
Abstract
Background: Cluster headache is a rare primary headache disorder characterized by recurrent, stereotyped short-lasting attacks of severe, unilateral head pain accompanied by autonomic symptoms.
Methods/results: Ophthalmic features such as conjunctival injection, lacrimation, ptosis and miosis occur in the vast majority of patients with cluster headache, whereas co-existent ocular movement disorders are rare.
Conclusions: To the best of our knowledge, only two documented cases of cluster headache with external ocular movement disorders have been reported. We describe herein an additional case with this unusual finding and discuss the putative pathophysiology of cluster headache associated with ophthalmoparesis.
Introduction
Cluster headache is an uncommon primary headache disorder characterized by recurrent, stereotyped short-lasting attacks of severe, unilateral head pain accompanied by autonomic symptoms. Ophthalmic features such as conjunctival injection, lacrimation, ptosis and miosis occur in the vast majority of patients with cluster headache, whereas co-existent ocular movement disorders are rare. To date, there have only been two reported cases of ocular movement disorders associated with cluster headache (1,2). We describe herein an additional case of this unusual association, further highlighting the variable spectrum of features seen within this headache disorder. Institutional Review Board (IRB) approval was not required as single case reports receiving standard clinical care are exempt per Montefiore Medical Center’s IRB policy.
Case report
A 23-year-old man with two previous cycles of episodic cluster headache was hospitalized for the evaluation and treatment of a recurrent, severe headache associated with new-onset diplopia. Two months prior to admission, the patient had developed daily attacks of strictly unilateral, excruciating, throbbing and sharp pain. The pain was centered mainly around and behind the left orbit with radiation into the ophthalmic and mandibular distributions of the left trigeminal nerve. These headaches regularly occurred from one to three times per night, typically around 9
There was a prior history of episodic cluster headache for two years in which circannual cluster periods began each September and lasted for three months. The patient also had a six-year history of migraine without aura, which occurred twice annually. Family history revealed that the patient’s mother suffered from migraine headaches as well. The patient smoked half a pack of cigarettes daily for eight years but denied drinking alcohol and using illicit drugs.
On examination in the emergency department (ED), he was afebrile with a blood pressure of 160/80 mmHg and a pulse of 65 beats per minute. General medical examination performed interictally following the prolonged cluster headache revealed a thin young African-American man who was seated on a hospital stretcher in obvious distress with his hands pressed against his left eye in a dimly lit ED room. Neurological examination demonstrated partial ptosis, miosis, conjunctival injection and severe monocular photophobia, all on the left. In addition, the left eye was slightly esotropic on primary gaze, with restricted abduction of the left eye on left lateral gaze. Severe binocular horizontal diplopia was present in both right and left directions of gaze. When the patient fixated with the paralytic left eye there was secondary deviation of the right eye to the right. All aspects of third, fourth, fifth and seventh cranial nerve function were intact. The remainder of the neurologic examination was normal. Routine chest X-ray, cerebrospinal fluid examination and hematological tests including complete blood count, coagulation studies, ANA, ACE level, erythrocyte sedimentation rate and C-reactive protein were unremarkable. MRI studies performed with and without gadolinium, as well as MR angiography (MRA) of the brain were unrevealing. Specifically, the meninges and cavernous sinus were entirely within normal limits, and there was no side-to-side asymmetry on the MRA involving the cavernous, supraclinoid or petrous segment of the internal carotid artery.
On the day of admission the patient was started on dexamethasone 6 mg intravenous (IV) every 6 hours hours, valproic acid 500 mg IV every 8 hours, and sustained-release verapamil 240 mg daily. Although the patient achieved significant relief from the pain on the second day of treatment, the sixth nerve palsy and ipsilateral ptosis persisted. He was discharged five days after admission with an oral steroid taper and sustained-release verapamil. On follow-up two weeks later, the patient was free from headache with partial recovery of the left sixth nerve palsy and ipsilateral ptosis. Unfortunately, the patient was lost to follow-up after this visit.
Discussion
The history of recurrent, stereotyped, short-lived attacks occurring in clusters, the strictly unilateral orbital pain, the prominent ipsilateral autonomic features and the unremarkable diagnostic studies suggest that this is a trigeminal autonomic cephalalgia (3). The duration and frequency of attacks and the response to treatment support the diagnosis of a specific trigeminal autonomic cephalalgia, namely episodic cluster headache. The presence of monocular photophobia supports the diagnosis (4). The atypical features in this patient are the development of persistent sixth nerve palsy and prolonged ipsilateral ptosis during an unusually long attack of cluster headache.
Sixth nerve palsies can result from lesions in the nerve fascicle, subarachnoid space, cavernous sinus, superior orbital fissure or orbit itself. The pathophysiologic differential diagnosis of a sixth nerve palsy includes ophthalmoplegic migraine, infectious processes, vascular abnormalities, neoplastic diseases, derangements of intracranial pressure and inflammatory conditions, such as Tolosa-Hunt syndrome and orbital pseudotumor (5). While migraine should be considered because of the unilateral location and throbbing quality of his headaches, the short duration, prominent autonomic features, fixed laterality, occurrence of attacks in clusters and absence of typical migraine features (i.e. aura, nausea, phonophobia) make this diagnosis unlikely. Though infectious, vascular, neoplastic and inflammatory disorders enter into the differential of painful ophthalmoplegia, the laboratory studies and meninges and cavernous sinus were entirely within normal limits in this patient.
Patients with cluster headache and external ocular movement disorders
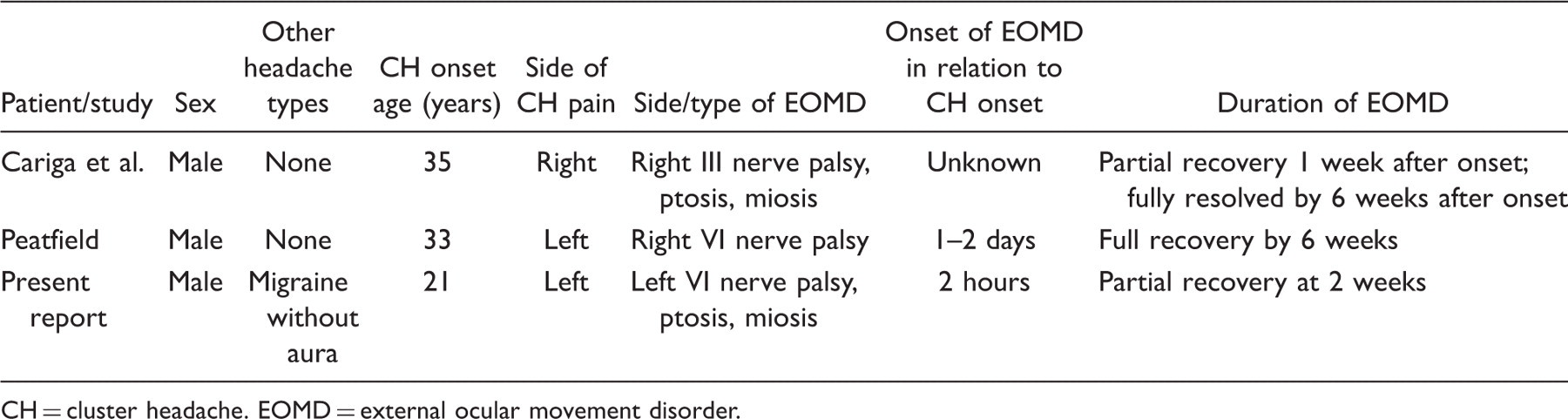
CH = cluster headache. EOMD = external ocular movement disorder.
These three patients have several features in common. All three patients had a history of typical episodic cluster headache and all of them developed an external ocular movement disorder in relation to an attack of cluster headache. In addition, the pain from the attacks of cluster headache resolved well before the transient external ocular movement disorder, with the latter often resolving gradually over several weeks. Of the three patients, the external ocular movement disorder involved the sixth nerve in two and the third nerve in one and was ipsilateral to the side of the pain in two and contralateral in one. In two of the three patients, the external ocular movement disorder was associated with ipsilateral ptosis and miosis.
A pathophysiologic model for ocular motor palsy in association with cluster headache must account for a number of clinical features seen in our patient and in previous reports. During the cluster attack, dilation and inflammation within the cavernous sinus may influence the cavernous segment of the carotid artery and the adjacent structures (6,7). Both positron emission tomography (PET) and MRA data have demonstrated that dilation of the intracavernous internal carotid artery occurs bilaterally both in cluster headache and in response to experimental pain in the first division of the trigeminal nerve (8). Thus, when the cavernous sinus is involved in cluster headache as an element of the trigeminal-autonomic reflex (9), the effects may be bilateral even though the pain is almost exclusively unilateral.
Autonomic symptoms in cluster headache reflect activation of the parasympathetic nervous system and dysfunction of the sympathetic nervous system. Trigeminal sensory fibers from the dura mater and cerebral vessels have their cell bodies in the trigeminal ganglion and synapse in the trigeminal cervical complex. The second-order neurons then synapse in the superior salivatory nucleus. From there, fibers from parasympathetic neurons travel with the facial nerve through the sphenopalatine ganglion to the lacrimal glands and nasal mucosa, causing lacrimation and rhinorrhea (9).
Studies in both monkeys and humans have demonstrated a small plexus of parasympathetic fibers within the cavernous sinus. In human post-mortem studies, this tiny ganglion, located laterally to the internal carotid artery and dorsally to the abducens nerve, contains neurons which stain with antibodies to vasoactive intestinal peptide (VIP) and choline acetyltransferase (ChAT), indicating a parasympathetic function. Parasympathetic nerve fibers originating in this ganglion cell may innervate the intracranial segment of the internal carotid artery and its intracranial ramifications. This ganglion has neural connections with the ophthalmic division of the trigeminal nerve, the abducens nerve, and the sphenopalatine ganglion. Fibers from the sphenopalatine ganglion may reach this small parasympathetic ganglion via the rami orbitales, causing a release of both VIP and acetylcholine, both of which are potent vasodilators (10). Activation of this pathway is a result of central activation of the parasympathetic nervous system at the level of the superior salivatory nucleus, which is thought to dilate the intracavernous carotid artery both through direct effects and by stimulating the release of histamine from mast cells (11). The sympathetic fibers traveling along the intracavernous carotid artery may subsequently become compressed during this process, giving rise to the partial Horner’s syndrome that is often seen in cluster headache. Like the carotid sympathetic plexus, the abducens nerve may be an “innocent bystander”, compressed by the inflammatory and vasodilatory changes that occur within the cavernous sinus during a cluster headache attack.
This model accounts for the onset of ophthalmoparesis during the attack of cluster headache when the cavernous carotid artery is dilated. It accounts for the involvement of both the third and sixth cranial nerves as both traverse the cavernous sinus. Because bilateral cavernous sinus involvement has been reported in cluster headache, this mechanism could account for both the ipsilateral and contralateral cranial nerve palsies seen in the reported cases. Ophthalmoparesis begins during attacks of cluster headache (two hours to two days from attack onset) and persists up to six weeks.
This case and a review of prior similar cases demonstrate that the spectrum of ophthalmic involvement in cluster headache includes ocular motor palsy. Patients with both cluster headache and ocular motor palsy should be evaluated for other conditions that cause ophthalmoparesis and painful ophthalmoplegia. In patients with long-standing cluster headache who develop ocular motor palsy during an attack, ocular motor palsy attributed to cluster headache should be considered after a negative work-up.