
Abstract
Background
Although medication-overuse headache (MOH) is common in China, its clinical profile is not yet fully established. Meanwhile, ICHD-3 beta has been published, but its diagnostic criteria require further validation.
Methods
We retrospectively classified the clinical features of 240 consecutive patients with MOH (55 males, 185 females), whose demographic data, headache features, overused medications (type, quantity, frequency and duration of use), headache-attributed burden, and outcomes were reviewed. We then applied the criteria of the several versions of ICHD (II, IIR and 3-beta) to these patients.
Results
Compared with those with other headaches, patients with MOH were more likely to be less well educated (64.6% vs 42.0% for secondary school or lower, p < 0.0001), and on lower annual incomes (72.3% vs 56.0% for an income of Chinese yuan (CNY) 30,000 or less, p < 0.0001). Combination analgesics were the most commonly overused medications, and, caffeine (89.9%), aminopyrine (70.0%), phenacetin (53.9%) and phenobarbital (48.8%) were the most commonly used specific components of these. Only two patients (0.8%) had previously been given the diagnosis of MOH; accordingly, the median time to diagnosis after the estimated onset of the disorder was 4.0 years. The majority of patients (83.7%) improved with treatment. All 240 patients fulfilled the diagnostic criteria for MOH according to ICHD-3 beta; only 134 (55.8%) satisfied the diagnostic criteria for definite MOH according to ICHD-II, while 195 (81.2%) met those of ICHD-IIR.
Conclusions
MOH in China is associated with lower educational level and annual income. MOH has rarely been diagnosed and correctly treated in China. ICHD-3 beta appears to be more appropriate for the diagnosis of MOH than previous versions.
Introduction
Medication-overuse headache (MOH) is one of several headache disorders characterized by headache occurring on ≥ 15 days/month (also known as “chronic daily headache” (CDH)). The cause of MOH is high frequency of use, regularly over a period of time, of medications for the symptomatic treatment of (usually) primary headaches (1,2). Medications linked to MOH include simple analgesics (acetaminophen, aspirin and other nonsteroidal anti-inflammatory drugs (NSAIDs)), but the risk appears higher (appearing earlier or at lower frequency of usage) with opioids, triptans, barbiturates and combination analgesic medications. The relatively few population-based studies suggest MOH has a highly variable prevalence worldwide, in the range 0.6% to 7.2% among adults (3–9), but most findings have nonetheless clustered in the much more limited range 1%–1.5% (10). Even at this level, given that headache occurs on more days than not, and in many cases every day, MOH represents a major cause of public ill health and disability, and imposes a substantial economic burden (11). At an individual level it is highly debilitating and damaging to quality of life.
Interest in MOH has grown only slowly over the last years, both worldwide (3–7,12) and in Asian regions (13–16), but realization of the magnitude of these burdens is nonetheless changing perceptions of MOH among health priorities. It is likely that future iterations of the Global Burden of Disease Survey (GBD) will include MOH (17). Correct characterization and prevalence estimation of this disorder are especially important in this context. In the Chinese mainland, we found in our nationwide population-based study that the prevalence of all causes of headache on ≥15 days/month was relatively low (1.0%) but that MOH accounted for approximately 60% of these (8). In our clinic-based research study, where of course the mix of headache disorders seen is very different from those in a population sample, MOH patients again accounted for almost half of those with headache on ≥15 days/month (18).
ICHD diagnostic criteria for MOH.

MOH: medication-overuse headache; ICHD: International Classification of Headache Disorders (II: second edition; IIR: second edition revised; 3 beta: third edition beta version).
ICHD-3 beta was published for field testing (19); its diagnostic criteria require validation. Here, we survey MOH patients registered at a headache clinic in Beijing, China, characterize their clinical features, and then apply to them, in turn, the criteria of the several versions of ICHD (II, IIR and 3-beta).
Methods
The study protocol was approved by the ethics committee of the Chinese PLA General Hospital, Beijing. All prospective patients were informed of the nature and purpose of the study, and those enrolled gave their consent prior to their participation.
All patients complaining of headache and seen at the International Headache Center of the Chinese PLA General Hospital in Beijing, China, between November 2011 and March 2013, were potential recruits for this study. During the initial consultation, a detailed questionnaire for headache disorders was completed by a certified neurologist. Magnetic resonance imaging of the head/brain was performed in all cases to rule out symptomatic origin. Final diagnoses were confirmed by at least two headache specialists applying ICHD-3 beta criteria (19). A detailed database for each patient included demographic data, headache features (frequency in days/month and maximum pain intensity on a visual analog scale (VAS)), medication(s) overused (type, quantity, frequency and duration of use) and headache-attributed burden assessed as impact on quality of life using the World Health Organization WHOQoL-8 instrument (20). Inquiries were made into educational level and annual income. For purposes of comparison, these inquiries, and quality of life assessments, were also made of patients with other headache disorders seen in our headache center during the same period.
All enrolled patients with MOH were given basic education in the nature and causation of their headache disorders, advised to use a headache diary and instructed in its use, given guidance on withdrawal (according to whatever was being misused) and, when appropriate, prescribed preventive medications. Patients were followed up two months after their enrollment by telephone. Treatment outcome was defined subjectively as “satisfactory” when a patient felt >50% improved and “poor” when improvement was <50% or the patient was unchanged.
All continuous measurements were reported as means ± SD. Categorical variables were compared using the chi-squared test, and continuous variables using Student’s t-test or one-way analysis of variance (ANOVA). For statistical analyses, we used SPSS for Windows, Version 20.0 (Chicago, IL, USA). Statistical significance was set at p < 0.05.
Results
Demographics and clinical features
A total of 3923 headache patients were seen in the headache center during the study period, of whom 1453 had migraine and 240 fulfilled ICHD-3 beta criteria for MOH (185 female, 55 male; 3.4:1 female:male ratio).
Demographic and clinical features of patients with MOH.

MOH: medication-overuse headache; TTH: tension-type headache; CNY: Chinese yuan; VAS: visual analog scale.
Educational levels and annual income attained by patients with MOH or other headaches.

MOH: medication-overuse headache; CNY: Chinese yuan; Other headaches: 3683 patients not fulfilling MOH criteria who visited the International Headache Center of the Chinese PLA General Hospital during the study period, of whom 3320 patients were willing to supply income information.
Overused medications
Overused medications listed by frequency of reported users.

Specific overused drugs listed by frequency of reported users.
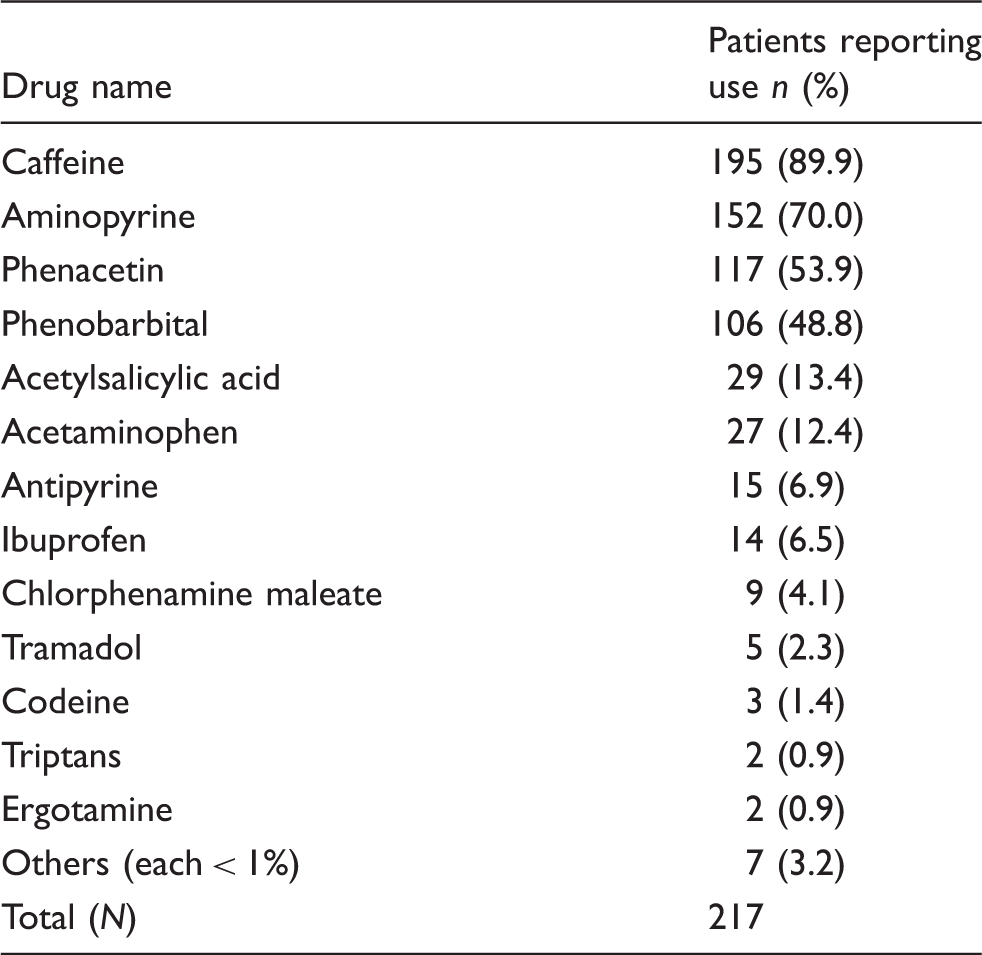
Only 16 patients overused simple analgesics alone (acetaminophen, acetylsalicylic acid or other NSAID). There was no case of ergotamine-overuse or triptan-overuse headache on its own in this study.
Quality of life
Quality of life (WHOQoL-8) in those with MOH or migraine.

MOH: medication-overuse headache; WHOQoL-8: World Health Organization quality of life instrument.
Not all migraine patients answered all questions.
Time delay to correct diagnosis
Only two of the 240 patients (0.8%) had previously been given the diagnosis of MOH for their present disorder. Median time to diagnosis after our estimated onset of the disorder was 4.0 years (quartiles: 1, 9.5; range: 0.25–40). Fewer than 10% (22 patients) were diagnosed in the first year after developing MOH, and for 25% (60 patients), it had taken 10 years or longer.
Treatment and follow-up
Withdrawal of the overused medication(s) was the most common treatment stratagem. Simultaneously, preventive treatments were administered to decrease intensity and frequency of headache during withdrawal in all 240 patients. Of 172 (71.7%) patients completing follow-up two months after the first visit, the majority (144; 83.7%) reported satisfactory improvement; by our criteria, the remainder (28; 16.3%) were judged to have had a poor treatment response. We could not follow up 68 patients (28.3%), being unable to contact 50 (73.5%) of these, while 18 (26.5%) refused to participate in follow-up.
Application of ICHD criteria for MOH
Relative performance of ICHD diagnostic criteria for MOH.

ICHD: International Classification of Headache Disorders (II: second edition; IIR: second edition revised; 3 beta: third edition beta version); MOH: medication-overuse headache.
Agreement between ICHD-IIR and ICHD-3 beta diagnostic criteria for MOH.

ICHD: International Classification of Headache Disorders (IIR: second edition revised; 3 beta: third edition beta version); MOH: medication-overuse headache.
Discussion
This is the largest clinic-based study describing the clinical profile of MOH in mainland China. We found that patients came from throughout China, were predominantly female, were less well educated than patients with other headache disorders and tended to have lower annual incomes. Combination analgesics were more overused than ergotamine, triptans, opioids and simple analgesics. We comment on each of these findings below.
The gender differential (female: male ratio 3.4:1) was both marked and significant, and in the same direction as seen elsewhere in Asia (Taiwan: 1.6:1 (13); Japan: 6.8:1 (14,15); India: 2.4:1 (16)). This was not a population-based study, and health-care-seeking behavior must be taken into account in explaining the magnitude of the difference. Still, the most likely reason is that primary headache disorders in general, and migraine in particular, are more common in women (8), and these are the principal risk factors for MOH since an antecedent headache is a necessary precondition. With regard to gender differences noted in this study, women had significantly lower incomes than men, and lower income has been noted as a risk factor for medication overuse and for headache chronicity (21). While relative poverty of a particular demographic group may affect health across populations, it seems unlikely to do so between genders, at least among those living within families who, presumably, share their income. Overall, our MOH patients were relatively poor: 72.3% estimated their annual income at CNY 30,000 or below, whereas the gross national income (GNI) per capita of China was CNY 35,855 according to the World Bank database in 2012 (22). We showed that MOH patients had significantly lower incomes than patients with other headache disorders. They also attained lower educational levels. These results may support previous suggestions that migraineurs with lower socioeconomic status have higher risk of developing MOH (21), but there is still uncertainty about cause and effect.
Most patients with MOH were overusing combination analgesics; among the most common (51.0% of patients) were aminopyrine, phenacetin, phenobarbital and caffeine in a proprietary formulation (so-called “pain-relief tablet” in China). The popularity of this medication may be explained by its ready availability (over the counter in pharmacies) and relatively low price (average CNY 0.055 per tablet). Although it is known that any use of barbiturates increases the risk of MOH quite substantially (23), this level of overuse of these “pain-relief tablets” is worrying for reasons beyond the causation of MOH: Adverse effects of aminopyrine and phenacetin include nephropathy, agranulocytosis and aplastic anemia, especially in frequent or long-term usage. The prevalence of MOH in China (8) may be at the lower end of the global range (10), but the frequent involvement of these drugs is a particular problem in China. Accordingly, special attention should be paid to those using combination analgesics for the treatment of headache. In contrast, overuse of triptans is very rare in China, as was found earlier in Japan and Taiwan (13–15), partly because of their high price (for instance, rizatriptan costs CNY 28 per tablet) but also because of their unavailability outside hospitals. Similarly, overuse of opioids is uncommon in China, because use of these drugs is severely restricted. We found that overuse of simple analgesics alone is also not very common, particularly compared with habits in western countries (3), presumably because of the cultural preference for alternatives.
Our study revealed that quality of life was significantly lower in patients with MOH than in those with migraine who visited our headache clinic during the same period, this being reflected in six of the eight items of WHOQoL-8. Despite this negative impact of MOH, recognition of this condition by non-headache specialists in China is low: Only 0.8% of patients had previously been given the diagnosis of MOH, although 25% had had the condition for at least 10 years. A revolution in public awareness is needed, as is a dramatic improvement in medical management of headache. MOH should be suspected in anyone with headache on ≥15 days/month; it is the most likely diagnosis by a considerable margin. Prevention of MOH is much preferable to treating an already established condition; inquiry into medication use is part of any headache history, but essential whenever headache recurs frequently.
A key purpose of our study was to compare how the three versions of ICHD performed in diagnosing MOH. We adopted ICHD-3 beta as the standard, applying the criteria from this version as entry criteria to the study; then we applied the stricter criteria of ICHD-II and ICHD-IIR. According to ICHD-II, patients with poor response to treatment, i.e. not reverting to episodic headache after weaning from overused medications (criterion D), could not in our study be diagnosed as definite MOH. This lost 11.7% of patients directly and another 28.3% who did not complete follow-up. This criterion was removed in ICHD-IIR, but still 19.8% of patients failed criterion C (for both ICHD-II and ICHD-IIR). ICHD-3 beta has been published for purposes of field-testing, and will be republished in final form probably in 2016 (19). Clearly it has higher sensitivity than its predecessors. Although MOH patients satisfied with ICHD-3 beta may unavoidably include some patients at the state of medication overuse, we believe this to be more important than specificity. Wherever frequent headache and medication overuse coexist, the latter should be regarded as a high risk factor for the former (6,7) even if it is not already the cause, and should lead to appropriate therapeutic stratagems including withdrawal of the overused drugs as early as possible. The general final criterion for secondary headache disorders in ICHD-3 beta (Not better accounted for by another ICHD-3 diagnosis) puts the onus on the clinician to establish causation by exclusion, which seems a better approach than the prescriptive but sometimes self-defeating method of ICHD-II and ICHD-IIR. It is our opinion that the less restrictive criteria of ICHD-3 beta have obvious advantages for the diagnosis of MOH, and will serve patients better. We also believe they will better serve the purposes of population-based studies intended to inform health policy (17).
Nevertheless, because we studied patients from a hospital outpatient department, the results should only with circumspection be extrapolated to the general population. This is a limitation of this study. Although we recruited from one headache clinic, patients came from all over China, from 25 different regions. A second limitation was that the initial clinical data were collected retrospectively as patient histories, so errors in recall were inevitable. However, the two-month follow-up was completed with prospective data collection, using diaries. A third limitation was that more than a quarter of all patients were lost to follow-up, because of our inability to make contact with them or their unwillingness to return. This of course illustrates one of the difficulties in conducting studies of this sort.
Conclusions
In this clinic series in China, MOH had rarely been diagnosed or treated correctly despite histories going back months to many years. Combination analgesics were far more commonly overused than ergotamine, triptans, opioids or simple analgesics. More attention must be devoted to improving recognition and diagnosis in China. ICHD-3 beta appears more appropriate for the diagnosis of MOH than previous versions of ICHD.
Clinical implications
More attention must be devoted to improving recognition and diagnosis of medication-overuse headache (MOH) because it has rarely been diagnosed or treated correctly despite histories going back months to many years in China. Far more commonly overused combination-analgesics were worrisome for their known toxicity, which should be reduced. The International Classification of Headache Disorders, third edition beta (ICHD-3 beta) appears more appropriate for the diagnosis of MOH than previous versions of ICHD.
Footnotes
Funding
This work was supported by the Clinical and Scientific Supporting Fund of Chinese PLA General Hospital (grant number 2012FC-TSYS-3041); the Capital Development Scientific Research (grant number 2011-5001-04); the National Key Technology R&D Program (grant number 2013BAI04B04); and the National Scientific Research Fund (grant number 2011ZX09307-001-07).
Conflict of interest
None declared.
Acknowledgments
We would like to thank Dr Xuhui Wang, Dr Yujun Zhao, Dr Yingshuo Mi and Dr Yujuan Kong for their efforts regarding patient follow-up.