
Abstract
Aim
The aim of this article is to evaluate the effectiveness of a specific multidisciplinary treatment programme for children with headache and to describe the concept and settings of the Children’s Headache Clinic in Denmark.
Method
All new patients were included and evaluations were conducted after six and 12 months. Pharmacological and non-pharmacological treatments were offered by a team of specialists (physicians, headache nurses, a physiotherapist and a psychologist).
Patients
The subjects comprised 169 children (mean age 11.7 (range 4–17), 91 females, 78 males), 39% of whom suffered from chronic headache (≥15 days/month). All children were diagnosed according to the International Classification of Headache Disorders, second edition; 20% had migraine, 34% tension-type headache, 27% mixed headache, 4% medication-overuse headache, and 15% were diagnosed with other types of headaches.
Results
Fifty per cent of the children had an improvement in headache frequency above 50% at six months. By the use of repeated measurement analysis, we found a significant decrease in headache frequency in all of the six headache groups, whereas the increase in quality of life (PedsQL™ 4.0) was significant for the group as a whole.
Conclusion
Though preliminary, the results show a good outcome for multidisciplinary treatment programmes for children who suffer from frequent or chronic headache.
Introduction
Headache is a frequent disorder among children. The overall calculated prevalence of headache in children (3–20 years) is 58% (1).
In Denmark, as in the majority of other countries, most of the children suffering from headache disorders are treated by general practitioners or private practising paediatricians and not many are referred to neurologists. Treating these children is a challenge because headache disorders in children have characteristics that differ from those in adults. Moreover, the International Classification of Headache Disorders, second edition (ICHD-II) (2) is not always used despite having been validated and agreed upon internationally. Misdiagnosis can lead to incorrect treatment strategies with the risk of a bad outcome. Especially, the treatment of chronic or disabling pain in children is a challenge. Chronic pain is often associated with mood disorders, lost social relations and decreased school attendance, and might have profound consequences for the children in every aspect of their daily lives (3,4). Successful treatment is dependent not only on the self-awareness of the child, but also parental support that helps the child adjust and adhere to the given recommendations. Furthermore, successful treatment is time consuming because enquiry into family dynamics, schooling and peer relationships are issues that need to be addressed. The majority of children with episodic headaches can be sufficiently cared for in the primary sector, but some children who are disabled by or suffer from frequent, intractable or rare headache may need a multidisciplinary approach carried out by headache experts in a tertiary setting.
With this in mind, the Children’s Headache Clinic (CHC) was established in Denmark in 2006 as part of the Department of Paediatrics at Glostrup Hospital, but is now located at Herlev Hospital. Both pharmacological and non-pharmacological treatments are offered by a team of specialists that comprises physicians, headache nurses, a physiotherapist and a psychologist.
A number of tertiary multidisciplinary headache clinics for adults have opened worldwide over the last 20 years (5–8). This development follows the suggestions of having a three-tier interdisciplinary system for headache care as recommended by the European Headache Federation in 2011 (9). Outcome research has demonstrated the effectiveness of these multidisciplinary treatment programmes (MTPs) using parameters such as: headache frequency, intensity, quality of life (QoL), anxiety, depression, workdays missed, emergency care visits and medication consumption (5,7,8,10–13). Furthermore, the concept seems to be well accepted and perceived as effective by adult patients (11). Common to all of these clinics is the multidisciplinary aspect, but the programmes vary markedly in duration and content (14).
The authors are aware of the existence of only a few tertiary multidisciplinary clinics worldwide for children with headache. Publications describing the concept, settings and outcome are also limited (15–17).
Aware of the major limitations of an observational study where randomisation is impossible, we still found it relevant and necessary to evaluate the outcome of treatment in our CHC.
This study describes the CHC approach and setting, characterises the new patients received in 2009 and evaluates the effectiveness of a specific MTP.
Methods
Study design
The study features a prospective cohort design with follow-up at six and 12 months.
The CHC setting and concept
CHC is the first clinic in Denmark to offer a multidisciplinary treatment for children suffering from headache in an outpatient hospital setting. The clinic has the capacity to receive 200 new children per year. Children between 0 and 18 years of age are referred from general practice, practising neurologists, practising paediatricians or from other paediatric departments. The main uptake area is the Capital Region of Copenhagen, which has a population of 1.7 million people; nonetheless, children come from all over Denmark, population 5.5 million, if referred to the clinic. Funded by taxes, health care services are free of charge in Denmark.
The multidisciplinary team at CHC comprises two half-time senior doctors with a speciality in headache in children (paediatricians who have specialised in neuropaediatrics), two specialised nurses, one half-time clinical/half-time research physiotherapist, one half-time psychologist, one medical doctor conducting research, one secretary and residents who have clinical consultations supervised by the senior doctors. In general the clinic adheres to the Danish Headache Society’s Treatment Recommendations (18).
The role of the paediatrician is to establish the diagnosis according to the ICHD-II (2) and to conduct a neurological examination, initiate any diagnostic examinations and to be responsible for pharmacological treatment. In general acetaminophen, nonsteroidal anti-inflammatory drugs (NSAIDs), triptans and domperidon are prescribed at the acute headache attacks as appropriate according to diagnosis and previous treatment (18). Furthermore, prophylactic treatments are considered and often initiated in children suffering from headache ≥15 days per month (amitriptylin is used as first choice) or migraine with an attack frequency of about three to four attacks per month (propranolol or flunarizin are used as first choice). Headache nurses conduct separate consultations that focus on lifestyle habits and trigger factors. They instruct in keeping a headache calendar, assess the disability level and address the family’s questions. Overall they monitor the child’s progress and serve as the primary contact to the child and parents. The physiotherapist conducts a primary musculoskeletal examination to detect possible aggravating or causative factors. Physiotherapy interventions focus on patient education in progressive relaxation therapy with or without computer-animated surface-electromyographic (EMG) biofeedback, body awareness, posture-correcting exercises, strength training and fitness planning. Finally, the psychologist works with parents and child within the areas of cognitive-behavioural training, self-efficacy, self-awareness, perceived control, the family’s readiness to change and pain-coping strategies.
The MTP in CHC
The MTP entails all of the various treatment options described above.
Prior to the first consultation, all children and parents receive a diagnostic headache diary similar to the one published by Jensen et al. and are told to record prospectively headache characteristics (19). At their first consultation, the children are met by a paediatrician and a headache nurse. Children are diagnosed according to ICHD-II criteria and pharmacological treatments are initiated/optimised. The first consultation is always followed by a second consultation 14 days later to thoroughly discuss lifestyle habits and trigger factors with the headache nurse. Individualised plans for eliminating/reducing important trigger factors are made and followed. Psychological therapies for children and adolescents and psychological interventions for parents of children and adolescents with chronic headache are used when needed, preceded by discussion among the multidisciplinary team (20). Likewise, physiotherapeutic interventions are initiated if relevant after being discussed among the multidisciplinary team. In addition the children can also be referred to consultants within psychosomatic medicine, psychiatry, dentistry or ophthalmology. Normally, children are followed at least twice a year at physician consultations and two to six times at nurse consultations. However, treatment courses are individually adjusted. If discharged from the clinic, the child is sent with detailed instructions for further primary care follow-up.
Participants
Inclusion
We prospectively included all children referred to the clinic who were seen for the first time from February 2009 to February 2010, and then followed them for 12 months. The cohort includes children with either primary or secondary headache disorders. The five exclusion criteria included: 1) declined to participate (three children); 2) headache free at inclusion (seven children); 3) never signed written consent form (13 children); 4) entered CHC in alternative ways and were not recognised as eligible (four children); and 5) were wrongly referred (two children).
Baseline data
At the initial CHC consultation, baseline data were obtained by the physician through interviews with the parents and child and from the headache diary. If clinical information was too unclear, the child and parents were asked to return after recording headaches in the headache diary for a period. All data were calculated as an average of the prior three months and recorded in a questionnaire. The children were classified into five social categories based on the education and current job status of the parent with the highest socioeconomic status (21). Group I comprises higher professional and managerial workers with extended higher education; group II: professional and lower managerial workers with medium-long education; group III: intermediate occupations, lower supervisory, small employers, farmers; group IV: skilled workers, routine occupations; group V: unskilled workers.
QoL and the burden of disease were determined by the questionnaires PedsQL™ 4.0 (22) and PedMIDAS(23). PedsQL™ 4.0 is a brief 23-item measurement model that evaluates QoL in four areas: physical, emotional, social and school functioning. The answers are converted into a 0–100 total score, where 100 is optimal QoL. In this study children were assisted by a headache nurse, if necessary. Parents and the child/adolescent independently completed the PedsQL™ but completed the PedMIDAS jointly. PedMIDAS comprises six questions about the number of days disabled by headache in school and at home.
If a medication-overuse headache (MOH) was suspected, a three-month withdrawal period was arranged without any bridging prophylactic. A 50% decrease in headache frequency during this period was the cut-off for definition of the MOH diagnosis, which was given retrospectively, as a baseline diagnosis after withdrawal. Children with no effect were rediagnosed and distributed into their primary diagnosis groups.
Follow-up data
Data were recorded during prescheduled face-to-face consultations at six and 12 months with one of the physicians and through a prospectively recorded headache calendar. PedsQL™ and PedMIDAS were recorded again. If the family cancelled or missed follow-up, an effort was made to reach the family for a telephone interview by a physician instead. PedsQL™ and PedMIDAS were later sent by ordinary mail.
Drop-outs
Children were discharged from CHC during the study period for three reasons: 1) successful outcome; 2) upon request; or 3) failure to appear.
Variables
Baseline variables
Headache characteristics, social status, parental marital status, previous treatment, number of days with medication per month, body mass index (BMI), child-reported PedsQL™ 4.0 and parent proxy-reported PedsQL™ 4.0, PedMIDAS (question 1, which indicates missed schooldays because of headache) were primarily used.
Outcome variable
As proposed by Powers et al., we used headache frequency (days/month) and changes in QoL (child-reported PedsQL™ 4.0) as outcome measures (24). Improvement in headache frequency was defined as a reduction ≥1 day/month. Improvement in QoL was defined as an increase ≥ 1 in PedsQL™ total score. PedMIDAS allowed us to register schooldays missed, but this information was not used as an outcome measure because of a reporting problem. All school-age children have a two-month summer holiday in Denmark. Consequently, this introduces bias in the August and September disability reports.
Bias
To minimise recall bias, we used standardised methods for the initial evaluation and follow-ups. This included headache diaries and calendars, as well as face-to-face interviews with parents and the child at baseline and as the primary method in follow-up evaluations. The data in the physician questionnaires were retrospectively controlled for left-outs by the primary author using the individual patient’s journal before being entered into SPSS.
Statistical methods
Quantitative variables following a reasonable normal distribution (child-reported PedsQL™ 4.0, parent proxy-reported PedsQL™ 4.0) are described by mean and standard deviations (SD), while other variables (headache frequency, headache intensity, schooldays missed) are described by median and interquartile range (IQR).
A paired-samples t test was used to test and quantify the differences between PedsQL™ in children and parents.
Headache frequency
For each type of headache, we performed a repeated measurement analysis for binomial counts (count parameter equal to 30, the number of days in a month), with time as a factor. We accounted for inter-individual subject variation by including a random subject level and also adjusted for possible overdispersion. Finally, the analysis was also done for the cohort as a whole. P values for successive changes over time are reported, while predicted mean values are shown in Figure 1 and Table 1.
Headache frequencies. Predicted values from repeated measurement analysis of the individual headache groups. Predicted outcome. After correction for dismissed patients, the predicted means from the repeated measure analysis are illustrated below. Reference group: Baseline. TTH: tension-type headache; MOH: medication-overuse headache; Other headaches: Headaches not classified in the other five groups; FETTH: frequent episodic tension-type headache; CTTH: chronic tension-type headache.

QoL
For each type of headache, we performed a repeated-measures analysis in the form of a mixed linear regression analysis, with time as a factor and subject levels as random effects. Child-reported PedsQL™ was used as a dependent variable in the models. Finally, the analysis was also performed for the cohort as a whole. P values for successive changes over time are reported, and predicted mean values are shown in Figures 2 and 3 and in Table 1. GLIMMIX in SAS was used to analyse headache frequency as an outcome. Other analyses were performed in SPSS 20. A p value less than 5% was considered statistically significant.
Child-reported PedsQL Child-reported PedsQL

Approval
Written informed consent was obtained from all patients. The study was approved by the Danish Data Protection Agency file no. 2009-41-3146.
Results
Participants
During the inclusion period, 198 children had their first consultation at CHC. A total of 169 children were included in the study and 29 children were excluded. The excluded children had a mean age of 10.1 years (SD 3.6, range 2–18); 11 were females and 18 were males. The excluded children were slightly younger and had a predominance of males compared to the included children. Figure 4 presents a flow diagram of the 169 children included. Thirteen were discharged before the six-month follow-up and an additional 26 were discharged before the 12-month follow-up, leaving 156 children for a potential six-month status and 130 for a potential 12-month status. The number of children with registered data is also listed in Figure 4. However, because of oversight, the staff sometimes failed to present the PedsQL™ to families at the clinical consultation and the subsequent failure of parents to return questionnaires by mail means there are missing values for PedsQL™ and schooldays missed.
Flow diagram of participants. The numbers of children who have registered data are shown in percentages.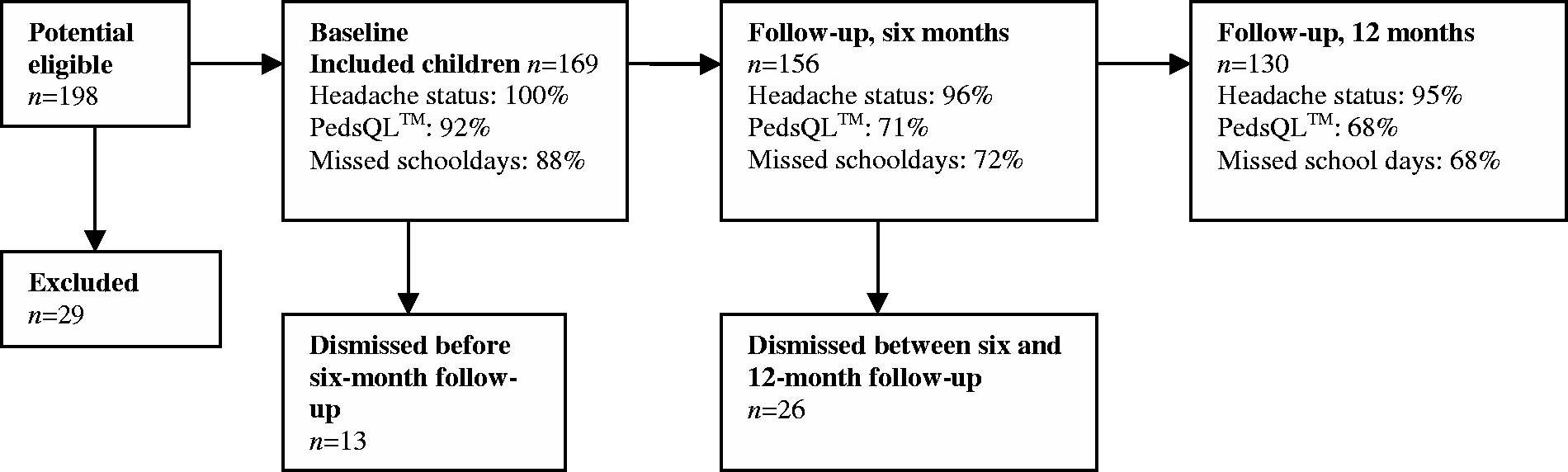
Clinical characterisation of the cohort at initial consultation
We included 91 females and 78 males. The children had a mean age of 11.7 (SD 3.04, range 4–17), and 22/169 (13%) had suffered from headache less than a year before inclusion, while the rest had suffered a median of two years (IQR 1–4, range 1–12) before inclusion. Fifty-two per cent were referred to CHC by their general physician, whereas the rest had been seen by a specialist before referral. The median BMI of all children was 17.8 (IQR 16–20, range 13–69). The children were classified into five social categories. Sixteen per cent were placed in group 1 (the highest socioeconomic status), 30.8% in group 2, 14.2 % in group 3, 20.7% in group 4 and 6.5% in group 5. Sixty-seven per cent of the children were living with both parents and in 86% of the children, both parents were Caucasians. Previous treatments were registered and 88% of the children had tried acetaminophen, 37% NSAIDs, 15% triptans and 3% prophylactic medication, while 14% had tried physiotherapy, 4% had visited a psychologist and 13% had tried alternative treatment strategies.
Participant data.

VAS: visual analogue scale; TTH: tension-type headache; MOH: medication-overuse headache; Other headaches: headaches not classified in the other five groups; FETTH: frequent episodic tension-type headache; CTTH: chronic tension-type headache; SD: standard deviation.
Only one patient at this follow-up.
In the migraine group, 12/34 (35%) had migraine with aura. In the TTH group 33/57 (58%) suffered from chronic TTH. In total, 66/169 (39%) suffered from headache ≥ 15 days/month at referral.
Sixteen children with presumed MOH were initially diagnosed. Seven were successfully treated. However, six completed three months of medication withdrawal and had no effect on headache frequency (did not have MOH), while three children did not return after the first consultation and were therefore discharged.
The six-month follow-up was conducted after a median duration of 184 days (IQR 174–217, range 126–280) and the 12-month follow-up after 372 days (IQR 358–401, range 266–500).
PedsQL™ 4.0 child/parents
At baseline, the children had a mean PedsQL™ of 74.0 (SD 13.4). The parents’ reports of PedsQL™ in their children had a mean of 72.3 (SD 14.5). The difference was significant (p = 0.012), but minimal (mean difference 1.7 (95% confidence interval (CI): 0.4–3.1). The parents seemed to slightly underestimate the QoL of their child.
Effectiveness of the MTP
Improvement in frequency
At six months, 105/150 (70%) of the children had an improvement in headache frequency and 75/150 (50%) had an improvement above 50%. At the 12-month follow-up, 83/124 (67%) of the children had an improvement in headache frequency and 59/124 (48%) had an improvement above 50% compared to baseline.
Table 2 shows headache frequency in the subgroups at the six- and 12-month follow-up.
Directly comparing these medians at specific points in time, however, will not provide us with the correct estimate of outcome. Some children were dismissed during the observation period either because they were cured or because they were recovering markedly. As a result, only children still in need of and interested in further treatment at CHC participated in later follow-ups. Fortunately, the use of a repeated-measurement analysis compensates for this inverse “healthy worker effect” and allows estimation of predicted headache frequencies after correction for dismissed patients between follow-ups, as shown in Figure 1 and Table 1.
All six headache groups had a significant decrease in headache frequency at six months compared to baseline (Table 1). After this point the decreasing effect compared to baseline was still significant for the following groups: migraine, TTH + migraine, MOH and CTTH as well as for the cohort as one large group. The speed of improvement, however, was not as quick subsequently, as illustrated in Figure 1.
Improvement in QoL
At the six-month follow-up, 68/105 (65%) of the children had an increase in QoL but only 5% of the active children had an increase above 50% compared to baseline. In those children still in active treatment at CHC at the 12-month follow-up, 47/85 (55%) of the children had an increased QoL and 5% of the active children had an increase above 50% compared to baseline.
Table 2 shows the child-reported PedsQL™ in the headache groups at the six- and twelve-month follow-ups.
Figure 2 and Table 1 show the predicted child-reported PedsQL™ after correction for dismissed patients between the follow-ups by using a repeated-measurement analysis.
The MOH and the FETTH groups were the only ones that had a significant increase in QoL after six months. After 12 months of treatment, QoL showed a tendency toward improvement in all headache groups compared to baseline, but the effect was not statistically significant.
Looking at the cohort as one large group, there was a significant improvement of 4.0 at six months (p < 0.001) and an improvement of 3.2 at 12 months (p = 0.008) compared to baseline. The baseline PedsQL™ was 74.0 in this model. See Figure 3.
Discussion
The present study shows a significant effect of our MTP for children with migraine, TTH + migraine, MOH, FETTH, CTTH and other headaches.
We found a significant decrease in headache frequency in all of the six headache groups and furthermore a significant increase in QoL for the cohort as a whole.
The most pronounced treatment effect was during the first six months, where the improvement frequency for every other child was more than 50% between baseline and the six-month mark. QoL, however, seemed to improve more slowly. This is not unexpected as re-establishing peer relations and confidence in the future likely take time after pain levels improve.
Another notable finding was the almost curative effect of the three-month medication withdrawal in half of the children with presumed MOH at referral. This illustrates the importance of non-pharmacological and correct pharmacological treatment of headache disorders in children and shows the importance of treating MOH in children.
Thirty-nine per cent of the children suffered from chronic headache at referral. With this high number of children in mind, we found that most of the children in the cohort had tried acetaminophen (paracetamol); however, only one-third of all the children had tried NSAIDs. Furthermore, only 3% had been in prophylactic treatment and only 4% had visited a psychologist. Forty-seven per cent of the children had seen a specialist prior to referral. This emphasises the current need and importance of continued and further distribution of current guidelines regarding diagnosis and treatment of headache in children at all levels of society, including among the general population and among various kinds of doctors. These trends also emphasise the value of establishing specialised headache clinics for children worldwide.
The present study comprised a displacement towards the top socioeconomic group compared to the distribution of socioeconomic groups in Denmark. Headache in children has previously been shown to be associated with low socioeconomic status (25). Our results indicate that children with well-educated parents are more likely to end up in a tertiary setting like CHC, even though equal access is theoretically available to all since health care services are provided free of charge in Denmark. A greater level of awareness and information in society may help to counteract this.
Having a clear picture of how much parents are aware of how their child perceives his or her own QoL is also of interest. In a cohort of 686 children and adolescents suffering from migraine, Powers et al. found that the score for child-reported PedsQL™ (mean 72.7 (SD 14.8)) and the parent proxy-reported score (mean 72.8 (SD 14.7)) were almost identical (26). This was also the finding in this study. This is positive because a close relationship between child and parent is a good starting point for compliance and successful outcome.
Our patients differed from those in the outcome study carried out by Kabbouche et al. at the headache centre at Cincinnati Children’s Hospital, Ohio, USA, which included only children with migraine (15). Kabbouche et al. evaluated independent subgroups after one, two and five years of treatment and concluded that the MTP was effective with improvement in multiple outcome variables. Claar et al. (Boston, Mass., USA) evaluated 47 adolescents with CTTH after six months of multidisciplinary treatment and found significant improvement in school functioning, frequency and duration (17). The children in our study were followed prospectively as a cohort and represented a broad range of primary and secondary headache disorders, which means that the studies are not directly comparable.
The major limitation of this study is the lack of a control group. The effectiveness of treatment could be accounted for by placebo and regression to the mean. The children might have improved even without our treatment programme as patients are often referred at a point where their symptoms are peaking. The children included in the present study, however, had a wait of four to eight months from referral to first consultation and had suffered from headache for years. As a result, we do not believe that the problem of regression to the mean is relevant in the present study. Furthermore, using overall outcome measures like frequency and QoL does not allow us to make conclusions about the effectiveness of the different parts of the treatment programme. The results of pharmacological treatment are included in our outcome measures, and may be responsible for some of the improvement seen.
The present study had a prospective design and therefore had some drop-outs caused by failure to appear or because the child experienced sufficient improvement. We have taken this problem into account by using a repeated-measure analysis for both types of outcome. However, the missing values might have been even more extreme than the predicted model (had they been observed), since we can only predict from the observations actually observed. The small sample size only justifies preliminary conclusions and unfortunately resulted in a failure to evaluate the importance of possible predictors for a good outcome.
The primary role of a multidisciplinary children’s headache clinic is to treat referred children, but other very important tasks include conducting research and educating physicians and society about headache in children and adolescents, the benefits of knowledge-sharing likely leading to an improvement in the treatment of all kinds of childhood headache. We are convinced that the future will bring more tertiary headache clinics for children. Initiatives have been taken, for example, to establish a network of headache specialists for children, most recently at the 2012 European Headache and Migraine Trust International Congress in London.
Conclusion
The present study describes the MTP in a tertiary children’s headache clinic. We found a significant and clinically important improvement in headache frequency and QoL during treatment. Though preliminary, the results show a good outcome that justifies the need for multidisciplinary treatment programmes to help children who are disabled by or suffer from frequent or chronic headache.
Footnotes
Acknowledgements
We would like to thank the participating children and parents.
Funding
This work was supported by The Lundbeck Foundation (grant number R19-A2040, R34-A3618); the Dagmar Marshalls Foundation; the Tømrermester Jørgen Holm and wife Elisa F. Hansen’s Memorial Trust; the Capital Region of Denmark (grant number R120-A3256); the Danish Headache Society; and the Professor Torben Iversen Travel Fund for Young Paediatricians.
Conflict of interest
None declared.
Clinical implications
The study describes the setting, concept and outcome of a multidisciplinary treatment programme in a tertiary paediatric headache clinic.
The multidisciplinary treatment programme significantly improved headache frequency and quality of life in the included children after six and 12 months of treatment.
We found that 50% of the children had an improvement in headache frequency above 50% at six months.
Though preliminary, the results justify the need for multidisciplinary treatment programmes to help children who are disabled by or suffer from frequent or chronic headache.
The primary role of a multidisciplinary children’s headache clinic is to treat referred children, but other very important tasks include conducting research and educating physicians and society about headache in children and adolescents.