
Abstract
The clinical characteristics of chronic daily headache were studied in 40 children and adolescents, as well as the associated factors responsible for maintenance of the continuous headache pattern. The study of the clinical headache characteristics, showed a female preponderance (75%), mean age of 11 years old at the first consultation, and onset of headache symptomatology at a mean age of 8.5 years old. The average time interval for the evolution of sporadic headache into chronic daily headache was 1.4 years, and psychosocial stressors were present, acutely or chronically, during the period of headache-frequency increase in 47% of the children. Headaches were classified as transformed migraine (65%), mixed pattern (17.5%) and chronic tension-type headache (17.5%). Sixty per cent of patients had mothers with migraine. Data regarding common analgesic use showed an average intake of 11.2 days/month.
Introduction
Chronic daily headache (CDH) specifically for adults was first described by Mathew et al. (1). It is characterized by headache that has transformed into episodes of daily pain from either episodic tension-type headache or migraine, or less often by headaches that already start with a continuous pattern. Often it is associated with overuse of analgesic medication.
CDH is a term used to define a group of headaches that are not included in the IHS classification (2). Silberstein et al. (3) proposed a new classification for CDH that reflected their clinical observations. Diagnostic criteria for four types of CDH were proposed: transformed migraine, chronic tension-type headache, new daily persistent headache, and hemicrania continua. The criteria for transformed migraine included meeting IHS criteria for migraine in the past, daily headache for more than 1 month, average headache duration of 4 h, and a history of increased headache frequency with decreased migraine symptoms over the last 3 months. Criteria for chronic tension-type headache included headache frequency of more than 15 days per month, with a duration of pain lasting more than 4 h per day for at least 6 months. Also, patients should have pressing, bilateral pain with mild-to-moderate severity that is not aggravated by physical activity. There should be a history of episodic tension-type headache in the past, with an evolution to daily headaches in the past 3 months, and an absence of autonomic symptoms. Criteria for new daily persistent headache included a headache frequency of more than 15 days per month, lasting more than 4 h per day, no history of tension-type or migraine headache in the past, and an acute onset of constant unremitting headache. Criteria for hemicrania continua included duration for at least 1 month, unilateral in location, and relief with indomethacin. Pain must be continuous but fluctuating, of moderate severity, and lack known precipitants.
The diagnostic criteria for CDH are not yet established for children and adolescents.
The prevalence of CDH among adults is 0.5 to 6%(4–7). In the paediatric population the rates are lower at 0.2 to 0.9% (8, 9).
CDH evolves from migraine in approximately 50% of cases and is frequently associated with analgesic overuse and psychiatric comorbidity (depression and anxiety), compromising the patient's life quality (10). In adults with CDH, 23% reported that an intermittent headache was present before 9 years of age, and 36%, between 10 and 19 years (6). The patients refer to a gradual transition of sporadic headache into a chronic one, after a mean interval of 10 years (6). A meta-analysis study of CDH showed that the average time period between the sporadic headache onset and the chronic form was 20.4 years, analgesic overuse occurred for a mean of 13.3 years and the duration of the daily headache was 5.9 years (11).
There are few studies about CDH in children and adolescents (12–17). They observed a higher rate of psychopathology, quality of life disability, female preponderance, CDH onset around 11–12 years of age, and a low rate of analgesic overuse. Although some studies refer to a high rate of transformed migraine (14, 15), others observed a high frequency of migraine headache symptomatology intermixed with tension-type headache, defined as a co-morbid state (12). More recently, studies suggest that, rather than having two co-existent headache types, children and adolescents with CDH have a single syndrome that will sporadically and paroxysmally worsen and gather migrainous characteristics (16, 17).
The objective of this study was to address the clinical characteristics of CDH in childhood and adolescence, using the adult criteria as a diagnostic tool (3), and to study the psychological stressors and traits that might be associated with the onset of CDH.
Patients and methods
Between January 1999 and April 2000, 51 children and adolescents, aged 7–14 years, with a history of headache frequency ≥ 15 days/month for more than 6 months, were referred to our outpatient clinic as part of a placebo-controlled clinical trial for drug treatment of CDH.
A detailed clinical history, with emphasis on primary headache symptomatology, physical and neurological examination, was taken on the first visit. Children with secondary headaches were excluded and all patients with abnormal neurological examination were also excluded. The patients and their relatives were directed to keep a monthly headache diary in which they recorded the frequency, duration and intensity of the headaches, occurrence of associated phenomena, worsening factors, and analgesic medication usage.
The first follow-up visit was scheduled after a month, when the headache frequency was checked. At the follow-up visit, those with a headache frequency of ≥ 15 days/month filled out questionnaires of self-evaluation for depression [CDI: Child Depression Inventory, Kovacs, 1983 (18)], anxiety [STAI: State-Trait Anxiety Inventory, Spielberger et al. 1973 (19)] and life quality [AUQEI: Autoquestionnaire du qualité de vie enfant imagé, Manificat and Dazord, 1997 (20)], adapted to the Brazilian population. The results of the questionnaires were used to classify the patients as having or not having traits that suggested a probable depressive tendency (CDI), an anxiety susceptibility (STAIT), and impairment of the quality of life (AUQEI).
The patients had monthly follow-up visits as part of a drug-treatment protocol that used placebo in a double-blind crossover way. They were followed for a mean period of 12.4 months. The study was approved by the ethical committee of our hospital and informed consent was obtained from the parents, according to the Helsinki declaration.
The primary headache that developed into the chronic form was classified according to the criteria of the IHS. Data obtained from the headache diary was used to classify CDH according to the criteria proposed by Silberstein et al. (3), as shown in Table 1, and Gladstein et al. (21) that defined the mixed pattern (co-morbid state), a co-existence of sporadic migraine and tension-type headache in the same patient.
Proposed criteria for daily or near daily headaches [Silberstein et al. (3)]

Data concerning the headache diary, as well as the primary headache symptomatology that developed into CDH was stored in the databank software Epi Info, version 6.03 (Dean et al. Center for Disease Control and Prevention, Atlanta, Georgia, USA, 1994).
We compared the following variables according to sex: age at the first visit, mean time of headache history, pain duration and headache frequency, days/month of analgesic intake, and questionnaire ranking.
Statistical analysis was performed using the Mann–Whitney test for independent samples with continuous variables, Kruskal–Wallis test for variance analysis between independent samples, and χ2, or exact of Fisher, for categorical variables or classificatory proportions, with a level of significance of 0.05.
Results
Of the 51 initially admitted, 40 constituted the study group. They had a headache frequency ≥ 15 days/month based on the headache episodes recorded in the diary. Eleven patients had a headache diary frequency < 15 days/month, and were excluded.
There were 30 (75%) female and 10 (25%) male patients, with a mean age of 11 years old (variance = 4.25 years).
Headaches clinical characteristics are shown in Table 2. Pain was localized mainly in the frontal and temporal regions (77.5%), being bilateral, in 75% of the patients, with a pulsatile quality in 60%, and duration > 2 h in 85%.
Clinical characteristics of headaches in the study group

NC, non classified.
One patient had migraine with aura and had variable pain intensity.
The primary headache classification of the study group based on the IHS diagnostic criteria is shown in Table 3. Migraine was the most common diagnosis, being present in 80% of the patients. Based on the data recorded in the headache diary, 26 (65%) patients were classified as having transformed migraine, seven (17.5%), the mixed pattern, and seven (17.5%), chronic tension-type headache (Table 4).
Primary headache classification of the study group, according to IHS diagnostic criteria (classification of the primary headaches that developed into CDH)

MDNF, migrainous disorder nor fulfilling the IHS criteria; CTTH, chronic tension-type headache.

Thirty-seven patients filled in the CDI questionnaire, 36 completed the STAI, and 35 the AUQEI. Younger children were not able to complete the questionnaires on their own, nor could fully understand the meaning of some questions. The results showed that 10/37 (27%) patients had scores that suggested a depressive trait, 7/36 (19.5%), scores that revealed a high anxiety status, and 11/35 (31.5%), low scores in the quality-of-life questionnaire. Of the 36 that were able to complete both questionnaires, four patients (11%) had both anxiety and depressive traits.
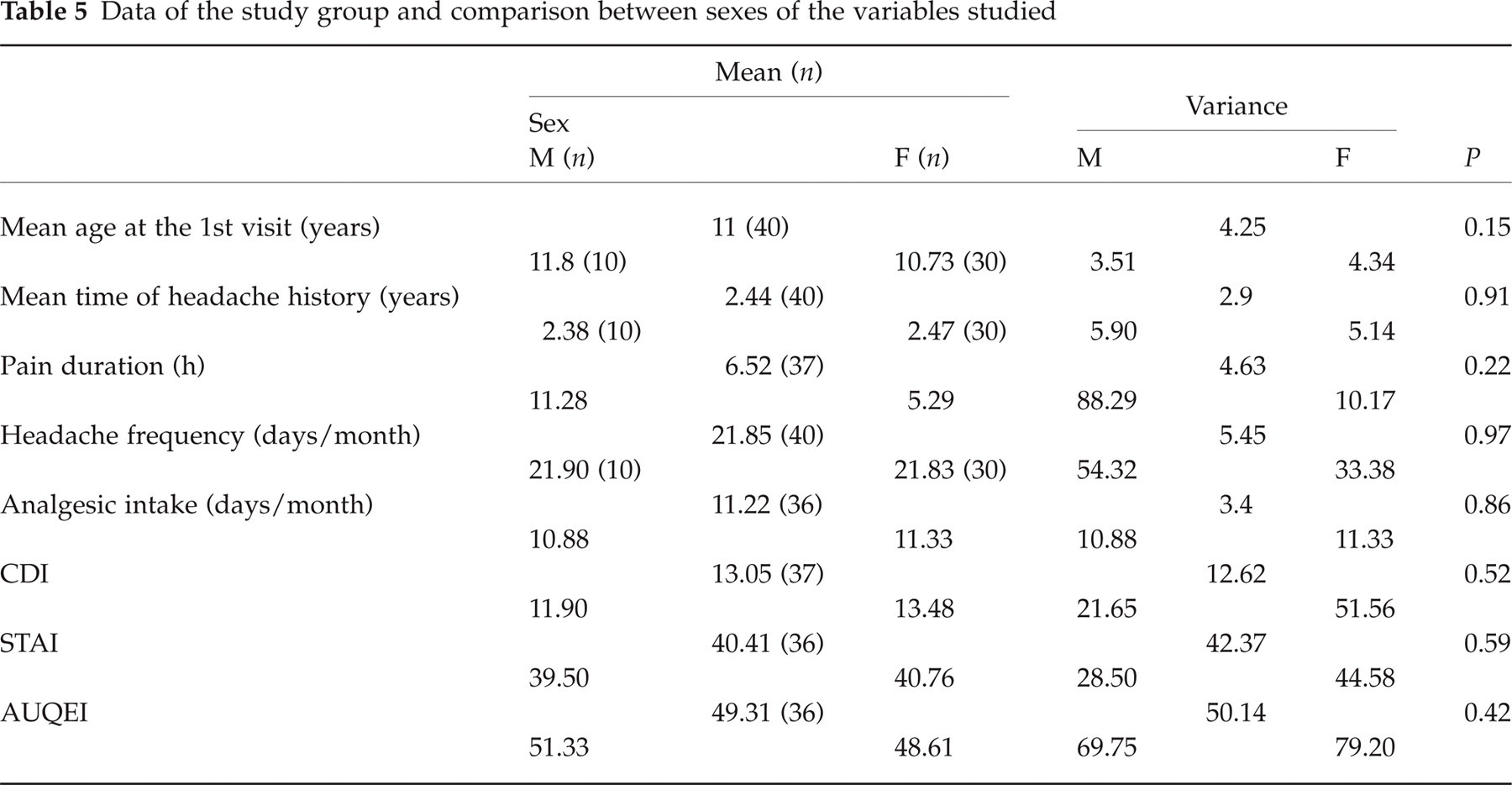
Table 5 shows data of the study group concerning mean age at the first visit, mean time of headache history, headache duration, headache frequency, monthly analgesic intake and questionnaire ranks, comparing male and female patients. There were no significant differences (Mann–Whitney test) concerning the variables above between female and male patients.
Data of the study group and comparison between sexes of the variables studied
The mean time interval for the transition of sporadic headaches into CDH was 1.4 years (1 month to 6 years).
Psychosocial stressors, in low-to-moderate levels, occurred in an acute or chronic form during the increase of headache frequency in 19 (47.5%) patients. The most common were school (failure, change), detected in six patients, and domestic problems (parent's fighting frequently, parental illness), in five.
Twenty-four (60%) patients had mothers with migraine.
Common analgesic drugs (nonergotamine) were used by 33 patients (82.5%), with an average intake of 11.2 days/month (Fig. 1). We were not able to precisely define the dosage intake for most of the patients. The drugs most commonly used were paracetamol and dipirone.

Frequency of analgesic intake (days/month).
There was no significant difference between transformed migraine, mixed pattern and CTTH regarding age at first consultation, age at onset, time interval for the transition of sporadic headaches into CDH, headache frequency, pain duration, analgesic intake, and questionnaires of self-evaluation for depression, anxiety and life quality (Kruskal–Wallis test).
Discussion
Our study showed that the headache diary is important for the diagnosis of CDH. This allowed us to exclude 11/51 (21.5%) patients initially referred to our headache clinic complaining of frequent primary headaches that would otherwise be incorrectly classified as CDH. This finding stresses the importance of a diary in headache management.
We observed a predominance of the female sex, a fact also noticed by others that studied CDH in this age group (12–14).
We found a striking predominance of migraine as the primary headache that developed into CDH in our study group. As a tertiary centre for the treatment of headaches, this finding is in agreement with other studies that were performed in specialized clinics (13, 14). The clinical symptomatology of the primary headaches in our study group are in accordance with those symptoms commonly observed when the study has a high rate of migrainous patients (14).
Transformed migraine was the major CDH type observed our study, being present in two-thirds of our patients, followed by the mixed pattern (17.5%), and chronic tension-type headache (17.5%). No patient in our study group had hemicrania continua or new daily persistent headache.
These findings are in disagreement with those of Gladstein et al. (12) that classified only 15% of their patients as transformed migraine, while 40% had a mixed (‘co-morbid’) pattern and 35% had new daily persistent headache.
We believe that the higher rate of transformed migraine observed in our study was due to the higher time elapsed between the episodic migrainous crises and transformation, which in our cases was always > 6 months.
Hershey et al. (14) studied 200 patients, 3–18 years of age, with headache frequency ≥ 15 days/month. Migraine was diagnosed in 92% of them, although only 60% met the IHS criteria. They observed that children had difficulties describing the transition from migrainous headaches into the transformed pattern. This can be a problem when defining this particular type of CDH in children, as they usually have difficulties in describing symptoms that are mainly subjective in nature.
There are no other published studies that address CDH types in children and adolescents that could be used for comparison. Perhaps the different findings could be due to methodological issues. We had a large proportion of patients who had definite migrainous symptoms in their past history (80%), and who developed a transformed migrainous pattern at the time they were seen in our clinic. Studies with a large number of patients with frequent headaches from the onset, or a history of short headache duration, are prone to find a higher rate of new daily persistent headaches and mixed pattern diagnoses.
The mixed pattern type of CDH was observed in 17.5% of our study group. The headache diary is of the utmost importance in establishing the diagnoses, because, with frequent headache episodes, it is impossible to recall each headache characteristics that allows the physician to classify them accordingly.
The mean time for transformation of migraine into CDH was 1.4 years in our study, lower than that observed in adult studies, which varied between 10 and 20 years (1, 6, 11). Although there is always the possibility of a bias in recall, perhaps the shorter transformation period observed in children allows a more accurate estimate of the time for transformation compared with adults.
We noticed the presence of psychosocial stressors in 47% of the patients associated with the increase and maintenance of headache frequency in our study group. This association was also observed by others (12, 22).
A depressive trait was observed in 27% of our sample. Lanzi et al. (23) used the same evaluation method in 32 children with primary headaches (migraine, and tension-type headaches), and found 31.6% children with a borderline depression. Abu-Arafeh (16), in a study of 150 children with chronic tension-type headache, observed 22.6% with significant chronic neurological or psychological disorders, and 9.6% with serious stressful events related to family illnesses. Wayne-Holden et al. (24) studied the prevalence of psychiatric co-morbity in 70 children with CDH, with a mean age of 12 years old, and suggested that CDH in children may be associated with more significant psychopathology and disability.
Parameters of overuse of medication have not yet been defined for children and adolescents. Although we noticed a high rate of common analgesic intake (85%) during several days/month (mean = 11.2), based on 1 month recording of the headache diary, we were not able to gather data on the amount ingested. There are no figures on this issue reported in the literature concerning this age group.
We conclude that CDH in childhood and adolescence evolves predominantly from migraine, has a shorter transformation period compared with adults and is associated with psychosocial stressors. Medication overuse should be a subject for further study, as well as therapeutic measures that address psychological factors related to the chronic headache transformation.