
Abstract
The role of non-pharmacological therapies in the preventive treatment of tension-type headache (TTH) is still an object of debate. The primary aim of this study was therefore to investigate the therapeutic effect of physiotherapy in properly classified patients with TTH in a controlled trial. Fifty patients with TTH, 26 with episodic, frequent (ETTH) and 24 with chronic TTH (CTTH) fulfilling the International Headache Society classification criteria were included in the study. After a 4-week run-in period, they were randomized to either an 8-week period of standardized physiotherapy (group 1) or to an 8-week observation period followed by an identical course of physiotherapy (group 2); after the physiotherapy all patients were followed for a 12-week follow-up period. We then evaluated the number of days with headache, severity and duration of the headache attacks, and drug consumption for symptomatic treatment before and after the course of physiotherapy. Forty-eight patients completed the study. The average number of days with headache per 4-week period was reduced from 16.3 days at baseline to 12.3 days in the last 4 weeks of treatment [from 14.5 days to 10.5 days (P < 0.001) in group 1 and from 18.1 days to 14.1 days (P < 0.001) in group 2]. Severity and duration of headache as well as drug consumption were unchanged throughout the study. Analysing the response to treatment separately in the various subgroups, we found that the number of responders was significantly higher among patients with CTTH vs. patients with ETTH (P < 0.002) and in females vs. males (P < 0.02). No differences were found between patients with and without disorder of pericranial muscles. We conclude that a standardized physiotherapy programme has a good therapeutic effect, albeit on a restricted group of patients.
Keywords
Introduction
Tension-type headache (TTH) is the most prevalent form of headache. In population-based studies in developed countries, the estimated lifetime prevalence rates range from 35% to 78% of the adult population (1, 2). TTH contributes a large burden of disability, loss of workdays, diminished quality of life and considerable healthcare costs (3,4).
The older terms ‘muscle contraction headache’, ‘psychogenic headache’ or ‘tension headache’ have now been rejected. In 1988, the International Headache Society (IHS) applied the current term ‘tension-type headache’ and defined two subgroups associated and unassociated with disorder of pericranial muscles, respectively (5).
Physiotherapy is widely used in the treatment of TTH, but scientific evidence of any possible beneficial effects is quite limited. Most of the previous studies were conducted in improperly classified headache groups. It is difficult to apply a placebo-controlled design to non-pharmacological treatment studies and most case reports are uncontrolled and unblinded (6) and do not fulfil present-day methodological standards (7).
The primary aim of the present study was therefore to investigate the therapeutic effect of physiotherapy in properly classified patients with TTH in a controlled trial. A secondary aim was to determine whether physiotherapy has a different effect on patients with episodic (ETTH) vs. chronic tension-type headache (CTTH), in males vs. females, and in patients with TTH associated with (MUS) vs. not associated with disorders of pericranial muscles (non-MUS) according to the two- and three-digit diagnostic levels of the IHS classification (5). In particular, we aimed to characterize those patients who benefited from physiotherapy by evaluating any possible factors that might predict a good therapeutic response. Furthermore, we aimed to evaluate the long-term effect of physiotherapy during a 12-week follow-up period.
Materials and methods
Patients
Fifty patients with frequent ETTH (arbitrarily defined as ≥ 8 and < 15 days with TTH per month) or CTTH fulfilling the IHS criteria (5) were included in the study. The patients were recruited from the out-patient Headache Clinic at the Gentofte University Hospital in consecutive order and were given a complete physical and neurological examination. Inclusion criteria were: duration of TTH for at least 1 year, age between 18 and 70 years, and no use of any preventive headache therapy. Exclusion criteria were: migraine attacks more than once a month, other forms of primary headache or neuralgia, other neurological, systemic or psychiatric disorders, and analgesic medication abuse (more than 100 tablets per month) or frequent use of ergotamine or triptans (more than two doses per month). Prior experience with physiotherapy was not an exclusion criterion. Informed consent was obtained from the patients and the study was approved by the local Ethics Committee. This study is part of a multifaceted study of TTH, other parts of which have been published previously (8, 9).
Study design
All patients had to keep a diagnostic headache diary (10) during the 4-week run-in period to ensure that they fulfilled the inclusion criteria. They were subsequently randomized to either an 8-week period of standardized physiotherapy (group 1) or to an observation period of similar length with clinic visits to the neurologist (R.J.) at week 4 and week 8 (group 2, see Fig. 1). Thereafter, group 2 received the same course of physiotherapy as group 1. At the end of the physiotherapy course, all patients were evaluated in a 12-week follow-up period (see Fig. 1). Patients were instructed to fill in the diary (10) at the end of each day with headache and to record the mean severity of pain on a 0–3 scale, where 0 was no pain and 3 was severe, debilitating pain that required bed rest. A standard dose of analgesics was defined as a dose equivalent to 1000 mg of acetylsalicylic acid (ASA).

Study design.
Methods
Pericranial tenderness was evaluated prior to the treatment or observation period by palpation of nine pairs of pericranial muscles and of tendon insertions in group 1 and in group 2, respectively (11). The manoeuvre was carried out by the same person – a trained technician – throughout the study, following a standardized procedure. The trained technician was kept uninformed about the subjects’ headache history. Tenderness was scored in each location according to an ordinal scale from 0 to 3, and scores from all sites were summated. This Total Tenderness Score (TTS) system has proved to be reliable (12). We had previously demonstrated that the ideal cut-off value for separating TTH subjects from non-headache subjects with respect to muscle tenderness was the 75% quartile of TTS obtained from a general population (13). In the following studies, TTS was used as the only criterion for further subdividing patients according to the IHS criteria at the three-digit level. Those with TTS > 9 (equal to the 75% quartile of TTS from healthy controls) were classified as having an association with muscular disorders (MUS), whereas those with a TTS value of ≤ 9 were classified as unassociated with such disorders (non-MUS) (13).
Physiotherapy
The course of physiotherapy was designed to give patients individual treatment twice a week for 4 weeks and then physical exercise for another 4 weeks in small groups together with four to six other patients. The patients followed both a fixed standardized programme consisting of initial massage, basic relaxation techniques (autogenic training and cognitive-behavioural therapy) and smooth stretching, and a daily programme to be done at home acting on shoulder, neck and pericranial muscles. Self-responsibility and activity were emphasized and any form of passive treatment, such as cryotherapy, ultrasound and transcutaneous electrical nerve stimulation (TENS) were to be avoided. The physiotherapist tried to instruct the patients on how to identify and avoid any possible muscular stress factors in their daily life. One of the purposes of this treatment was to teach patients to be active and learn how to handle, control and hopefully avoid their pain. The procedures were performed by an expert physiotherapist who was blinded to the subjects’ headache history and the presence of muscular disorders.
Statistical analysis
Results are presented as mean values and standard deviations. For data analysis, the clinical parameters were evaluated in the run-in period, in the last 4 weeks of physiotherapy and in the last 4 weeks of follow-up in both groups, and in the last 4 weeks of the observation period for group 2. The primary efficacy parameter was the number of days with headache out of 28 days. We have calculated the difference in the number of days with headache between the last 4 weeks of physiotherapy and the baseline in group 1, between the last 4 weeks of physiotherapy, the last 4 weeks of the observation period and the baseline in group 2. We have verified, in group 2, the modification in the same parameter between the baseline and the last 4 weeks on the observation period. Responders were defined as those patients with> 50% reduction in headache days in the last 4 weeks of treatment compared with the run-in (baseline) period as indicated in the IHS guidelines for clinical trials in TTH (7). Secondary outcome parameters were the average duration and severity of attacks and drug consumption for symptomatic treatment. The analysis was first carried out in the whole sample and then repeated in ETTH vs. CTTH patients, in males vs. females and in MUS vs. non-MUS patients, respectively.
The Wilcoxon signed rank sum test and the Mann–Whitney test were used to compare paired and unpaired data between subjects, respectively. The Fisher's exact test (two-sided) was used to compare the percentages of responders in ETTH vs. CTTH patients, in males vs. females and in MUS vs. non-MUS patients. All data were analysed with SPSS software, version 10.0 (SPSS Inc., Chicago, IL, USA). A 5% level of significance was used.
Results
Forty-eight patients completed the treatment period and their demographic and clinical characteristics are shown in Table 1.
Clinical characteristics of the 48 patients studied
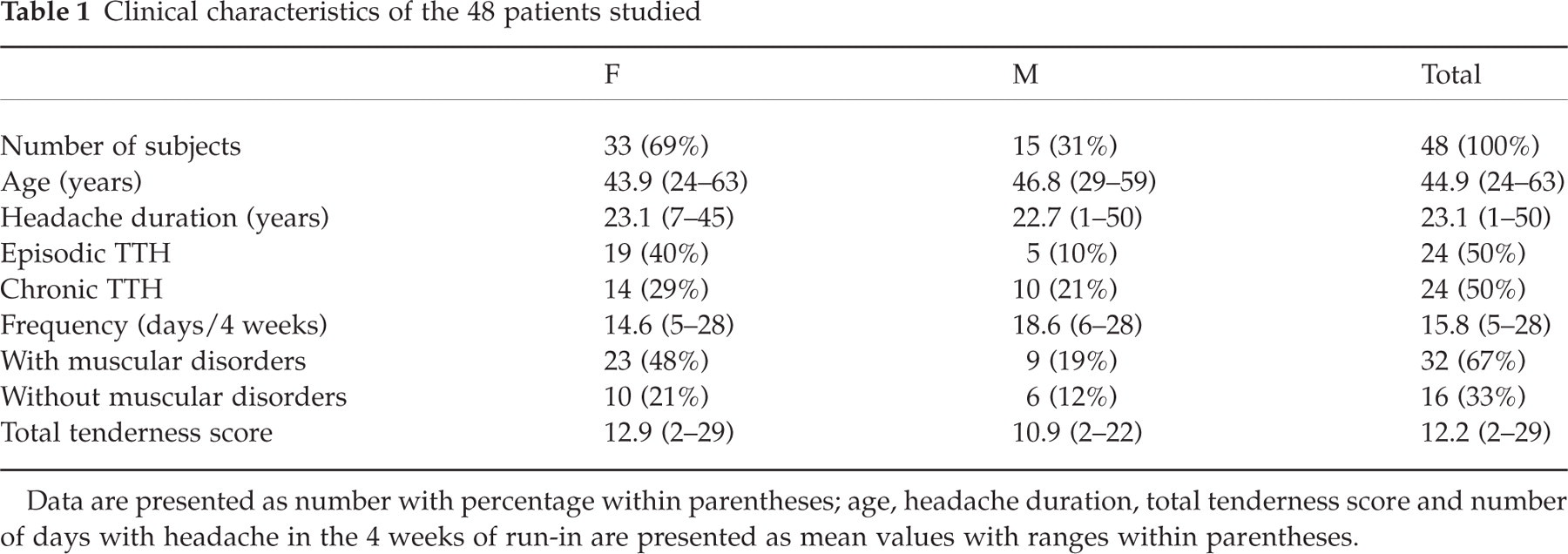
Data are presented as number with percentage within parentheses; age, headache duration, total tenderness score and number of days with headache in the 4 weeks of run-in are presented as mean values with ranges within parentheses.
Participant flow through the trial is displayed in Fig. 2. At baseline, group 1 and group 2 did not differ significantly with respect to number of days with headache, severity and duration of headache, and analgesic medication used (see Table 2). At the 8-week evaluation, the number of drop-outs did not differ between the two groups – one female patient did not complete the treatment period because of a poor response to treatment after 4 weeks (group 1), while the other patient dropped out for personal reasons unrelated to the study (group 2).

Participant flow in the study.
Clinical characteristics in Groups 1 and 2

Data are presented as number with percentage within parentheses; number of days with headache, headache severity and duration, drug consumption are presented as mean values with ranges within parentheses.
Days, number of days with headache/28 days; severity, 0–3 scale; duration, hours of headache/24 h; drugs, number of tablets per 28 days expressed in equivalent dose of 1000 mg of acetylsalicylic acid.
Furthermore, in the follow-up period, 11 patients (five males and six females) dropped out because they failed to show up regularly for the planned follow-up visits. The clinical characteristics at baseline of the 11 drop-out patients did not differ significantly.
Clinical effects of physiotherapy
The number of days with headache was significantly decreased after physiotherapy. The average number of days with headache per 4-week period was reduced from 16.3 days at baseline to 12.3 days in the last 4 weeks of treatment [from 14.5 days to 10.5 days (P < 0.001) in group 1 and from 18.1 days to 14.1 days (P < 0.001) in group 2]. There was no difference between the run-in period (18.1 days) and the observation period (17.8 days), while the significant reduction in the average number of days with headache per 4-week period was confirmed between the observation period (17.8 days) and after the treatment (14.2 days) in group 2 (P < 0.001). The effect was maintained throughout the 12-week follow-up period, with an average headache frequency of 8.6 and 14.2 days in group 1 and in group 2, respectively (see Fig. 3).
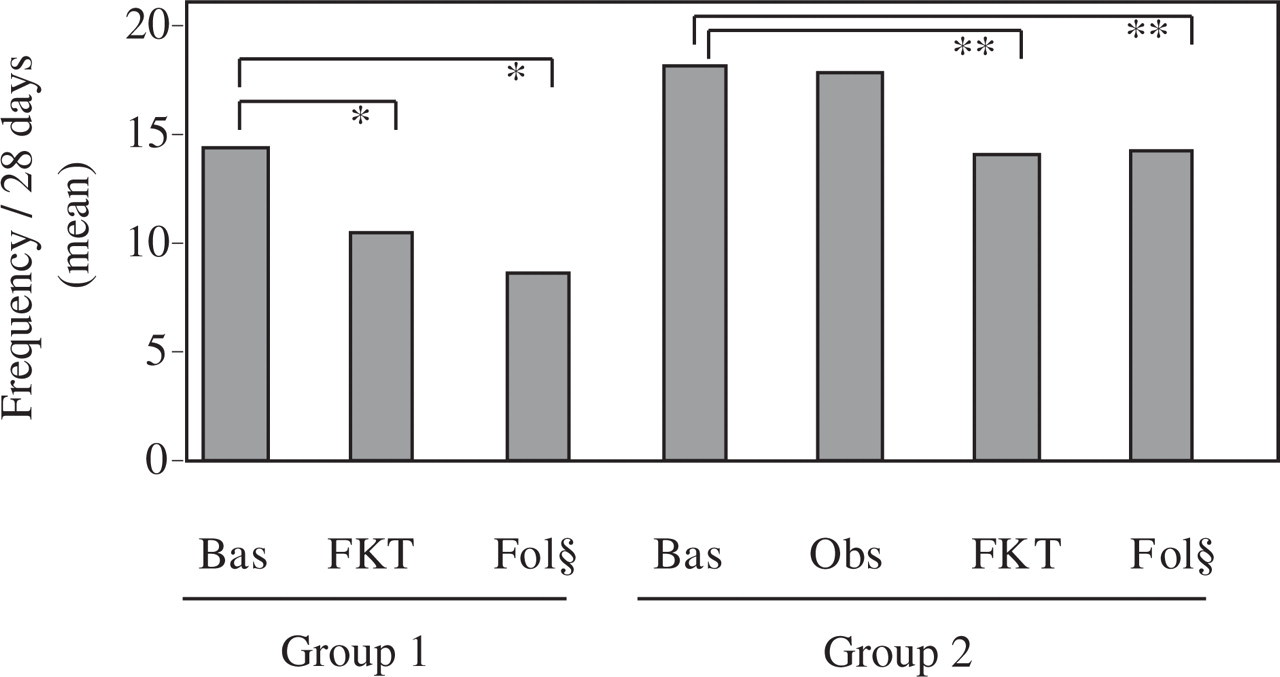
Effect of physiotherapy on headache frequency. ∗P < 0.001; ∗∗P < 0.001.
The severity and duration of headache were unchanged throughout the study periods in both groups. The severity was 1.6 at baseline and after physiotherapy and 1.8 in the follow-up period in group 1; it was 1.7 at baseline and in the observation period, 1.6 in the last 4 weeks of treatment and 1.7 during the follow-up period in group 2. The duration of headache varied from an average of 9.8 h at baseline and 9.4 h in the follow-up in group 1 and from 12 h to 11.4 h in group 2.
Drug consumption, at doses equivalent to a 1000-mg dose of ASA, was significantly reduced only in the follow-up period vs. baseline for both groups (P < 0.001): the average analgesic use was 19.7 tablets per 28 days expressed in equivalent dose for group 1 and 23.6 for group 2 at baseline, and 14.8 for group 1 and 12.9 for group 2 during follow-up, respectively. No significant differences were found in medication use in both groups between baseline and the treatment period, the mean dose taken during physiotherapy being 18.5 for group 1 and 22.3 for group 2.
ETTH vs. CTTH patients
The number of days with headache was reduced in the last 4 weeks of physiotherapy in both groups, but significantly so only in CTTH patients (P < 0.001). Among ETTH patients, the number of days with headache was reduced from 9.5 in the run-in period to 8.1 in the treatment period and to 7.5 in the follow-up period in group 1, but the reduction was not significant (P = 0.57); group 2 exhibited the same pattern as group 1. Among CTTH patients, the effect was maintained throughout the 12-week follow-up period, whereas the number of days with headache was largely unchanged in ETTH patients (P = 0.36, see Fig. 4). The other clinical parameters considered in the study, i.e. headache severity and duration and drug consumption, did not show any significant variations within ETTH and CTTH patients.
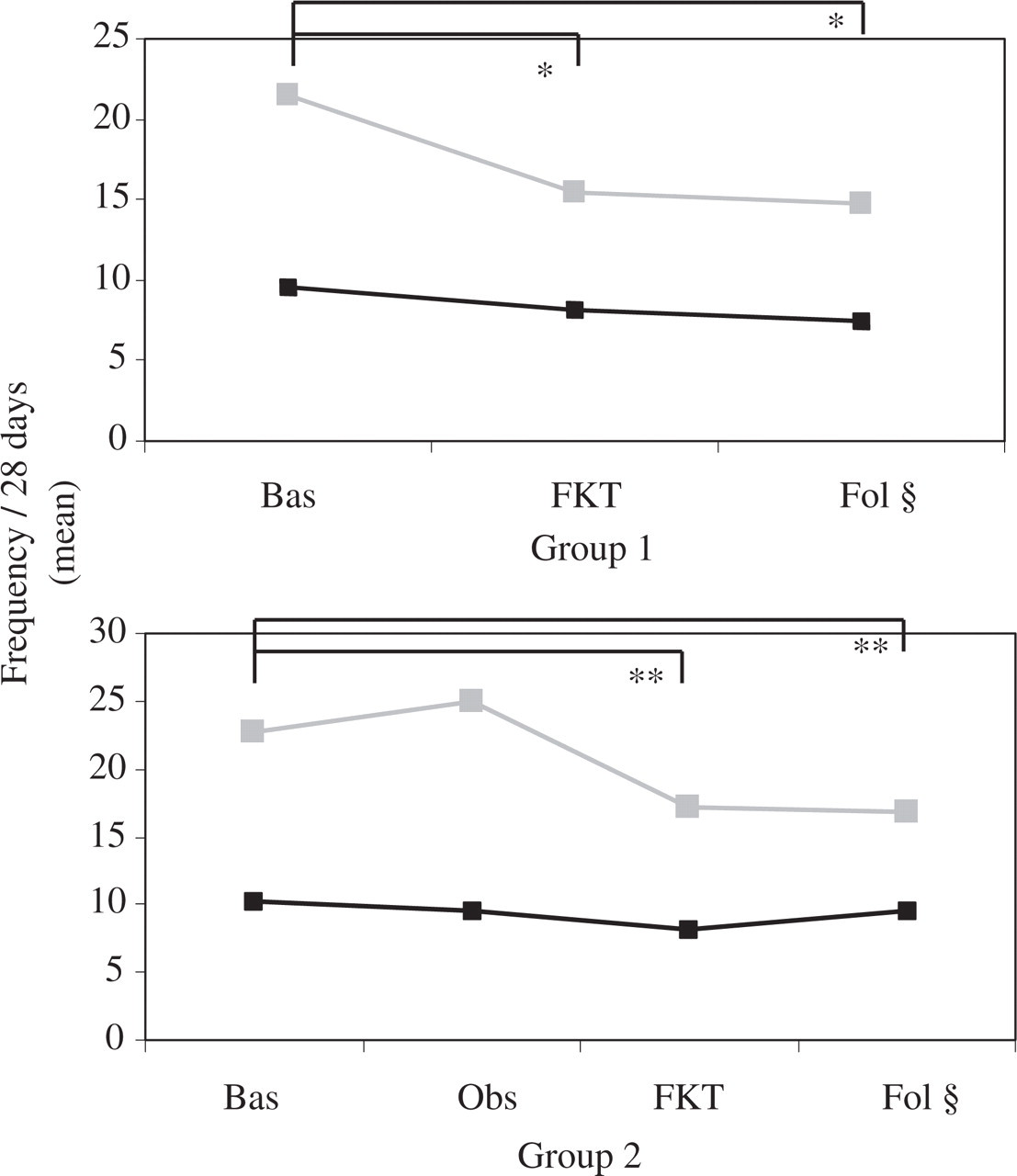
Effect of physiotherapy on headache frequency in episodic and chronic tension-type headache patients. ░, Chronic TTH; ▪, episodic TTH. ∗P < 0.001; ∗∗P < 0.001.
MUS vs. non-MUS patients
The number of days with headache was significantly reduced after physiotherapy in both groups to the same extent (MUS, P < 0.002; non-MUS, P < 0.002) and the effect was maintained throughout the 12-week follow-up period (see Fig. 5). The analysis of the other clinical parameters did not show any differences between the periods considered within these two groups.

Effect of physiotherapy on headache frequency in tension-type headache with (MUS) and without (non-MUS) muscular disorder. ░, MUS+▪, non-MUS. ∗P < 0.002; ∗∗P < 0.002.
Responders
In 29% of the sample (14 patients out of 48), the number of attacks was reduced by> 50% (7). The number of responders did not vary significantly between group 1 and group 2 (9/24 and 5/24, respectively). Analysing the response to treatment separately in the various subgroups, we found that the number of responders was significantly higher among patients with CTTH (13/24) vs. patients with ETTH (1/24) (P < 0.002) and in females (12/33) vs. males (2/15) (P < 0.02). In the female population, the proportion of CTTH responders (11/14) was significantly higher than that of ETTH responders (1/19) (P < 0.002), while in the male population the proportion of responders did not differ significantly between CTTH (2/10) and ETTH (0/5) (see Table 3). Of the 11 female responders with CTTH, nine (82%) had TTH MUS and the remaining two had TTH non-MUS. Of the two male responders with CTTH, only one (50%) had TTH MUS (P < 0.06). In the CTTH non-responder group, six of the eight men (75%) had TTH MUS, compared with one of the three women (33%). In the ETTH non-responder group, 13 of the 18 women (72%) had TTH MUS, compared with two of the five men (40%). The only responder among ETTH patients was a woman who had TTH non-MUS. No significant difference was found between MUS patients (10/32), all of them with CTTH (nine female and one male), and non-MUS (4/16) patients (P = 0.69), three with CTTH (two female and one male) and one woman with ETTH. The duration of attacks (10.4 vs. 14.4 h, P < 0.01) and drug consumption (10.7 vs. 25.4 standard doses, P < 0.01) at baseline was significantly lower in responders vs. non-responders (Table 4).
Distribution of responders (defined as patients with> 50% reduction in headache days) and non-responders
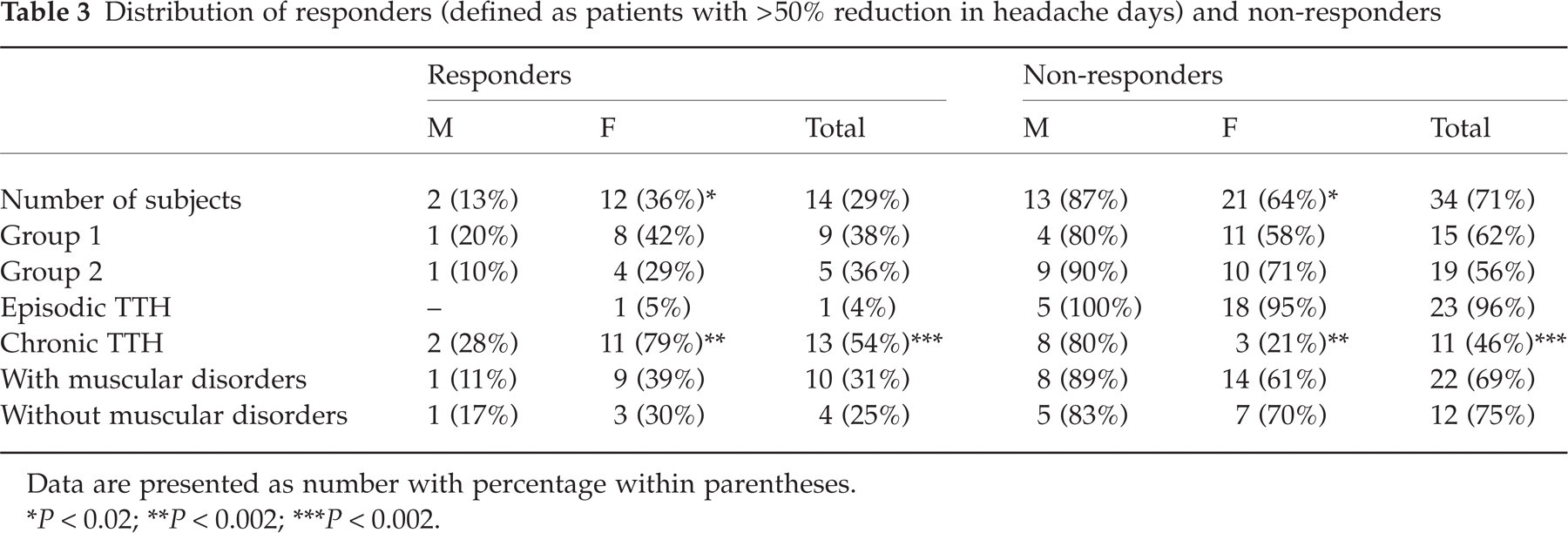
Data are presented as number with percentage within parentheses.
∗P < 0.02
∗∗P < 0.002
∗∗∗P < 0.002.
Clinical features of responders (defined as patients with> 50% reduction in headache days) and non-responders

Data are presented as mean values with ranges within parentheses.
Data are presented as mean values at baseline.
∗P < 0.01
∗∗P < 0.01.
Among non-responders, 21% (10/48) showed a percentage reduction of attacks between 25% and 50%, 25% (12/48) presented with an unchanged clinical course, and the remaining 25% (12/48) exhibited a worsening of symptoms (Fig. 6).

Percentage distribution of effect.
Discussion
Use of complementary non-pharmacological therapies in headache has increased considerably over the last few years. A national population-based survey conducted in the USA to determine the prevalence, costs and pattern of use of unconventional therapies has shown that about one-third of the subjects investigated had followed some form of non-pharmacological treatment in the year prior to the survey and that the cost of such treatments was the same as the annual cost of all hospitalizations in the USA (14). In the field of preventive treatments for headache, systematic reviews and meta-analyses have been reported, but the interventions studied were confined to pharmacological and cognitive/behavioural therapies and mostly to the study of migraine (15). Despite the high prevalence of TTH in the general population, the utilization rates of non-pharmacological therapies in TTH sufferers remain poorly studied. Only a few studies have assessed the effectiveness of traditional physiotherapy techniques of heat, massage, traction, specific exercise or postural education on TTH (6). Using a controlled, randomized design, our study was able to demonstrate a significant reduction in the number of days with headache following physiotherapy, albeit in a small sample of patients. Our findings are in agreement with those of Carlsson et al. (16), who compared physiotherapy treatment with acupuncture in 60 female CTTH patients defined according to the criteria set by the Ad Hoc Committee on Classification of Headache (17). In that trial, ‘physiotherapy’ consisted of a variety of individualized patient-initiated modalities, including relaxation techniques, stretching, TENS and ice therapy, as well as education regarding muscle tension and how to control it ‘autogenically’. Both treatments resulted in benefits for the patients’ mood state and overall health function, as well as for the number of days with headache, even though no exact figures were provided for the latter. The decreased severity of headache assessed on the Visual Analogue Scale in those patients who had been treated with physiotherapy is different from our study results, which demonstrate rather stable severity and duration of attacks despite their reduced frequency.
By contrast, our observations confirm those reported by Hammill et al. (18), who assessed the effectiveness of a treatment programme encompassing ergonomic and postural education in an open uncontrolled study of 20 patients. A significant and long-lasting decrease in headache frequency and drug consumption was noted, although there was no effect on headache severity and headache duration.
Given the poor efficacy and the numerable side-effects of preventive pharmacological TTH treatment, the clinical characterization of headache is certainly of great interest in those patients, predominantly women, who reported> 50% decrease in the frequency of attacks following physiotherapy. Most of these responders were CTTH sufferers, and the average duration of attacks and analgesic use, both assessed at baseline, were significantly lower in responders vs. non-responders. In spite of the fact that pericranial muscular disorders were slightly more frequent in responders, there was also some response to treatment in patients without significant tenderness in the pericranial muscles. Separate data analysis for males and females shows that CTTH women with muscular disorders were those responding better to treatment. CTTH males with muscular disorders and ETTH patients, whether male or female, with or without muscular disorders, responded poorly to physiotherapy. These data need to be confirmed by studies on larger samples that should consider the different parameters identified.
Although current knowledge of the mechanisms of action of physiotherapy and the pathophysiological processes underlying TTH are still unclear, we cannot rule out a priori the existence of a relation between the beneficial effect of physiotherapy and the pathophysiology of TTH. The most prominent abnormal finding in TTH is a considerable increase in tenderness of the pericranial myofascial tissues (11, 19, 20). ETTH and CTTH may or may not share pathogenic mechanisms and it has been suggested that CNS sensitization may contribute significantly to increased tenderness and to chronification of TTH (19). Furthermore, a generalized hypersensitivity to pain probably also contributes to chronic pain in these patients (21). The therapeutic efforts in physiotherapy are primarily designed to produce muscle relaxation, but it may also activate central anti-nociceptive processes. It seems therefore reasonable to assume that, at least in CTTH, there is some convergence between the mechanisms activated by physiotherapy and the systems underlying TTH. In CTTH central sensitization has been shown to play a significant role. It is tempting to speculate that the greater effect in CTTH than in ETTH could be due to reduced central sensitization and/or increased anti-nociceptive action. On the other hand, it is not possible to rule out that the effect of physiotherapy is also mediated by a peripheral mechanism that acts by relaxing the muscles and also increasing local blood flow to the affected area that could reduce the local concentration of pain mediators (22). Muscle stretching is also reported to reduce the excitability of the motorneurone pool which may lead to decreased muscle tone and pain (23).
Our study results are not totally unbiased, as: (i) it is apparent that it is difficult to apply a placebo-controlled, double-blind design methodology in non-pharmacological treatments such as physiotherapy, and our study is controlled but not blinded; (ii) in TTH it is extremely important to consider the placebo effect, even though the lack of response in ETTH and the absolute lack of significant variations in the clinical course during the observation period compared with the run-in period seem to rule out any relevant placebo effect in therapeutic response; and (iii) physiotherapy is mainly based on tradition and experience and the applied treatment strategies are certainly not evidence based. In our study, a standardized therapeutic approach in a controlled design was applied for the first time, but an absolute blinded, controlled study design evaluating the individual treatment modalities in physiotherapy is still lacking in this area.