
Abstract
Background
Headache following stroke has been described in previous studies with an incidence of 23%–54%, but a clear description of headache developing after stroke onset is still lacking. The aim of this study was to determine the incidence and characteristics of persistent novel headache after stroke and to describe the use of medication, including dipyridamole.
Methods
As a follow-up to a prospective study, a standardized questionnaire about characteristics of novel headache and medication use was sent out to surviving patients three years after their stroke.
Results
The questionnaire was sent to 256 patients and returned by 222, of whom 12% (26/222) of patients reported persistent novel headache. Dipyridamole had no significant influence on the incidence. Stroke-attributed headache according to predefined criteria was reported in 7.2% (16/222) of patients, with tension-type-like headache in 50.0%, migraine-like in 31.3% and medication overuse in 6.25% of patients. More than half of patients experienced moderate to severe pain and had a score of 55 or above on the Headache Impact Test-6 scale.
Conclusion
Novel headache after stroke affects one in 10 patients and seems to be unrelated to dipyridamole use. Persistent headache attributed to stroke is similar to tension-type headache for half of patients.
Introduction
Headache is a well-known symptom at stroke onset and has been reported in 9.3%–38% of patients (1–12). Persistent headache following stroke has, however, been described in only a few studies with an incidence of 10.8%–23.3% within two years after stroke (13–16).
A few stroke studies have distinguished between pre-existing and novel headache and between different types of headache, e.g. migraine or tension-type headache (2,16). Because both headache and stroke are prevalent conditions, it is necessary to distinguish between headache that existed before the stroke and persistent post-stroke headache and to know the time interval between the two phenomena if a causal relationship is to be postulated.
Medication-overuse headache may arise when headache patients consume medication in order to achieve relief of headache or other pain (17–19). To our knowledge, the role of headache medication overuse after stroke has not previously been studied. Dipyridamole is a frequently used antiplatelet with the well-known adverse event of headache in 9%–42% of patients (20,21), which is considered to be due to cyclic guanosine monophosphate activation and indirect adenosine-mediated activation of headache pathways, similar to findings in sildenafil and nitroglycerin provocations (22,23).
The aim of this study was to determine the incidence of novel headache following stroke (International Headache Society (IHS) categories 6.1.1. and 6.2.1) and to describe the characteristics of this secondary headache attributed to vascular disorder, including a sub-classification of migraine-like (IHS: 1) or tension-type-like headache (IHS: 2). Finally, we wanted to examine the influence of headache medication overuse and dipyridamole use on the development of headache.
Methods
Patients and initial examination
The study is a three-year follow-up of patients with a stroke diagnosis (ICD-10 codes: I61, I63, I649, I676, I677) from a previously published prospective study on post-stroke pain (4). Patients with a diagnosis of transitory cerebral ischemic attack (G459) or subarachnoid hemorrhage (I609), communication problems (e.g. severe aphasia or dysarthria), dementia, somnolence, lack of consent to participate, or lack of Danish language skills were excluded. Two hundred and seventy-five stroke patients acutely admitted to the Stroke Unit at the Department of Neurology, Aarhus University Hospital, from February 2007 to July 2008, underwent a structured interview on persistent or recurring pain including headache within the three months preceding their stroke and questions on pain experienced in close temporal relation to stroke onset followed by a brief standardized sensory examination conducted by two of the authors (N.S.M and A.P.H) (4).
Stroke etiology was determined in agreement with the Trial of Org 10172 in Acute Stroke Treatment (TOAST) classification by two of the authors (N.S.M and A.P.H) (24,25).
The Scandinavian Stroke Scale (SSS, 0–58) was used for measuring stroke severity, with a score of 45 or below representing a severe stroke (26,27).
Three-year follow-up
A standardized questionnaire designed to classify possible migraine or tension-type headache following stroke was developed based on the principles described by Olesen and Dodick (28) and tested in a post-stroke headache group recruited from another study (29). The final questionnaire was mailed to all surviving patients from the prospective study three years after stroke with an accompanying letter explaining the purpose of the study and requesting that the patient fill in the questionnaire or ask the investigator (A.P.H.) for assistance completing the questionnaire over the phone (4). Patients were asked if they had suffered from headache prior to their stroke and to indicate if the severity of their headache had changed after the stroke (more severe, unchanged, or better). The Headache Impact Test-6 (HIT-6) scale on impact of headache on daily life was applied (30,31).
If patients indicated development of novel headache after the stroke, they were asked: “Have you
A reminder was sent out once, and non-responders were categorized as lost to follow-up.
All drugs dispensed through pharmacies to all citizens in Denmark are registered in the Danish National Prescription Registry. Since headache is a well-known side effect of dipyridamole, a request was sent to the patients together with a written consent to access the database on dipyridamole prescriptions. No reminders were sent to non-responders.
All patients gave written consent at stroke onset, and the study was conducted in accordance with the Declaration of Helsinki and approved by the Danish Data Protection Agency (2006-41-6900). The prospective study was approved by the local ethics committee (20060116).
Data analysis
The patients were divided into two groups based on two criteria. First, their response about headache onset in the prospective study (4) and second, their positive response on headache development at the three-year follow-up to distinguish between stroke-attributed and non-stroke-attributed headache. The first group included patients who reported headache both at stroke onset and at the three-year follow-up. The second group included patients who had not reported headache at stroke onset, but reported novel headache at the three-year follow-up.
The intensity of headache was classified as “mild” if the patients scored 3 or below on the numeric rating scale (NRS), “moderate” with a score between 4 and 7, and “severe” with a score of 8 or higher (32).
The HIT-6 scale (range 36–78) was used as a measurement of impact of headache on daily life. A score below 50 indicated “no or little impact,” a score of 50–55 “to have some impact,” a score of 56–59 “to have substantial impact,” and a score above 60 “to have severe impact” on the daily life of patients (31,33).
While depression was not directly measured, possible depression was assessed by evaluation of self-reported use of antidepressant medicine both at stroke onset and at the three-year follow-up.
Headache was classified as probable migraine (G43.83) or probable tension-type headache (G.44.28), using the criteria from the second edition of The International Headache Classification (ICHD-2) (18). Patients presenting both with probable migraine and probable tension-type headache were classified as mixed headache. Patients who could not be classified as probable migraine, tension-type or mixed headache were categorized as having other headache.
Headache medication overuse was diagnosed based on the self-reported use of headache relief medication as ≥15 days or triptans and/or opiates ≥10 days per month as well as on an underlying novel headache frequency of 14 days or more per month.
Statistical analysis
Data were analyzed with STATA 11 software (StataCorp LP, College Station, TX, USA). Pearson’s χ2 test or Fisher’s exact test was conducted for comparison of categorical variables depending on group sizes. T-test and Wilcoxon rank-sum were applied for continuous variables. Odds ratio (OR) was used to estimate risk factors. Two-tailed probability (p) values <0.05 were considered significant. Missing data were less than 4.5% and evident from the results.
Results
Study population
A total of 640 patients were assessed for inclusion in the study (Figure 1); 299 patients were included and 275 completed the six-month follow-up (4). The questionnaire was sent out to the 256 surviving patients three years after stroke. Five were excluded because of dementia, lack of communication skills and understanding, and 29 patients did not respond. The questionnaire was completed and returned by 216 patients, while six patients responded during a phone interview, resulting in a response rate of 88.4% and an average time for follow-up at 1097.5 days (median 10th and 90th percentiles: 1065–1129 days). There was no difference in gender (53.6% versus 65.5% of patients were male (p = 0.225, χ2)) or age (mean 68.1 years versus 65.0 years within patients lost to follow-up (p = 0.239, t-test)) between the 222 patients who completed the study and the 29 patients lost to follow-up.
Patient flowchart.
Pre-existing headache
Twenty-three percent (52/222) of patients reported that they suffered from headache prior to stroke at the three-year follow-up. Twenty-one percent (11/52) of patients reported worsening of headache after stroke, 30.8% (16/52) reported no change in headache severity, and 48.1% (25/52) found their headache to be milder after stroke. The HIT-6 score showed that the headache had severe impact (≥60 points) in 25.5%, substantial impact (56–59 points) in 15.7%, some impact (50–55 points) in 17.6%, and no to little impact (≤50 points) in 41.2% of patients on their daily life.
Novel headache three years after stroke
At the three-year follow-up, 26 of the 222 patients (11.7%) reported having experienced novel headache after their stroke. Pre-existing headache was more common (53.9%) in patients reporting novel headache compared with patients without novel headache (19.6%) (p < 0.001, χ2). A higher occurrence of hemorrhage in the group of patients with novel headache compared with the group without novel headache was found, but the difference was not statistically significant (15.4% versus 9.2%; p = 0.32, χ2). No significant differences in stroke characteristics or risk factors were seen between the two groups of patients except for atrial fibrillation with a significantly lower occurrence in the group with novel headache (11.8% versus 13.4%; p = 0.035, χ2). A total of 34.6% (nine of 26) of the patients took antidepressants daily, and only one of these patients was already prescribed antidepressants prior to stroke onset. Regular use of antidepressants prior to stroke was not a significant risk factor for development of novel headache (OR = 1.24; 95% confidence interval (CI) = 0.29–4.10).
Patient characteristics.
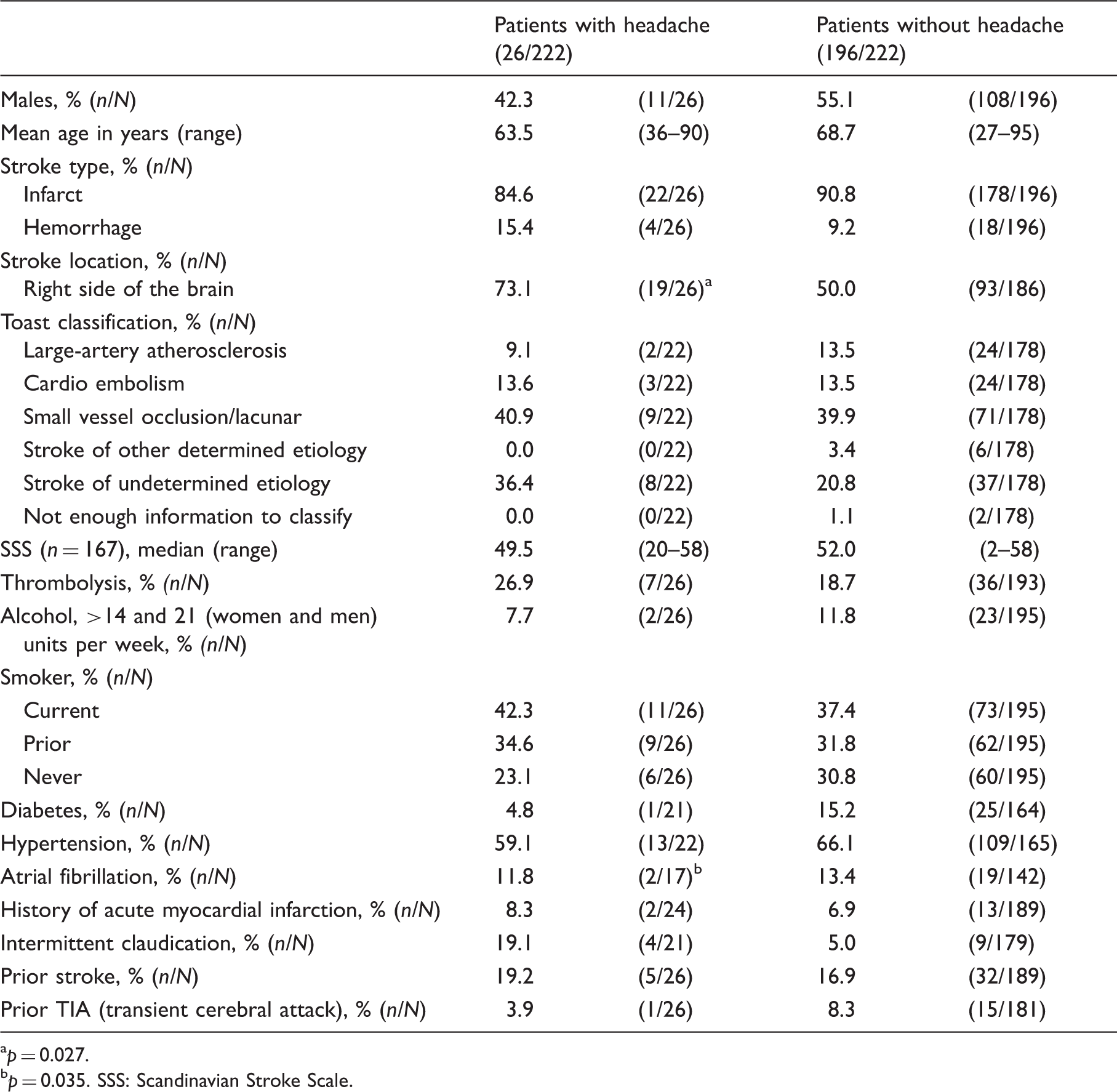
p = 0.027.
p = 0.035. SSS: Scandinavian Stroke Scale.
The consent to access the Danish National Prescription Registry for obtaining information on dipyridamole use was returned by 84.7% of patients (188/222). The 15 patients with hemorrhage were excluded from the analysis, leaving a total of 48% (83/173) of patients who were prescribed dipyridamole around the time of the three-year follow-up. No significant difference in dipyridamole consumption between patients with and without novel headache was found (55.0% versus 47.1%, p = 0.50, χ2).
Of the 26 patients with novel headache, 16 had stroke-attributed headache and 10 non-stroke-attributed headache. The two groups will be described in the following section.
Stroke-attributed headache
A total of 7.2% (16/222) of patients reported stroke-attributed headache, with a frequency of daily headache in 18.8% of patients, while 81.2% reported having headache two to 14 days per month (Table 2). The headache lasted less than one hour in 18.8% of patients, less than one day in 31.2%, one or more days at a time in 12.5%, was constant in 12.5%, and varied in 25%. The headache was bilateral in 43.8% and unilateral in 56.2% of patients. According to CT or MR scans, the infarction or hemorrhage was located in the frontal cerebral area in 18.8% of patients, in the temporal cerebral area in 50%, and in the posterior cerebral area in 12.5%, whereas the scans did not show infarction or hemorrhage in 18.7% of patients. The right side was affected in 56.3% of the patients with headache (nos. 1, 6–9, 10–12, and 15). Headache, infarct, and hemorrhage locations are shown in Figure 2.
Scans of 16 patients with stroke-attributed headache. The black lines enclose the location of the stroke. The white sagittal lines show the location of the headache. The white diagonally lines illustrate the location of alternating side headache. Summary of the 26 patients with novel headache three years after stroke. Self reported onset at the three-year follow-up;1= At stroke onset; 2= following stroke and more than 6 months ago; 3=for less than 6 month ago; 4= do not remember Numeric rating scale: 1= mild (NRS 0-3), 2=moderate (NRS 4-7) & 3=severe (NRS 8-10). Average = average of intensity within the last 4 weeks; worst= highest intensity within the last 4 weeks; ongoing= intensity while filling out questionnaire. Pulsating= pulsating or throbbing Other character= burning, cutting, hurting, shooting and sense of “floating brain matter” (only patient no. 26 reported the latter) Headache Impact Test-6 (score range 36–78); No/little impact≤50 points, some impact=50–55 points, substantial impact=56–59 points, severe impact ≥ 60 points. TTH= tension-type headache; M= migraine; mixed= tension-type headache co-existing with migraine; other=unable to classify. Regular headache medication overuse (intake of regular pain medication ≥ 15 days or triptans and/or opiates ≥ 10 per month).
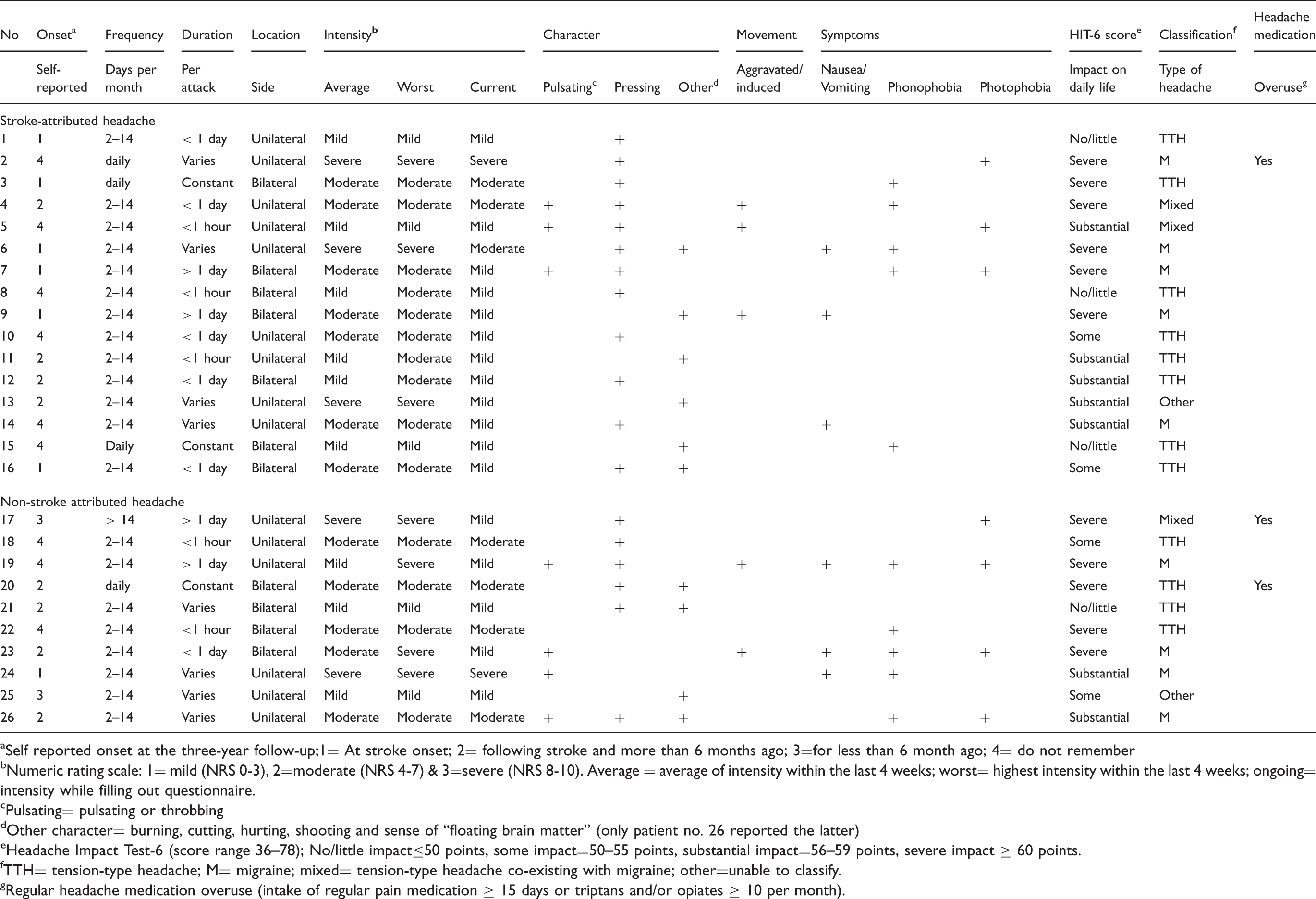
Mean pain intensity within the last four weeks prior to follow-up was 4.5 (NRS, 0–10 (range 2–9)) and 62.5% of patients reported a moderate to severe intensity (NRS ≥4). The headache was described as pressing by 75%, pulsating by 18.8%, and as various other characteristics by 6.2% of patients (Table 2). Only 18.8% of patients reported the headache to be aggravated or induced by movement. Nausea or vomiting was reported by 18.8% of patients, phonophobia affected 31.2%, and photophobia 18.8%.
Types of headache.

Medication intake for the 26 patients with novel headache.

E.g. neck pain, back pain, and knee pain. Antithrombotic prophylaxis containing acetylsalicylic acid is not included due to the low dose.
Regular medication overuse: ≥ 15 days or triptans and/or opiates ≥ 10 days per month and an underlying novel headache frequency of 14 days or more per month.
Non steroidal anti-inflammatory drugs.
For transdermal administration every second day.
Tramadol.
Oxycodon.
The average HIT-6 scale score was 58 (range 36–78), with 37.5% of patients reporting severe impact on daily life, 31.2% substantial impact, 12.5% some impact, and 18.8% no or little impact.
The risk of developing stroke-attributed headache in patients with pre-existing headache was 17.3% (nine of 52; 95% CI = 8.2%–30.3%) compared with 4.1% (seven of 170; 95% CI = 1.7%–8.3%) in patients without pre-existing headache.
Non-stroke-attributed headache
Ten patients reported non-stroke-attributed headache. One patient reported daily headache, one patient headache more than 14 days per month, and eight patients headache between two and 14 days per month (Table 2). The headache lasted less than one hour for two of the patients, less than a day for one patient, one or more days at a time in two patients, was constant in one other and varied in duration for four patients. The headache was bilateral in 40% and unilateral in 60% of patients.
Mean pain intensity in the last four weeks prior to follow-up was 5.5 (range 3–8), and 70% of patients experienced a moderate to severe pain intensity (NRS ≥4). Headache was described as pulsating in 40% of patients, pressing in 60%, and in addition other characters such as burning or cutting were used. Movement-induced or -aggravated headache was reported in 20% of patients. Headache was associated with nausea or vomiting in 30%, phonophobia in 50%, and photophobia in 40% of patients.
Probable migraine was found in four patients (40.0%), probable tension-type headache was found in four patients, and one of them also had medication-overuse headache. Mixed headache was found in one patient with an additional diagnosis of medication-overuse headache (Table 4). Other headache was found in one patient (Table 3).
Median HIT-6 score was 59 (range 42–66) with severe impact on daily life in 50% of patients, substantial impact in 20%, some impact in 20%, and no or little impact in 10%.
Discussion
The main finding in our prospective cohort was that 11.7% of patients (26/222) reported novel headache, and 61.5% of these patients (16/26) had stroke-attributed headache while 38.5% had non-stroke-attributed headache three years after stroke. Novel headache in 11.7% of patients is much lower compared with the 23.3% of patients two years after stroke reported by Widar et al. (16). Our results are consistent with the results of Naess et al., who found headache in 10.8% of patients; however, none of the studies distinguished between stroke-attributed and non-stroke-attributed headache (13,16).
Novel headache was regarded as stroke-attributed with the origin at stroke onset in 62% of patients with novel headache (16/26). Probable tension-type headache was the leading diagnosis when having stroke-attributed headache (50%). Probable migraine (40%) and probable tension-type headache (40%) were equally dominant in the group with non-stroke-attributed headache. Interestingly, Widar and colleagues (16) found only tension-type headache in their patients, and in our study we also found headache with migraine characteristics; however, in only a small number of the patients (9/26).
The majority of stroke-attributed headache was due to infarctions or hemorrhages in the right temporal side of the brain according to Figure 2. Beyond this, no relation between the location of headache and the infarction or hemorrhage was apparent. Ideally, a new scan should have been performed in the present study to determine the location of stroke in patients in whom the initial scan did not show any stroke as well as to determine any secondary strokes that might have influenced the development of headache. It is of interest to note that in a study by Arboix et al. (34), the frequency of headache was higher in lacunar infarctions located in the deep brain gray matter or brainstem compared to lacunar infarctions located in the supratentorial white matter. The authors suggested that the higher frequency of headache in deep gray matter might be related to a higher glutamate concentration in gray matter than in the supratentorial white matter and that the excitotoxic action of glutamate may contribute to the difference between gray and white matter. This is an interesting hypothesis that needs further studies.
Headache medication-overuse headache was found in 11.5% (three of 26) of patients with novel headache. In order to determine medication-overuse headache, the IHS diagnostic criteria have to be fulfilled, e.g. knowledge of development or marked worsening of headache during medication overuse, cessation of consumption, and an evaluation of improvement of headache two months after cessation, and thus we cannot make a final diagnosis of medication-overuse headache in this study.
The majority of patients with pre-existing headache reported the headache to be less bothersome three years after their stroke. The reason for this change is not clear. Structural changes in the vascular system of the brain or a psychological stress factor may play a role in this less intense experience of headache after stroke. More thorough information on pre-existing headache would have enabled us to classify the type of headache and compare pre-existing headache with novel headache to discuss the possibility of the novel headache being a reactivation or impairment of the prior headache. However, a questionnaire concerning both pre-existing and novel headache was not possible in this vulnerable patient group.
Pre-existing depression requiring treatment was not a risk factor for developing novel headache three years after stroke (OR = 1.24; 95% CI = 0.29–4.10). A comparison of depression among patients with and without novel headache would be ideal for future studies to assess the possibility of depression, resulting in an increased incidence of headache. We can conclude that 34.6% (nine of 26) of patients took antidepressants on a regular basis, which is in accordance with a review by Hackett et al. (2005), who found a pooled estimate of 34.0% in the long-term phase after stroke (35). Admittedly, we cannot determine the indication for prescribing the medicine.
Headache due to dipyridamole has been reported by Acheson et al. (21) and Theis et al. (36) to disappear or decrease significantly within the first 14 days, which may explain the lack of difference in dipyridamole consumption between patients with and without novel headache three years after stroke.
The strength of the present study is the high response rate and high completeness of variables plus the explicit questions on novel headache to distinguish between pre-existing and post-stroke headache. A postal survey has some methodological limitations, which also applies to the present study, e.g. the questionnaire could be filled out by proxies and one or more questions could be misunderstood, leading to potential bias. Furthermore, there is a risk of recall bias and, and in this study a potential overestimation of the frequency of headache following stroke. However, in previous studies the reported frequency of headache was not higher than other types of pain (13,16,29).
Conclusion
Novel headache affects 12% of patients three years after stroke, and is attributed to the stroke in 61.5% of patients. Tension-type headache is the most common type of headache in patients with stroke-attributed headache, affecting half of the patients. Medication-overuse headache was reported by 11.5% of patients. Dipyridamole did not seem to cause persistent headache following stroke.
Clinical implications
Novel headache following stroke affects 12% of patients. Stroke-attributed headache affects 7.2% of patients. Stroke-attributed headache mimics tension-type headache. Dipyridamole has no significant influence on the incidence of headache following stroke.
Footnotes
Funding
The study was supported by a grant from the Danish Headache Society without any involvement in the study on their part.
Conflict of interest
None declared.
Acknowledgements
The authors would like to thank Emilia Horjales-Araujo, MSc Biol., Lic.Med., PhD, and Cathrine Baastrup, Msc Pharmacology, PhD, for statistical and technical support; Research Secretary Helle O. Andersen for revision of the manuscript; and graphic designer Ken Kragsfeldt for the illustration.