
Abstract
Objective
Inhalation of oxygen is highly effective in cluster headache, a subtype of trigeminal autonomic cephalgias. Since oxygen has no effect on nociceptive pain, the mechanism of action is still unknown. The present study investigated whether oxygen inhalation modifies the trigeminal autonomic reflex arc in healthy volunteers.
Methods
21 healthy volunteers participated in a randomized, placebo controlled, double-blind, cross-over, and within-subject study design. In a randomized order demand valve inhalation of 100% oxygen or medical air were administered. Capillary blood samples were collected to control for blood gas changes. Cranial parasympathetic output (lacrimation) was provoked using kinetic oscillation stimulation of the nasal mucosa. Standardized measurement of lacrimation between baseline and kinetic oscillation stimulation served as a measure of induced cranial autonomic output.
Results
There was no significant difference in parasympathetic output after oxygen inhalation when compared to inhalation of medical air.
Conclusion
The inhalation of 100% oxygen does not affect the parasympathetic reflex arc of the trigeminal autonomic reflex.
Introduction
Cluster headache is a trigeminal autonomic cephalgia (TAC) and characterized by severe unilateral head pain associated with ipsilateral autonomic symptoms (1). Inhalation of 100% oxygen is an effective treatment of attacks and results in freedom from pain after 15 min in 78% of the attacks (2). One hundred percent oxygen inhalation has also been reported to be effective in migraine patients, particularly in those who show cranial autonomic symptoms (3,4). This suggests a link between oxygen efficacy and the occurrence of parasympathetic symptoms in headache attacks. However, the exact mechanism of action is not yet known. Another effective treatment of episodic cluster headache (5,6) and migraine (7,8) is non-invasive vagal nerve stimulation (nVNS). A recent study showed that non-invasive vagal nerve stimulation exerts a quantifiable physiologically effect and significantly modulates the parasympathetic arc of the trigeminal autonomic reflex (9). Animal studies investigating oxygen inhalation suggest that it might likewise act specifically on the parasympathetic arc of the trigeminal autonomic reflex, rather than on the trigeminal nerve itself (10). Furthermore, a significant change in lacrimal sac blood flow induced by the stimulation of the superior salivatory nucleus (SSN) has been shown during oxygen inhalation in these animal studies (10), suggesting that oxygen might act specifically on parasympathetic/facial nerve projections and that this effect may inhibit both trigeminovascular activation and activation of the autonomic pathway (10). This would indeed explain why patients with cluster headache and migraine patients with cranial autonomic symptoms benefit from oxygen inhalation. Consequently, the aim of the present study was to investigate whether the inhalation of 100% oxygen modulates specifically the cranial parasympathetic system in healthy volunteers.
Methods
The study was approved by the local ethics committee in Hamburg, Germany (PV 5522) and was conducted in accordance with the Declaration of Helsinki. Prior to the first study session a written informed consent was obtained, and participants were allowed to discontinue the study at any time.

Study Design.
Results
Effects of oxygen inhalation on provoked lacrimation
All volunteers completed the study, 20 were included in the final data analysis (age range 19–34 years, mean ± SD age: 24.85 ± 3.99, 15 female). One participant had to be excluded because of dizziness and syncopal problems during blood sampling.
The ipsilateral lacrimation difference before-after for both conditions is shown in Figure 2. There was no significant difference between lacrimation after oxygen inhalation and the inhalation of medical air at any timepoint.

Ipsilateral KOS-induced lacrimation increase.
Blood gas analysis
Blood samples were collected from all participants; however, due to technical issues during analysis, all four sample results were obtained for only 15 participants. Figure 3 shows changes in pH, pCO2 and pO2 for these 15 volunteers. pO2 values significantly increased during inhalation of 100% oxygen (101.47 ± 1.83 vs. 409.81 ± 29.18 [p < 0.001]), whereas no significant change occurred after inhalation of placebo (99.72 ± 1.80 vs. 105.07 ± 2.56). In both conditions a significant decrease of pCO2 (37.06 ± 0.85 vs. 33.79 ± 1.54 [p = 0.007] for medical air; 37.03 ± 0.65 vs. 34.31 ± 1.30 [p = 0.013] for oxygen), was found, however post-inhalation values did not significantly differ between the two sessions (33.79 ± 1.54 [air] 34.31 ± 1.30 [O2]).

pCO2 and pO2 after inhalation of medical air.
No adverse events occurred during either the inhalation of medical air or oxygen, nor during KOS. In 52.5% of the sessions participants were right in guessing which gas they inhaled during the experimental sessions (Figures 4 and 5).
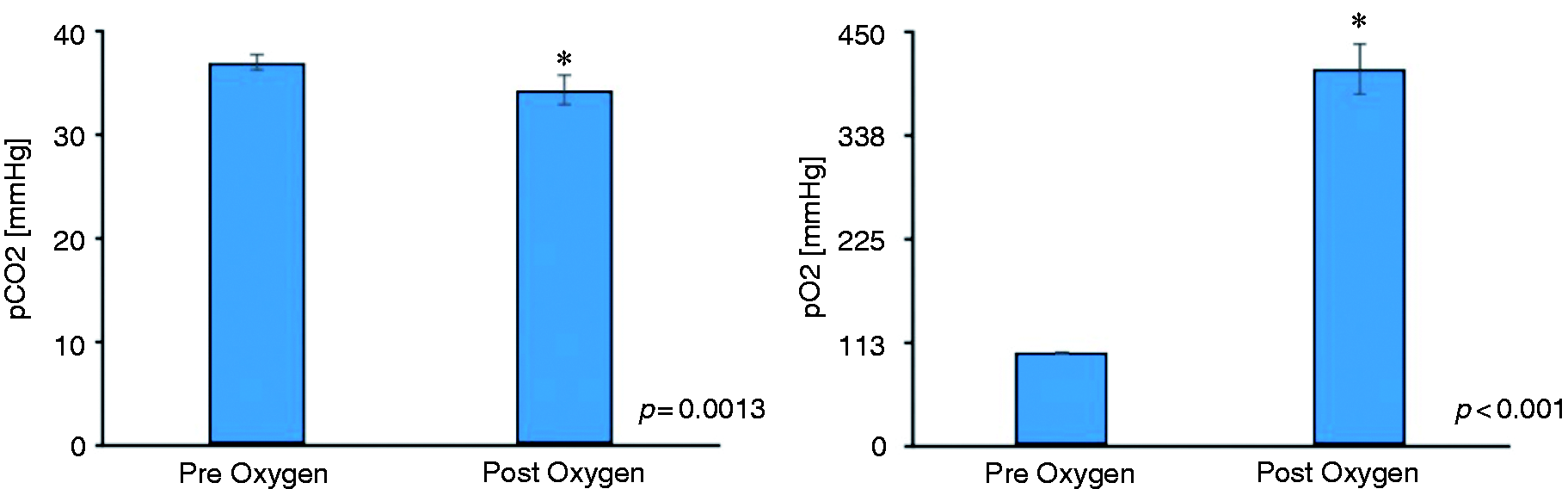
pCO2 and pO2 after inhalation of oxygen.

Blood Gas Analysis post oxygen vs. post medical air.
Discussion
Our main finding is that inhalation of 100% oxygen has no impact on the trigeminal autonomic reflex arc in healthy participants, which was stimulated by KOS.
Previous studies have shown that KOS stimulation elicits a robust quantifiable trigeminal autonomic response, i.e. lacrimation (12,13) and that this response can be modified by nVNS. In a similar way, this effect has also shown to be true for oxygen in an animal model (10): In this study, oxygen treatment inhibited neuronal firing at the trigeminocervical complex (TCC), but only when activated via SSN stimulation. Oxygen treatment did not affect trigeminal nerve activation (i.e. did not act as a pain killer) or dural or lacrimal blood flow (10). These results suggest that oxygen acts on the trigeminal autonomic reflex rather than the trigeminovascular system (14). However, our study does not confirm that this mechanism of action is also true for humans. Although oxygen intervention is a proven therapeutic approach for trigeminal autonomic cluster headache, the exact mechanism and site of action remains unclear.
One possible explanation for the discrepancy between the animal model and our work may be the strength and nature of the trigeminal autonomic response itself. While KOS stimulation is largely well tolerated by participants, the type and quality of a cluster headache attack, accompanied by autonomic symptoms, is significantly more severe. This leads to greater activation of the trigeminal autonomic system with increased recruitment of trigeminal afferents and efferents. This in turn could lead to a change in the populations of neurons recruited, which have been suggested to have a different affinity to oxygen (10). Again, it remains unclear whether these different neuronal populations also exist in humans. Another obvious limitation is that a cluster attack is intrinsically generated and numerous central nervous structures are involved. The KOS method, on the other hand, is an extrinsic stimulus that has been shown to be unable to trigger cluster attacks in a previous study (15), suggesting that a peripheral stimulus/trigeminal autonomic activation is not sufficient to generate cluster attacks and that the cluster headache pathophysiology is far more complicated. Another possible assumption could be that oxygen is not effective at all via the trigeminal autonomic reflex arc for the acute therapy of cluster headache. The plasma level of the neuropeptide calcitonin-gene related peptide (CGRP) is increased during the cluster attack (16) and seems to be modified at least indirectly by oxygen (17). Studies have shown that after administration of sumatriptan or inhalation of oxygen, CGRP levels returned to normal (17). Whether CGRP release is a cause, or a consequence of the cluster attack cannot be concluded, but oxygen may be involved the trigeminovascular coupling through CGRP.
We note that in some participants the Schirmer’s test was already filled after two minutes, and although these participants would show ongoing lacrimation, this could not be measured. However, we found no statistical difference at any time-point between groups and, moreover, a cross-over design was also used to correct for this. We additionally performed statistical approaches to handle missing values and sensitivity analyses and this did not alter our results.
In conclusion our results indicate that the inhalation of 100% oxygen does not affect the autonomic pathway of the trigeminal autonomic reflex in healthy volunteers in an experimental condition using KOS. Since we investigated healthy volunteers, we cannot make inferences regarding the pathophysiological activation of the trigeminal autonomic reflex in patient with cluster headache. Further studies, including patients, are necessary in order to make more precise conclusions about the exact mode of action of oxygen for the treatment of cluster headache.
Key findings
Inhalation of oxygen is highly effective in cluster headache, a subtype of trigeminal autonomic cephalgias. Animal studies suggest that oxygen may act on the cranial parasympathetic system rather than the trigeminovascular system. Our data show that in humans, the inhalation of 100% oxygen has no effect on experimental activation of the cranial parasympathetic system.