
Abstract
Background
Headache is one of the most common symptoms after cocaine use.
Methods
We investigated headache frequency and characteristics and the correlation between headache and acute cocaine intake in a cross-sectional study in a consecutive series of chronic cocaine users.
Results
Participation rate was 94.1%. Of the 80 subjects enrolled, 72 (90%) reported current headaches, in most cases migraine or probable migraine without aura. Of these 72, 29 (40.3%) had a headache history, whereas 43 (59.7%) reported de novo headache after beginning to use cocaine. After acute cocaine use, a large percentage of users reported headache attacks: 86.2% of previous headache sufferers (migraine or probable migraine without aura in all cases) and 93% of de novo headache sufferers (migraine/probable migraine without aura = 35; episodic tension-type headache = three patients; cocaine-induced headache= two patients). Most subjects reported that when they used cocaine headaches worsened.
Conclusion
Chronic cocaine use frequently seems to worsen or induce headache with migraine or migraine-like characteristics, probably owing to a serotoninergic and dopaminergic system impairment. In headache sufferers, especially those with migraine headaches, clinicians should enquire into possible cocaine use.
Introduction
As many as 14 million to 21 million people worldwide (0.3%–0.5% of the population aged 15–65 years) use cocaine. Cocaine use is the most frequent cause of drug-related emergency department visits (1). Cocaine blocks catecholamine (dopamine, norepinephrine) and serotonin reuptake and exerts toxic activity at many receptors throughout the central nervous system (CNS) and cardiovascular systems (1). Besides seizures, focal neurological deficits, dizziness and transient loss of consciousness, among the most common neurological complications of cocaine use is headache (2).
Owing to the heterogeneous definitions, methods and populations in various studies, the precise frequency of headache in cocaine users remains debatable, reportedly ranging from 0.8% to 75% (2–8). The growing burden of cocaine addiction, not only in high-income countries, and the greater awareness of headache as a cocaine use symptom led the second edition of the International Classification of Headache Disorders (ICHD-II) (9) to include the diagnosis of cocaine-induced headache among the headaches attributed to a substance or to its withdrawal. Cocaine-induced headache is defined as a headache that develops within an hour after cocaine use and lasts at the most 72 hours, manifesting with at least one of the following symptoms: bilaterality, frontotemporal location, pulsating quality and worsening with physical activity. Since the ICHD-II criteria were published no study has investigated headache in cocaine users (9). Having more information on the frequency of headache in cocaine users would help clinically in diagnosing otherwise unexplainable atypical headaches.
To determine headache frequency, type and characteristics as diagnosed by the ICHD-II criteria (9) in chronic cocaine users, we conducted a cross-sectional study in a consecutive series of chronic cocaine users attending a drug addiction service. We assessed the association between the acute and long-term effects of cocaine use and headache in subjects with neither lifetime nor current headache, lifetime and current headache and de novo headache.
Methods
We conducted a cross-sectional study on all consecutive chronic cocaine consumers according to the Diagnostic and Statistical Manual of Psychiatric Disorders, fourth edition, text revision (DSM IV-TR) criteria (10) attending the Cocaine Addiction Service of the Drug Addiction Service, 20th District, UOS Municipio 17, ASL RME, Rome, from 1 June 2011 to 31 December 2012. Subjects attending this municipal service come mostly from the Lazio region (especially from the city of Rome). They have a wide age range (18 to 70 years) and heterogeneous socioeconomic status. At their first visit to the clinic or at follow-up, after a complete physical and neurological examination, subjects were seen by a psychiatrist (VO) who gathered detailed information on cocaine use, concomitant disorders and treatments (concentrating on drugs known to influence headache including antiepileptics, antidepressants and neuroleptics) then interviewed by a neurologist (LF) using a semi-structured questionnaire (11) focused on the presence of lifetime or current headache (≥1 headache attack in the past three months) or both, and detailing all headache characteristics. The association between cocaine use and headache was investigated by asking the following questions: Did your headaches begin after you started using cocaine? Did your previous headaches change their course when you began using cocaine? Did acute cocaine consumption trigger a headache attack? and Did you ever use cocaine during a headache attack? If so, what happened? Subjects were divided into three groups reporting neither lifetime nor current headache (group 0), lifetime and current headache (group 1) and de novo headache (individuals in whom headache developed only after cocaine use began) (group 2).
The protocol was approved by the local institutional review board and procedures were conducted in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki. All subjects gave their informed consent before their inclusion in the study.
Statistics
Data were first analyzed to evaluate differences in characteristics between the three groups and then only between subjects with lifetime and current headache and those with de novo headache (groups 1 and 2). A one-way analysis of variance (ANOVA) was used for continuous variables and a chi-square test for categorical variables. A post-hoc analysis was also run to check differences between groups. A Pearson’s correlation analysis was used to seek a possible correlation between age at headache onset and age at first and continuous use of cocaine in the group with de novo headache. A multiple regression analysis was also used to evaluate the effects of these predictor variables on the association between cocaine and headache. All data were analyzed with SPSS (version 17.0). A p value ≤0.05 was considered to indicate statistical significance.
Results
Sociodemographic and headache characteristics
Socio-demographic and headache characteristics in 80 chronic cocaine users.

HBV: hepatitis B virus; HCV: hepatitis C virus; SSRI: selective serotonin reuptake inhibitor; SNRI: serotonin-norepinephrine reuptake inhibitor; NS: not significant. ap values by one-way analysis of variance (ANOVA).
Characteristics of cocaine use in 80 chronic users.
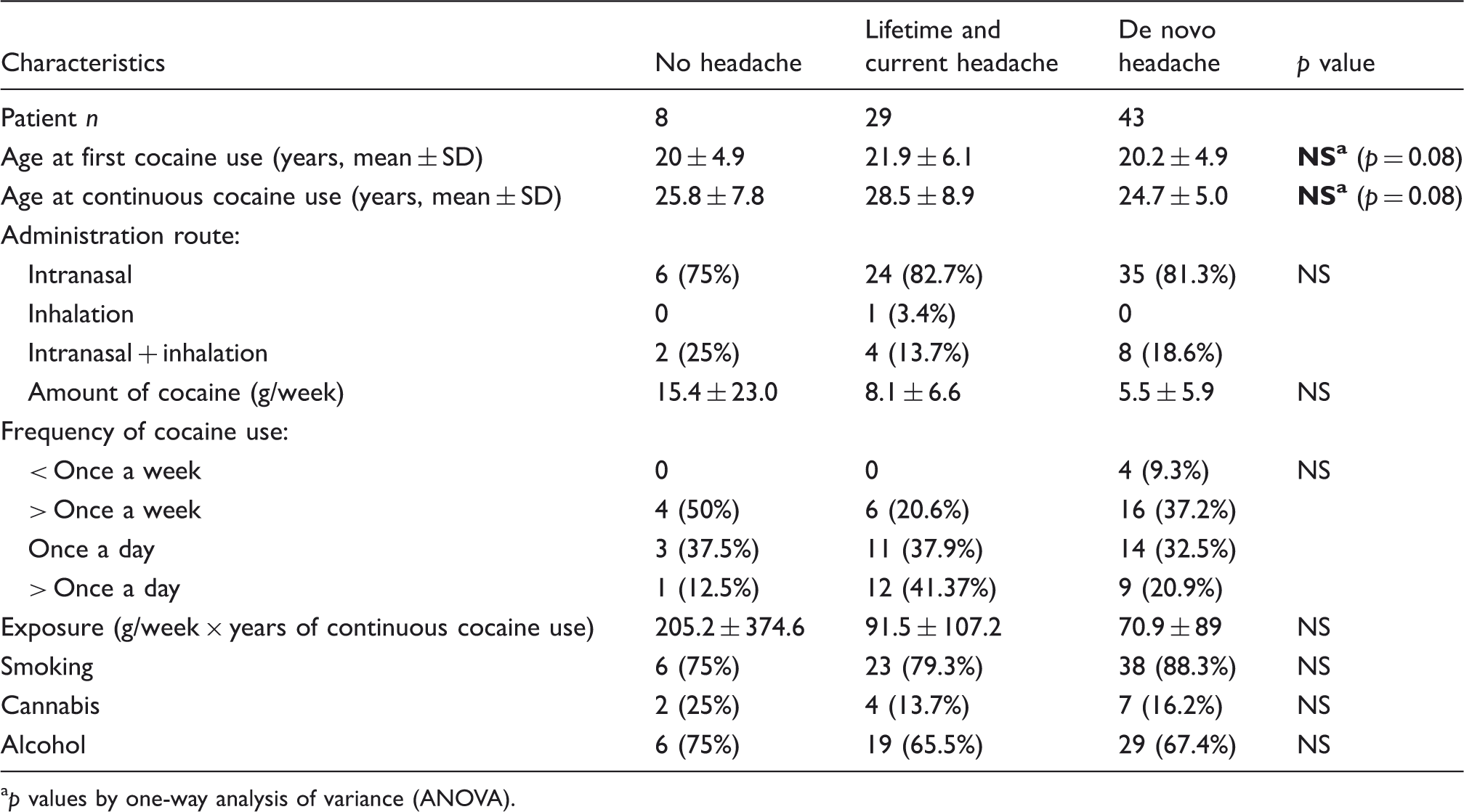
p values by one-way analysis of variance (ANOVA).
Cocaine use and headache onset
The frequency of headache onset after cocaine use differed notably according to headache history. None of the patients who had neither lifetime nor current headache but 25 subjects (86.2%) in the group with previous headache reported experiencing headache after cocaine use. Of these 25 subjects, 11 individuals previously suffering from migraine or probable migraine without aura reported having a more severe headache but slightly shorter than usual, whereas 14 referred experiencing a headache similar to their usual one. Headache frequency was reported as unchanged in 17 out of 25 patients and increased in eight (in two cases headache frequency was >15 days per month). As many as 40 subjects (93%) in the de novo group reported that headaches began after they started cocaine use: 35 had migraine without aura or probable migraine without aura, three episodic tension-type headache and two cocaine-induced headache (Table 1).
Effects of acute cocaine use during a spontaneous headache attack
In the group of chronic cocaine users reporting previous headache, 29 (100%) took cocaine at least once during a headache attack. Of these 29, 20 subjects (69%) reported that after taking cocaine their headaches worsened, five (17.2%) that they improved, and four (13.8%) that they remained unchanged. Of the 43 patients in the de novo headache group, 29 took cocaine at least once during a headache attack, 16 patients (55.2%) reported that headaches worsened, 10 (34.5%) that they improved, and three (10.3%) that they remained unchanged (Table 1).
One-way ANOVA and Pearson’s correlation analysis
No differences were found between the three groups for socio-demographic characteristics (Table 1), cocaine doses, administration routes and cocaine use frequency. Combining cocaine with cannabis or alcohol had no influence on headache characteristics (Table 2).The post-hoc analysis showed that several headache features differed significantly according to whether patients had previous headache: Compared with the de novo group, patients with previous headaches had significantly longer headache duration (p = 0.02), more severe head pain (p = 0.001), more frequent vomiting (p = 0.041), higher analgesic use (p = 0.04) and lower response to analgesics (p = 0.047).
We found a trend for a different age at first and continuous cocaine use between the three groups (p = 0.08), in particular between the group reporting previous headache and the de novo headache group (p = 0.081). In the de novo headache group, Pearson’s analysis disclosed a linear correlation between age at headache onset and age at first cocaine use (r = 0.401; p = 0.008) and between age at headache onset and age at continuous cocaine use (r = 0.367; p = 0.016). The multiple regression analysis identified as the major predictors for age at headache onset in the de novo headache group, age at first cocaine use and age at continuous cocaine use (R2 = 18%; p = 0.02).
The corresponding regression equation is: age at headache onset = 12.1+ 0.55 age at first cocaine use+ 0.33 age at continuous cocaine use.
Discussion
Our study, specifically designed to investigate headache frequency, type and characteristics in a consecutive series of chronic cocaine users by examining and interviewing them directly and applying the ICHD-II criteria (9), suggests that headache affects chronic cocaine users far more frequently than previously reported (90% vs from 0.8% to 75%) (3–8). This discrepancy probably reflects heterogeneity in study design (retrospective studies, clinical surveys with self-report questionnaires, case reports), routes of cocaine administration (intranasal, intravenous, inhalation), amounts, use frequency (sporadic, chronic) and concomitant polysubstance abuse (2–8).
Unlike previous studies (2–8), we investigated the acute and long-term effects of cocaine on headache in chronic consumers. When considering the long-term effects we showed that cocaine addiction induces de novo headache in 59.7% of previously unaffected individuals and in 40.3% of headache sufferers headache worsens. Conversely, in 93% of de novo headache sufferers and in 86.2% of headache individuals, acute cocaine intake triggers headache. According to our subjects’ answers to self-reported questionnaires, rather than relieving headache pain during a spontaneous headache attack, as some suggest (7,12,13), cocaine actually worsens headache pain.
Another new clinically useful finding in our study is the headache clinical characterization in chronic cocaine users. The most frequently reported headaches are migraine without aura and probable migraine without aura. Unexpectedly, cocaine-induced headache, as classified by the ICHD-II criteria (9), seems exceedingly rare in chronic cocaine users (2.2%) because in most of our patients (87.5%) headache developed >2 hours after acute cocaine use (in 81.2% >4 hours after) and almost one-third of subjects referred to pain in sites other than the frontotemporal location. Many previous and de novo headache sufferers (86.2% and 67.4%) reported self-medicating their cocaine-related migraine attacks with analgesics. This interesting finding underlines the concern that self-medication without consulting a physician could increase the risks related to drug interactions and medication overuse.
Although our findings provide no conclusive evidence on how cocaine influences headache, in line with current knowledge we conjecture that especially in migraine it does so by inducing a dopaminergic and serotonergic system imbalance. However, cocaine-induced cardiovascular effects could be theoretically involved.
Whereas acute cocaine administration blocks monoamine reuptake inducing increased dopaminergic and serotoninergic activity (14–16), its chronic use decreases synaptic dopamine and serotonin levels in critical brain circuits. Chronic cocaine use is associated with a reduced dopamine D2 receptor binding potential and, consequently, to decreased dopamine transmission, related to a downregulation connected to dopaminergic pathway supersensitivity (6–20). These changes are more evident in the limbic system, insofar as major reductions have been observed mostly in the striatum with concomitant reduced activity in the orbitofrontal cortex, cingulate gyrus and frontal regions (21). Human and experimental studies provide convincing evidence of a serotoninergic system dysfunction in chronic cocaine consumers (22). Neuroendocrine responsiveness to serotonin releasers is diminished in rats withdrawn from repeated cocaine injections (23), and similar findings have been reported in abstinent human cocaine addicts (24,25). A specific postulated mechanism in migraine is monoaminergic synapse impairment that reduces dopaminergic and serotoninergic tone thus leading to receptor upregulation and hypersensitivity (“empty neuron” condition) (26–31). Given that chronic cocaine use deranges dopaminergic and serotoninergic transmissions, we hypothesize that in headache sufferers chronic cocaine use further compromises monoaminergic neurotransmission, thus worsening pre-existing headache. Conversely, in previously headache-free individuals continuous cocaine use would disrupt dopaminergic and serotoninergic neurotransmission as happens in the “empty neuron” condition, thus lowering the headache threshold in these subjects. This assumption could also explain our finding that the younger the age when sporadic and chronic cocaine use begins the earlier headache develops, because catecholaminergic functional connectivity is disturbed earlier in these subjects. Moreover, a major monoaminergic disruption could account for an increase in headache burden in terms of pain severity, duration and analgesics’ efficacy in subjects with prior headache compared to de novo ones.
As an alternative causative mechanism to explain how chronic cocaine use causes headache, given that we found that headache is in most cases a delayed event, beginning at least four hours after cocaine ingestion, we consider it unlikely that a cocaine-triggered headache attack reflects a potent and immediate sympathomimetic effect or acute vasoconstriction. A more reasonable headache trigger mechanism in chronic cocaine abusers could be serotonin or dopamine release or both characterized by dopamine and serotonin receptor upregulation, due to chronic neurotransmitter impairment.
Despite its strong point—a specific study-design involving direct interviews using the current ICHD-II criteria (9) in consecutive subjects and the detailed patient demographic and clinical assessment—our study has some limitations, for example, the sample size, the lack of sporadic cocaine users as a control group, and the potential recall bias (our study design could eventually have led to overestimating patients with de novo headache or headache worsening). Nor can we exclude effects induced on headache by concomitant medications (e.g. neuroleptics and antiepileptics). All subjects were recruited at their first or follow-up visit and they could have a different clinical profile.
In conclusion, chronic cocaine use seems frequently to worsen or induce headache with migraine or migraine-like characteristics, whereas cocaine-induced headache, as presently classified (9), is a rare event. Given the substantial proportion of young adults in developed countries who use illicit drugs, clinicians should investigate their use in greater depth in all headache suffers, especially those with migraine characteristics.
Clinical implications
Headache affects 90% of chronic cocaine users. Chronic cocaine use seems frequently to worsen or induce headache with migraine or migraine-like characteristics whereas cocaine-induced headache, as presently classified, is a rare event. Clinicians should investigate cocaine use in greater depth in all headache suffers, especially those with migraine characteristics.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
PB has received grants or research support and honoraria or both for lecturing for and has been a consultant and scientific adviser for Merck, Janssen Pharmaceutical Products, Lusofarmaco and Allergan.
Acknowledgment
Thanks are due to Mrs. Alice Crossman for the English revision.