
Abstract
Purpose
Our aim was to review the existing literature to document oxygen’s therapeutic effect on cluster headache.
Method
A PubMed search resulted in 28 hits, and from these and their references we found in total 11 relevant studies. We included six studies that investigated the efficacy of oxygen treatment. One study is observational and the remaining five are RCTs. Another five studies were on hyperbaric oxygen treatment hereof two case studies.
Conclusion
Oxygen therapy can be administered at different flow rates. Three studies investigate the effect of low-flow oxygen, 6–7 l/min, and found a positive response in 56%, 75% and 82%, respectively, of the patients. One study investigates high-flow oxygen, 12 l/min, and found efficacy in 78% of attacks. The effect of hyperbaric oxygen therapy has been investigated in a few small studies and there is evidence only for an acute, but not a prophylactic effect. Despite the fact that only a few high-quality RCT studies are available, oxygen treatment is close to an ideal treatment because it is effective and safe. However, sufferers of cluster headache do not always have access to oxygen because of logistic and financial concerns.
Background
Cluster headache (CH) is a primary headache disorder that is markedly underdiagnosed and undertreated. The headache is characterized by strictly unilateral attacks of severe pain in the retroorbital region accompanied by ipsilateral autonomic symptoms and restlessness, each attack lasting between 15 and 180 minutes. CH may manifest itself as episodic cluster headache (ECH) or chronic cluster headache (CCH). In ECH there is an episodic pattern of CH bouts and during the bout a patient may experience multiple CH attacks a day. Between the bouts the patient is headache free (1). Typically, the attacks have both a circadian and circannual rhythm (2). In CCH the attacks are present for more than one year without an attack-free period of more than one month (1). There are six times more ECH patients than CCH patients (3).
Oxygen’s mechanism of action is unknown. Several studies have investigated the mechanism and proposed different theories of how oxygen alleviates the pain and cranial autonomic symptoms of CH. The older studies indicate that oxygen is a vasoconstrictor (4–6). These studies are based on measurements of cerebral blood flow and arterial pulsation with photoplethysmograph. Schuh-Hofer et al. showed that oxygen inhibits neurogenic plasma protein extravasation in the dura mater of rats, which was interpreted as a decrease in neurogenic inflammation (7) but confirmatory studies are lacking. In a recent study Akerman et al. showed that oxygen does not have the expected direct effect on the afferent trigeminal nerve fibers; however, it does have a direct inhibitory effect on the cranial parasympathetic nerve fibers (8). Thus, it would seem that oxygen acts as a neuro-modulator acting on the neurotransmitter levels and via deactivation of the trigemino-autonomic reflex-arch. Therefore, it is possible that oxygen either activates a terminating factor of the CH attack or it inhibits an activating mechanism.
CH treatment consists of acute intervention and transitional and maintenance prophylaxis. Oxygen is an acute treatment for CH and is the first line of treatment together with injectable triptans. The acute treatment aims to treat the ongoing pain and other symptoms of the attack (9). Transitional prophylaxis is a short-term treatment, which can interrupt the cluster period, for example high-dose prednisolone (10). The transitional treatment is primarily given at the same time as the start-up of the maintenance prophylaxis. Maintenance prophylaxis is given in the CH periods and the purpose is to reduce the attack frequency and intensity. First choice is the calcium channel blocker verapamil, and the effectiveness is relatively well documented (11–13); however, the effect of the other prophylactic therapies such as lithium is only sparsely documented.
The aim of this paper is to review the literature and expand our knowledge of oxygen as a potent acute treatment of CH attacks.
Search strategy
Normobaric oxygen treatment.

CH: cluster headache; ECH: episodic cluster headache; CCH: chronic cluster headache.
Hyperbaric oxygen treatment.
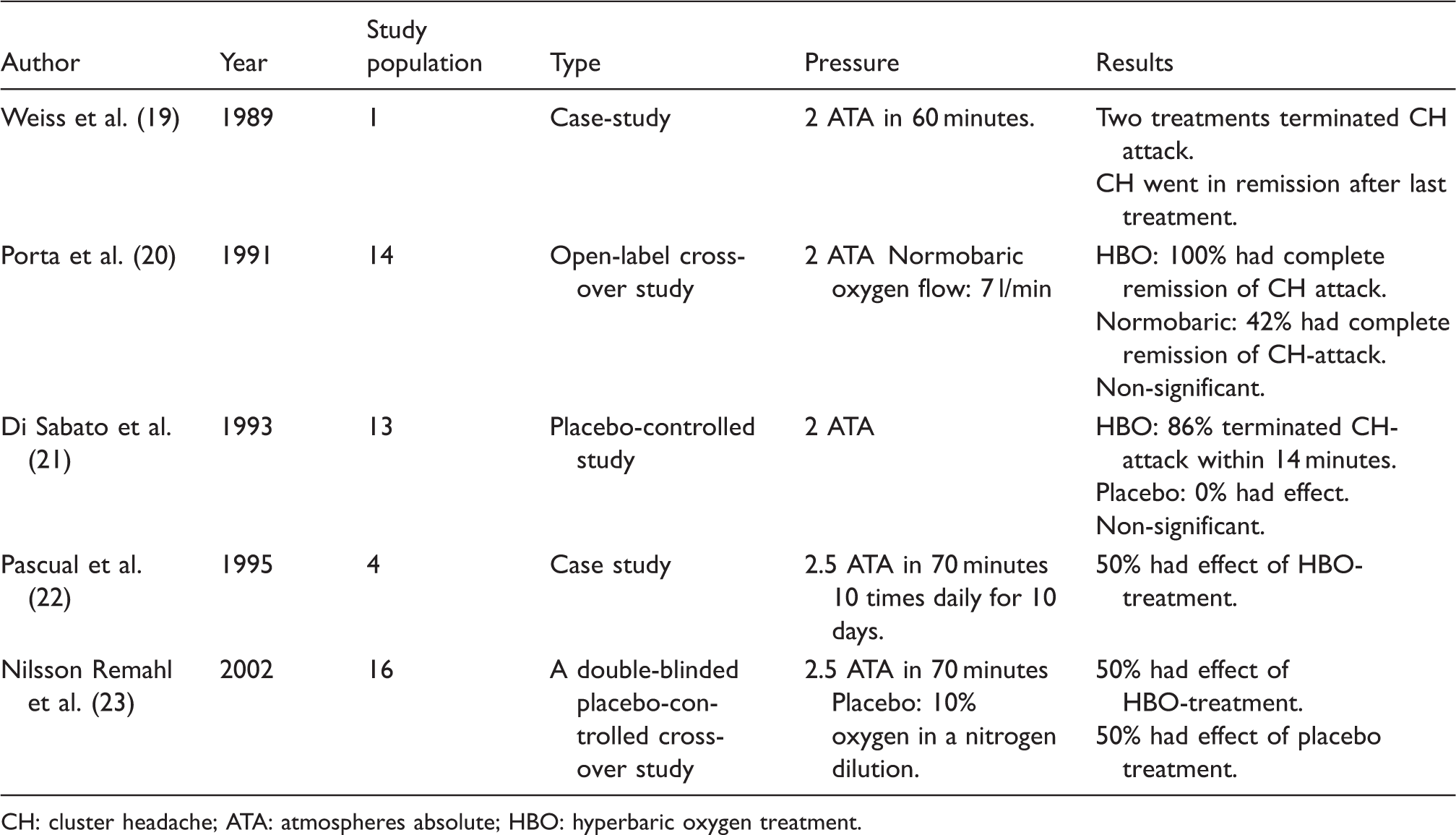
CH: cluster headache; ATA: atmospheres absolute; HBO: hyperbaric oxygen treatment.
Risk of bias assessment.

L: low risk of bias; H: high risk of bias; ?: Unclear risk of bias.
The Cochrane analysis includes the headings “Blinding of outcome assessment (detection bias) (mortality)” and “Incomplete outcome data addressed (attrition bias) (longer-term outcome (>6 weeks))”. These are non-applicable in regard to the review literature.
Normobaric oxygen treatment
Treating headache with oxygen was first described in 1940 (24,25), which is before the description of CH in “Histaminic cephalgia” by Horton (26). In 1981 Kudrow published his landmark study on oxygen treatment, which proved the efficacy of oxygen treatment at a flow rate of 7 l/min (14). The study consists of two sub-studies. The first sub-study is interventional, where 52 CH patients attempted to treat 10 CH attacks with 100% oxygen for 15 minutes. Three-quarters of the patients had complete or almost complete cessation of pain in at least seven out of 10 CH attacks, and 62% had aborted the attack within seven minutes. The time window of treatment success is not explicitly described; however, it appears that 75% had an effect within 15 minutes. The second sub-study is an open-label cross-over study that compares oxygen to ergotamine in a 15-minute treatment period. In total 82% had an effect with oxygen and 70% had an effect with ergotamine; however, the difference was not significant. The peak response to oxygen was within four to six minutes while the peak response to ergotamine was 10 to 12 minutes after administration. Altogether the trial consisted of 102 CH patients and of these 78% had an effect with oxygen treatment. In 1985 Fogan conducted a double-blind, placebo-controlled, cross-over study in which 100% oxygen was compared to atmospheric air at a flow rate of 6 l/min (15). Significantly, and confirming Kudrow’s earlier results, 56% of the study population experienced complete or substantial relief in a minimum of 80% of their attacks and only 7% had the same response to placebo. The lower response rate to oxygen inhalation could be caused by the difference in flow rate.
In 2004 Rozen published a case report describing three CH patients who were refractory to oxygen inhalation at low-flow rates (7–10 l/min) (16). The three patients tried to terminate CH attacks with high-flow oxygen (14–15 l/min) in an unknown amount of time. Two out of three experienced complete headache relief and the third individual experienced 70%–100% relief. All of the results were reproducible in the same patients. Thus, treatment with high-flow oxygen could be an effective alternative to patients who do not achieve effect at low-flow rates. Cohen et al. recently investigated high-flow oxygen as an acute treatment in a double-blind, randomized, placebo-controlled, cross-over trial (17). This trial compared high-flow 100% oxygen (12 l/min) to air. The authors reported that in 78% of the attacks the patients achieved freedom from pain or adequate relief at 15 minutes when treating a CH attack with high-flow oxygen while only 20% had the same response to placebo. These results are statistically and clinically significant and the study is the first to prove the efficacy of high-flow oxygen treatment.
While it seems quite certain that the flow rate is indeed important, the way oxygen is administered may also play a role. A newly published pilot study with a study population of four patients (18) investigated a new delivery method, the oxygen demand valve, that supports hyperventilation by delivering oxygen according to demand (respiration rate and tidal volume). The mask delivers 100% oxygen at flow rates between 0 to 160 l/min. The pilot study was an open-label, cross-over trial that compared high-flow continuous-flow oxygen delivered via non-rebreather facial mask to demand valve oxygen. Oxygen delivered via demand valve appeared to be an effective acute treatment for CH, with faster response time and higher rates of pain freedom compared to continuous-flow oxygen (18). Demand valve oxygen therapy also eliminated the cranial autonomic symptoms in two out of four CCH patients and reduced, but did not eliminate them, in the two other patients. Continuous-flow oxygen did reduce cranial autonomic symptoms, but none had resolution of these. The pilot trial was underpowered and no firm conclusions can be drawn so the findings should be confirmed in a larger, controlled study.
Together, these five studies provide strong evidence for the treatment of CH with oxygen therapy. It has even been investigated whether cold air in itself has an effect (27). The study found no difference in efficacy of cold air compared to oxygen inhalation delivered at a flow rate of 6 l/min. This study had a population size of 10 individuals and there are no confirming or subsequent studies. CH is regarded as a relatively rare condition and the cyclic nature creates some unique, practical problems for the conduction of trials because treatment must be applied during the cluster-bout when patients are severely affected. This can cause a large dropout rate. The small study populations make a statistical analysis of the treatment response in the different subgroups practically impossible; however, an epidemiological survey did not identify a gender difference in oxygen response (28). In the studies mentioned above there was no difference in efficacy between patients who used prophylaxis and those who did not (14,17). In the trial by Fogan the patients were not on prophylactic treatment and in Cohen et al.’s study patients with ECH discontinued prophylaxis one week prior to the study; however, CCH patients were allowed to stay on stable-dose prophylactics during the trial. All four trials were conducted on an outpatient basis. This could be a study limitation because it is unknown whether patients complied with the instructions. On the contrary, in a normal setting oxygen treatment will mainly take place at home. It is usually not practical to ask patients to visit a clinic to treat their cluster attacks but it may be valuable for compliance and trial observations (pain onset, treatment cycle, accompanying symptoms). In three out of the four trials there is no information on smoking history or how long it took from pain debut to treatment initiation, even though these factors are clinically known to influence the oxygen response (14,29). Kudrow highlighted that early initiation of oxygen treatment is very important for optimal efficacy and termination of the CH attack. A weakness in the studies investigating low-flow oxygen treatment is that they do not exclude CH patients with short attacks; a short attack could be interpreted as a false-positive response to oxygen, as it may terminate spontaneously. However, this weakness should be eliminated by the controlled cross-over design.
In all the studies no serious adverse events related to oxygen treatment were observed. In Cohen’s study only two adverse events were possibly related to the treatment. The possible related adverse event was changed headache characteristics, which the patients describe as “Prolonged ‘spikier’ [sic] pain” and “Head felt more tender than if had taken injection.” None of them required further action to be taken. However, Kudrow observed a phenomenon called rebound headache, occurring in 25% of his population (14), which is not described in the four other papers. A recent study of rebound headache found that only 4.4% of CH patients suffer from rebound headache defined as a more rapid than usual reoccurrence of a CH-attack after successful treatment with oxygen (30). The discrepancy may be due to better administration or higher flow rates; however, the study also suggests underreporting as an explanation since rebound headache is rarely mentioned since Kudrow’s original study (14). The mask type used in the three later studies was a non-rebreather mask; however, it is not mentioned which type of mask Kudrow used. This may affect the occurrence of rebound headache, but it has not been investigated further. Geerlings et al. (30) found that oxygen treatment increased the daily attack frequency and that the interval until the next CH attack was on average around 15 hours shorter. Kudrow observed that a young ECH patient had a greater chance of a successful response to oxygen than an older CCH patient (14). Two retrospective epidemiological studies suggested that positive predictors were smoking history, short attacks and no interictal pain (29) and negative predictors were found to be nausea/vomiting and restlessness (31). A recent prospective cross-sectional study did not confirm these findings; however, it suggested that there is a negative correlation between the occurrence of photo- and phonophobia and a positive oxygen response (32).
An ideal acute treatment of CH should be fast-acting, easily accessible, have a low side effect profile, have no daily maximal usages and should be effective in the majority of CH patients. None of the currently available acute treatments for CH fulfill all of the criteria listed above. Oxygen is, however, shown to be an effective, fast-acting, acute treatment with a low side effect profile in adults, no limits of maximal usage and no contraindications (33,34). One could imagine that smoking might be a safety issue; however, in the literature no such incidence has been reported, nor is it our clinical experience.
Oxygen is not as easily accessible as injectable sumatriptan, but is equally effective (35), cheaper and does not have a maximum usage of twice per day, as well as the side effects and contraindications that hamper the triptans (10,36). Despite these positive properties many CH patients do not use oxygen and there are big differences from country to country. Studies from the United States, Canada, Great Britain and Germany show that a range of 31%–71% of CH patients have tried oxygen therapy (37–40) and only 31.4% of CH patients who have experience with injectable sumatriptan and oxygen actually prefer oxygen over sumatriptan (41). A study by Gallagher et al. found that 76% of CH patients reported significant relief with oxygen treatment at a flow rate of 8 l/min, but only 31% of the patients continued using oxygen inhalation (42). This apparent self-exclusion from oxygen treatment could have many causes, but the most important seem to be of a logistic and economic nature (38). Patients describe the use of analgesics as more convenient and easier versus the cumbersome use of oxygen (42). Admittedly, getting hold of both prescription and oxygen cylinders can be difficult and costly in some countries (37) although oxygen treatment is one of the safest, most effective and probably cost-saving treatments that exists.
Normobaric oxygen is not traditionally used as a treatment for other types of headache (33,43–45); however, it may have an effect on migraine patients who have cranial autonomic symptoms related to the migraine attack (46–48). However, this effect has not been investigated in a placebo-controlled study.
Hyperbaric oxygen treatment
Another way of administering oxygen is to deliver it at higher pressures than one atmosphere absolute (ATA), so-called hyperbaric oxygen treatment (HBO). Three minor trials and two case studies illustrate the possible effect of HBO treatment of CH (19–23). Three of these investigated HBO as an acute therapy, and the two most recent publications examine the prophylactic effect. The first article regarding HBO treatment was a case study (19) that describes an ECH patient who in the middle of a bout received two treatments of 100% oxygen at a pressure of two ATA for 60 minutes. The ECH patient was refractory to inhalation of normobaric oxygen. Each treatment resulted in relief both of the headache and the autonomic symptoms. The first treatment session was followed by a rebound CH attack and after the second HBO therapy her headache bout went into complete remission. The publication does not provide any concrete evidence for HBO treatment, but it did spur further research.
Two later studies support the effectiveness of HBO in the acute treatment of CH at 2 ATA, but the results were not significant because of small sample sizes (20,21). In the study by Porta et al., all 14 participants experienced pain relief after only one to two minutes and the mean duration was 6.2 minutes but the autonomic symptoms continued for several more minutes (20). The mean duration before treatment start was 25 minutes, which gives a reduction of 55 minutes compared to the mean duration of the attack without treatment. However, 25 minutes before treatment initiation is long compared to normobaric oxygen and sumatriptan injections that have an effect within 15 minutes and are applied normally within minutes. DiSabato et al. conducted a placebo-controlled study in 13 patients in whom 86% experienced an interruption of the attack when treating with HBO at a pressure of 2.5 ATA. None in the placebo-group had an interruption in the CH attack (21). The six patients, who had an effect with HBO, reported being headache free for a minimum of four days after HBO treatment. Three patients reported a complete remission of the CH bout at the two-month follow-up (21). This suggested that HBO might also be an effective prophylaxis; however, this could be a spontaneous remission since all were ECH patients.
In the available literature there are two other studies that describe the prophylactic effect of HBO treatment (22,23). Pascual et al. conducted a case study in which two out of four cases showed a positive response to HBO treatment. One went into total remission for a month and the other experienced decreased frequency and duration of attacks during the two weeks of HBO sessions; however, the duration and frequency returned to normal two days after the HBO treatment (22). The two cases with poor response to HBO treatment consisted of one non-responder and another patient who had only a minor effect on frequency during the two weeks of HBO sessions. In a double-blind, placebo-controlled, cross-over study from 2002, the preventive effect of HBO was questioned as there was no significant difference between the HBO group and the sham group. The sham treatment was 10% oxygen in nitrogen delivered at 2.5 ATA, which is equal to hyperbaric normoxic conditions. Fifty percent did show an effect with the hyperbaric condition regardless of the oxygen level (23). The result may suggest two findings: one, that the hyperbaric condition per se may have a preventive effect or two, the study has a high placebo response, since CH patients are known to have a placebo response of up to 43% (49).
The HBO studies do not provide significant results favoring HBO for prevention whereas HBO as an acute treatment seems to have an effect. In these five studies only one CH patient experienced an adverse event in the form of ear dysbarism (22), which are barotraumas that happens when there is an inability to equalize pressure (50).
The major disadvantages of HBO therapy are that the equipment is costly and stationary, which makes it unlikely that it will be available outside of a hospital setting. This is a big hindrance for HBO as an acute therapy; however, if HBO does indeed have a prophylactic effect it could be offered at specialized centers for medically refractory CH patients.
Conclusion
Treatment of CH with oxygen inhalation has been known for many years but only few investigations have been conducted. It has been found that oxygen treatment is effective as an acute treatment of CH and that some CH patients may need high-flow therapy. All identified studies, both those investigating normobaric and HBO treatment, have relatively small study populations. Therefore predictors for successful outcome have not yet been identified. Not every CH sufferer uses oxygen, because the cylinders are unpractical, relatively expensive and the patients feel limited in their daily life. However, because of its excellent interaction and side effect profile, oxygen treatment can be combined with other acute medication and should in our opinion be offered to all CH patients.
The mechanisms of action of oxygen are not clarified; however, the overall data indicate that oxygen inhibits the neurogenic inflammation and the trigeminal autonomic reflexes by acting on parasympathetic outflow. Understanding the effect of oxygen on CH may provide important insights into CH pathophysiology, and more research is needed. In the past 15 years there have been some improvements in this field; however, there is still a tremendous unmet need for better CH treatment and much more knowledge of oxygen regarding the mechanism of action, identification of responders and optimization of administration.
Clinical implications
Oxygen treatment is effective as an acute treatment of cluster headache (CH). Some CH patients may need high-flow therapy. Oxygen has an excellent interaction and side effect profile. Hyperbaric oxygen treatment (HBO) as an acute treatment seems to have an effect; however, as a preventive method HBO does not seem to be efficient. Some results indicate that oxygen inhibits neurogenic inflammation and the trigeminal autonomic reflexes by acting on parasympathetic outflow.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
Mads Barloese: Unrestricted research grant from AGA-Lindegas.
Rigmor H. Jensen: Lectures for Pfizer, Berline-Chemie, Allergan, Merck and Autonomic Technologies. Member of advisory boards of Autonomic Technologies, Medotech, NeuroCore and Linde Gas ltd.
Anja S. Petersen has nothing to declare.