors may have a role in this process. Sensitization of second-order neurons at dorsal horn/trigeminal nucleus and supraspinal neurons at thalamus and somatosensory cortex have also been proposed to explain central increased pain sensitivity in TTH (2,3). Inflammation may be implicated in generating and maintaining pain in peripheral structures and can also promote sensitization of central nervous system structures involved in nociception (4). Therefore, it is reasonable to hypothesize that inflammation may play a role in peripheral and central sensitization in patients with TTH.
Previous studies have investigated the peripheral levels of inflammatory mediators in patients with TTH. Increased levels of interleukin-6 (IL-6) were found in patients with both episodic and chronic TTH (10), being higher in chronic than in episodic TTH. Interleukin-1 beta and interleukin-18 levels were shown to be increased in chronic TTH (11). These data suggest that inflammation participates in TTH pathogenesis. TTH has been associated with psychiatric comorbidities, including depression (5) and anxiety disorders (6). Such disorders have been previously associated with increased expression of pro-inflammatory mediators as well, including cytokines and chemokines (7–9). No study to date has evaluated whether the increase of pro-inflammatory cytokines in TTH could be secondary to psychiatric comorbidities.
Chemokines are a family of small (8–10 kDa) proteins that can induce chemotaxis of inflammatory cells to sites of inflammation and their activation. The family is composed of about 50 related molecules. According to the number and spacing of cysteine residues, four chemokines subfamilies have been identified: CC; CXC; C; CX3C. CC chemokines, the largest group, are characterized by the presence of two adjacent cysteine residues near the N-terminus and CXC is the second largest group and presents a single amino acid between the first two cysteine residues (12). No previous study has evaluated chemokines in patients with TTH.
The aims of the current study were two-fold: (i) to compare the serum chemokine levels between TTH patients and healthy controls; (ii) to investigate whether chemokine levels in TTH could be influenced by psychiatric comorbidities such as depression and anxiety.
Methods
Patients and procedures
This was a cross-sectional study including patients with TTH and healthy controls. From June to September, 2011, 48 patients with TTH, enrolled from the headache clinic of the Santa Casa de Misericórdia Hospital, Vitória, Brazil, were recruited during their first visit to the clinic. A headache expert neurologist evaluated all patients and the diagnoses were performed in accordance with the International Classification on Headache Disorders – 2nd edition (13). All the patients were asked about the presence of headache pain at the time of the evaluation and they were included irrespective of their pain status (i.e. ictal or interictal pain state). Control subjects were recruited in waiting rooms at the same outpatient clinic by an active search carried out among accompanying subjects. Forty-eight age- and gender-matched healthy subjects with no history of previous primary headaches were included in the control group. The minimal age for the inclusion of patients and control subjects was 18 years. Subjects with inflammatory, infectious, allergic, autoimmune, hepatic, neurodegenerative and neoplasic diseases were not included in the study, as well as pregnant women and people in use of corticosteroids or immunosuppressive drugs. This study received full approval by the Ethics Committee on Research of the ‘Escola Superior de Ciências da Santa Casa de Vitória’, Vitória, Brazil and informed consent was obtained from each participant.
Demographic (age, body mass index (BMI), race and marital status) and headache features (time of disease, frequency of attacks in the last month) data were recorded. Anxiety was evaluated with the Beck Anxiety Inventory (BAI) (14) and depression with the Beck Depression Inventory (BDI) (15). The anxiety symptoms were classified as mild (BAI 8–15), moderate (BAI 16–25) and severe (BAI > 25) (14). The depressive symptoms were classified as minimal (BDI 0–9), mild (BDI 10–18), moderate (BDI 19–29) and severe (BDI 30–63) (15).
Chemokines assessment
List of names and abbreviations of measured chemokines.

Statistical analysis
The data were analysed with SPSS, version 15.0 for Windows. The confidence interval was 95% and the significance level was set at P < 0.05. Verification of normal distribution of data was performed using the Kolmogorov–Smirnov test. Mann–Whitney was used for the medians comparisons of continuous data. Demographic categorical characteristics were compared using chi-square analyses. Binary logistic regression analysis was performed with the presence of TTH and the type of TTH as the dependent variables.
Results
Clinical and demographic data of subjects with tension type headache (TTH) and controls.

P: Mann–Whitney test, BMI: body mass index; BAI: Beck Anxiety Inventory; BDI: Beck Depression Inventory; HIT-6: headache impact test.
Patients with TTH had higher median BDI (P = 0.041) and median BAI (P = 0.014) when compared with controls. Four (8.3%) TTH patients had moderate to severe and 44 (91.7%) had no or mild anxiety symptoms. Forty-three TTH patients had minimal to mild (89.6%) and 5 (10.4%) had moderate to severe depression symptoms according to BDI score.
All the assays were above the limit detection for each chemokine except one control subject and one TTH patient for RANTES measure. By univariate analysis a significant difference in IL-8 levels was found between TTH patients and controls (P = 0.039) (Figure 1). Eotaxin, eotaxin-2, IP-10, MCP-1, MIP-1α and RANTES levels were not significantly different between TTH patients and controls (P = 1, 1, 0.081, 0.153 and 0.540, respectively) (Table 3). After controlling for anxiety and depressive symptoms, IL-8 levels remained significantly higher in patients with TTH when compared with controls (P = 0.025). There were no significant differences in chemokines levels when TTH patients were categorized according to the severity of anxiety and depressive symptoms. We performed the same analysis after excluding male subjects (three controls and three patients) and the results remained the same. Female TTH patients had significantly higher IL-8 levels than female controls, even after adjusting for depression and anxiety (P = 0.021).
Comparison of interleukin-8 (IL-8) levels between tension-type headache (TTH) patients (n = 48) and controls (n = 48). Chemokines levels in patients with tension type-headache (TTH) and controls. P: Mann–Whitney test; P*: binary logistic regression analysis with adjusted for depression and anxiety scores; MCP-1: monocyte chemoattractant protein-1; MIP-1α: macrophage inflammatory protein 1α; RANTES: regulated on activation, normal T cell expressed and secreted; IL-8: interleukin-8; IP-10: interferon gamma induced protein 10.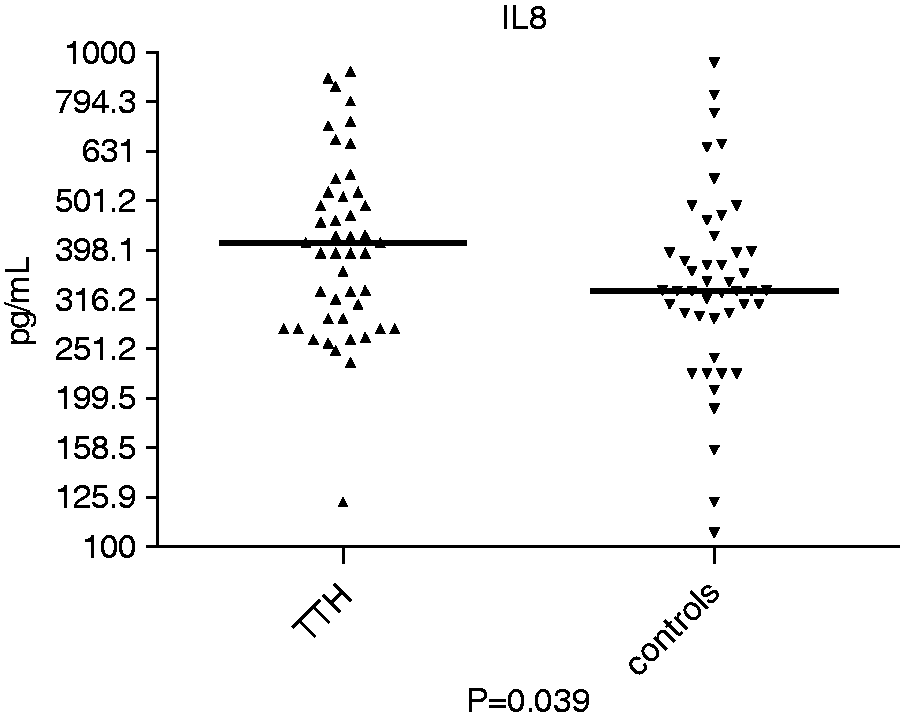

Forty-two (87.5%) out of 48 patients with TTH were classified as having episodic TTH and six (12.5%) as having chronic TTH. Patients with chronic TTH were older (median age 62.5 years, ranging from 47 to 74 years) than patients with episodic TTH (median age 35.5 years, ranging from 19 to 76 years), but there were no significant differences in ethnicity, gender and marital status groups in patients with episodic and chronic TTH (P = 0.359, 0.289, and 0.592, respectively). By univariate analysis the levels of eotaxin were higher in patients with chronic TTH (1261.33 pg/mL, 923.11–2073.56 pg/mL) than patients with episodic TTH (716.83 pg/mL, 163.84–1260.02 pg/mL) (P = 0.029). MCP-1 levels were also higher in chronic TTH (3917.38 pg/mL, 2540.99–6122.25 pg/mL) than in episodic TTH (1706.18 pg/mL, 669.35–31056.79 pg/mL) (P = 0.029). After adjusted analysis with binary logistic regression with age as covariate, there were no significant differences in eotaxin and MCP-1 levels between patients with episodic and chronic TTH (P = 0.682 and 0.349, respectively).
Patients with headache at the time of assessment had significantly higher MCP-1 levels (2809.3 pg/mL, 1101.05–6122.25 pg/mL) than TTH patients without pain (1630.22 pg/mL, 669.35–31056.78 pg/mL) (P = 0.026) (Figure 2). This difference was no longer observed after excluding male patients from the analysis (P = 0.137). No other chemokine (eotaxin, P = 0.112; eotaxin-2, P = 0.751; IL-8, P = 0.895; IP-10, P = 0.751; MIP-1α, P = 0.751; RANTES, P = 0.895) as well as no other clinical parameter (including age, headache impact test (HIT)-6, allodynia, number of headache days per month, BAI and BDI) was associated with the presence of pain.
Comparison of CCL2/monocyte chemoattractant protein-1 (MCP-1) levels between tension-type headache (TTH) patients with (n = 14) and without (n = 34) headache pain.
Discussion
To the best of our knowledge this is the first study to show elevated IL-8 serum levels in patients with TTH. IL-8 is a chemokine produced by macrophages and other cell types exposed to different inflammatory stimuli. IL-8 promotes the preferential accumulation of neutrophils in the sites of inflammation. The pro-inflammatory role of this chemokine has been shown in several pathological conditions (17). This finding is in line with a previous study that demonstrated elevated serum IL-6 levels in patients with TTH (10). It has been shown that inflammation may enhance nociceptive signalling by affecting peripheral nerve and neuronal excitability (18). One possible explanation of the finding of increased IL-8 in TTH outside a headache attack may be related with the interaction between stress and inflammatory response. Emotional conflict and stress are commonly reported in association with TTH (3). Recurrent or chronic stress may alter the functioning of the hypothalamic-pituitary-adrenal axis, thus enhancing pro-inflammatory responses. There is considerable evidence showing that increased production of inflammatory biomarkers occurs in stress response and this may be identified even in the prodromal stage of neuropsychiatric disorders (19). Therefore, the interictal increase in IL-8 could be part of a stress response. This hypothesis requires further confirmation.
Elevated eotaxin and MCP-1 levels were found in patients with chronic TTH; however, this difference was not significant after adjusted analysis. It is possible that the small number of patients with chronic TTH precluded demonstrating significant differences. Increased pro-inflammatory cytokines were previously shown in patients with chronic TTH (11) and in patients with other types of chronic primary headaches, such as chronic migraine and new daily persistent headache (20). The up regulation of pro-inflammatory cytokines may be implicated in neuroplastic changes of nociceptive circuits, thus contributing to the chronification of primary headaches. However, the relationship between chemokines and TTH chronification remains to be determined.
MCP-1 was increased in patients with headache at the time of clinical assessment. The association between pro-inflammatory cytokines and headache attacks has been explored (21). An increase of IL-6, interleukin-10 and RANTES was previously shown in migraine attacks (22). Bo et al. found increased MCP-1 in cerebrospinal (CSF) fluid samples of patients with TTH and migraine attacks (23). In the same study, an ictal increase of CSF interleukin-1 receptor antagonist and transforming growth factor-1β, both anti-inflammatory molecules, was shown. All these findings indicate that mild ictal immune/inflammatory changes occur in primary headache disorders. One possible hypothesis for the ictal increase of pro-inflammatory molecules in TTH is that miofascial pain triggers the release of inflammatory mediators leading to the excitation of peripheral afferent nerves. Nevertheless, this hypothesis is unlikely since ‘normal’ levels of inflammatory mediators were found in tender trapezius muscle in patients with chronic TTH (24). An alternative explanation is that peripheral stimuli could activate the spinoreticulothalamic tract that extends rostrally to the hypothalamus, resulting in the release of multiple circulating molecules such as corticotropin-releasing hormone, vasopressin, beta-endorphin and adrenocorticotrophic hormone, which stimulate cortisol production that may activate peripheral leukocytes and the release of cytokines (25). This hypothesis is in line with a previous study suggesting that cytokine increase during headache attacks may represent a mild response to pain (23).
Anxiety and depression symptoms were higher in patients with TTH. There is growing evidence that anxiety and depression can lead to increased production of pro-inflammatory cytokines (7–9). However, in the present study, TTH patients with moderate and severe anxiety and depression scores had no increase in chemokine levels as compared with patients with mild anxiety and depression scores. Moreover, anxiety and depression symptoms did not influence the increased levels of IL-8 that showed to be independently associated with TTH.
This study has limitations. This is a cross-sectional study not allowing the establishment of any causal assumption. The small number of patients with CTTH does not allow definite conclusions regarding whether chemokine plays a role in TTH chronification. Anxiety and depression were assessed through self-administered inventories, not a formal psychiatric evaluation. Also, we did not evaluate smoking status of the participants. The obtained samples were not fasting; however, we minimized the influence of circadian rhythm by collecting all samples at the same time of the day.
In conclusion, the present study showed a mild increase of IL-8 serum levels in TTH and an increase of MCP-1 associated with TTH headache pain, suggesting that inflammation has a role in TTH pathophysiology. Future and larger studies are still needed to assess the role of inflammation in TTH chronification.
Clinical implications
IL-8 levels were increased in tension-type headache. MCP-1 levels were higher in patients with headache at the time of assessment. There were no differences in chemokine levels between episodic and chronic tension type headache. Pro-inflammatory mechanisms may participate in tension-type headache pathophysiology.
Footnotes
Funding
This work was funded by CNPq and Fapemig, Brazil. Dr Domingues is the recipient of a CAPES post-doctoral scholarship.
Conflict of interest
None declared.
Acknowledgements
We gratefully acknowledge the contribution of Cassio Lacerda and Tarnara Campostrini in data collection.