
Abstract
Knowledge on the quality of life of children with headache is lacking. Until now only a few studies in this field have provided information on a limited number of life domains. The aim of this study was to assess the quality of life in a comprehensive number of life domains in children with primary headache presenting at an out-patient paediatric department in a general hospital. From October 2003 to October 2005 all children referred to the out-patient paediatric department of the Vlietland Hospital because of primary headache were investigated by protocol. A thorough history was taken and a general physical and neurological examination was performed. The International Headache Society criteria were used for classification. Quality of life (QoL) was measured using the Dutch version of the Child Health Questionnaire (CHQ-PF50 Dutch edition) and compared with data from a previously investigated cohort of healthy children from the same region, and with data from a cohort of children from the USA with asthma or with attention deficit hyperactivity disorder (ADHD), investigated with the CHQ-PF50. A total of 70 primary headache patients were included in the study (25 with tension-type headache, 36 with migraine, seven with chronic tension-type headache, two with both tension-type headache and migraine). Their mean age was 10.6 years (range 4–17 years); 37 children were male. On all but one subscale (self-esteem) the QoL of the children with primary headache was decreased compared with the cohort of healthy children, especially on the domains of mental health, parental impact time and family cohesion. Compared with the cohort of children with asthma the QoL was significantly worse for our headache group on seven subscales and significantly better on one subscale (general health perception). Compared with the cohort of children with ADHD, the QoL was significantly worse on six subscales but significantly better on three subscales. There were no significant differences on any QoL subscale between children with tension-type headache and children with migraine. We conclude that the QoL in children with primary headache presenting at the out-patient paediatric department of a general hospital seems to be considerably diminished. Furthermore, we conclude that, in this population there is no difference in QoL between children with tension-type headache and those with migraine.
Introduction
Headache is a common problem, not only in adults but also in adolescents and even in children. The prevalence of headache and migraine in children is age and gender dependent. Sillanpää has reported a prevalence of headache of 50.5% for boys and 49.5% for girls at 7 years of age, and a prevalence of migraine of 2.9 and 2.5%, respectively (1). At age 14 years, the prevalence of headache is 48.6 and 51.4%, and for migraine the prevalence is 6.4 and 14.8% for boys and girls, respectively (1).
In the Netherlands 15% of children aged 6–16 years suffer from at least two episodes of headache each month (2); only 30% of these children are seen by a physician. In most cases the parents give the child a simple analgesic, put the child to bed, or take other measures to give the child some rest. If the child is seen by a physician, it is usually a general practitioner (GP). Children with migraine are more inclined to consult a physician than those with tension-type headache (TTH); this is because children with migraine have more alarming symptoms, and treatment by the parents with the measures mentioned above is often insufficient. A relatively small percentage of children with headache seen by the GP is referred to a specialist, who can be a paediatrician, neurologist or paediatric neurologist. Children with migraine tend to be over-represented in the group of children referred (2).
An important outcome measure for effectiveness of treatment is quality of life (QoL), which reflects the impact of disease and treatment on a subjective evaluation by the patient (or, in the case of children, by the parents) of the patient's physical functioning and emotional well-being (3–6). QoL studies in children with headache and migraine are either population-based (2, 6, 7) or hospital-based (8–10). In both types of study, but particularly in the hospital-based ones, children with headache had significantly lower QoL scores than healthy children. Compared with children with chronic illness (such as rheumatic disorders or cancer) their QoL was similar with respect to impairments in school and emotional functioning. All the hospital-based studies were conducted in tertiary headache centres (8–10); these studies indicate that children with headache have a comparable QoL to those with a chronic illness.
The present study aimed to measure the QoL in children with primary headache presenting in an out-patient paediatric department in a general (non-academic) hospital to obtain information on the severity of headache as perceived by the children and their family. It is of clinical interest to compare the QoL in children with migraine with that in children with TTH. In addition, we compared the QoL in children with migraine and TTH with that in the normal population. It was hypothesized that children with primary headache would report a lower QoL than healthy children.
In the QoL studies performed in tertiary headache centres, the QoL in children with primary headache was comparable to that in children with chronic illnesses such as cancer or rheumatic disorders (8–10). As attention deficit hyperactivity disorder (ADHD) and asthma are, in our opinion, conditions of similar severity to headache, but not as severe as cancer and rheumatic disorders, we found it of additional clinical interest to compare the QoL in children with primary headache with that in children with one of these two chronic afflictions. Therefore, we decided to compare our data with a cohort of children with asthma and ADHD in the USA who had previously been investigated with the same QoL questionnaire. It was tested whether there is a significant difference in their QoL compared with that of children with primary headache.
Material and methods
Patients
A consecutive series of 70 children referred (between October 2003 and October 2005) because of primary headache complaints by their GP to the out-patient Department of Paediatrics of the Vlietland Hospital participated prospectively in this study after informed consent was obtained. Headache diagnosis and classification were obtained using the criteria of the International Headache Society (IHS) (11).
With regard to the control group, the study population consisted of 353 schoolchildren in grades 3–8 (aged 5–13 years) at three representative elementary schools in Rotterdam, the Netherlands (6). In both the headache and control group we used the original database for statistical analysis. The ADHD cohort consisted of 83 children who were treated at the behavioural neurology clinic at Sargent College, Boston University (MA, USA) (12–15). Finally, the QoL data of the asthma cohort were collected from a baseline pharmaceutical study among 158 children with asthma in the USA (12). In both the ADHD and asthma group we could use only the summarized published data for statistical analysis in this study.
Procedure
In case of the children with primary headache, a thorough history was taken and a complete physical and neurological examination was performed. The Dutch version of the Child Health Questionnaire (CHQ-PF50 Dutch edition) (6) was handed over to the parents or guardians; they were asked to complete it at home and return it at the next visit. For both children and adolescents the parents filled in the questionnaire, which is understandable given the cognitive developmental level of the included children (≤ 11 years old) that does not permit the abstract formal thinking required for answering QoL questions. To obtain uniformity in the way the answers were given, the parents of children > 12 years old were also asked to complete the questionnaires. No rewards or other response-increasing policies were applied. To ensure accuracy, the questionnaire was reviewed at the next visit at the out-patient department. On that occasion, if the forms had not been returned completely filled out or not filled out at all, parents or guardians were asked to complete the form during the visit. All questionnaires were filled out completely without any drop-outs. All parents were able to read and write Dutch. The data were stored on a database. Only children with primary headache as defined by the IHS criteria (11) were included. Children with secondary headache were excluded. There were no other exclusion criteria.
With regard to the control group, the teachers of each class distributed the health questionnaires to the children, to be handed over by them to their parents (or guardians). The children were required to return the forms within 2 weeks. No rewards or other response-increasing policies were applied. The two criteria for eligibility for analysis were: (i) parent's ability to read and write Dutch, and (ii) at ≥ 80% response on the CHQ items (6).
The QoL data of the children with ADHD were gathered using two modes of administration (on site completion and mail out/mail back) at the behavioural neurology clinic where they were treated. A diagnosis of ADHD as defined by the Diagnostic and Statistical Manual of Mental Disorders, 3rd edn revised (DSM-II-R) criteria was the primary eligibility criterion (12–15). The eligibility criteria in the asthma cohort were: (i) suffering from asthma in accordance with the American Thoracic Society definition of asthma, and (ii) using asthma pharmacotherapy daily for ≥ 3 months prior to screening (12).
Measures
We decided to measure QoL with the CHQ because this questionnaire has already been administered in chronically ill children (6, 12, 16). The CHQ was translated into Dutch in 2001 according to international guidelines (6, 16–18). This translated version has previously been validated; the internal consistency [Cronbach α on average 0.72 for the domains (range 0.39–0.96)] appeared to be adequate and the test–retest reliability good (6). This version was further validated by measuring the QoL in 353 healthy Dutch schoolchildren from the same region in which the present study was performed (6); this latter validation study provided the data on the QoL in healthy children.
The CHQ-PF50 comprises 50 items over 11 multi-item scales or domains, and two single-item questions (6, 12, 16). The life domains give insight into not only the QoL of the child itself, but also the impact of the disease of the child on their parents and family (see Table 1 for the separate subscales). Each CHQ domain consists of three to six items with four, five or six possible responses per item. According to the CHQ User's Manual, the domain item scores have to be recoded, recalibrated and finally summed. The final score may range from 0 (worst possible health state) to 100 (best possible health state) (12).
CHQ-PF50: children with primary headache compared with healthy children, and with children with asthma or with ADHD

∗Significant difference (P < 0.05; two-sided) measured by two-way
†Significant difference (P < 0.05; two-sided) measured by one-way
ADHD, attention deficit hyperactivity disorder; QoL, quality of life; NA, not available.
Statistical analysis
Analyses were performed using the statistical programme
Results
Demographics
This study evaluated 70 children (37 male, 33 female). Their ages ranged from 4 to 17 years, the mean age was 10.6 years (
The ADHD cohort consisted of 83 children. Their ages ranged from 6 to 13 years, the mean age was 11 years (
CHQ scores
Children with primary headache compared with healthy children
Table 1 presents the means and
Children with primary headache compared with children with chronic illness
Table 2 presents the means and
CHQ-PF50: children with migraine compared with TTH
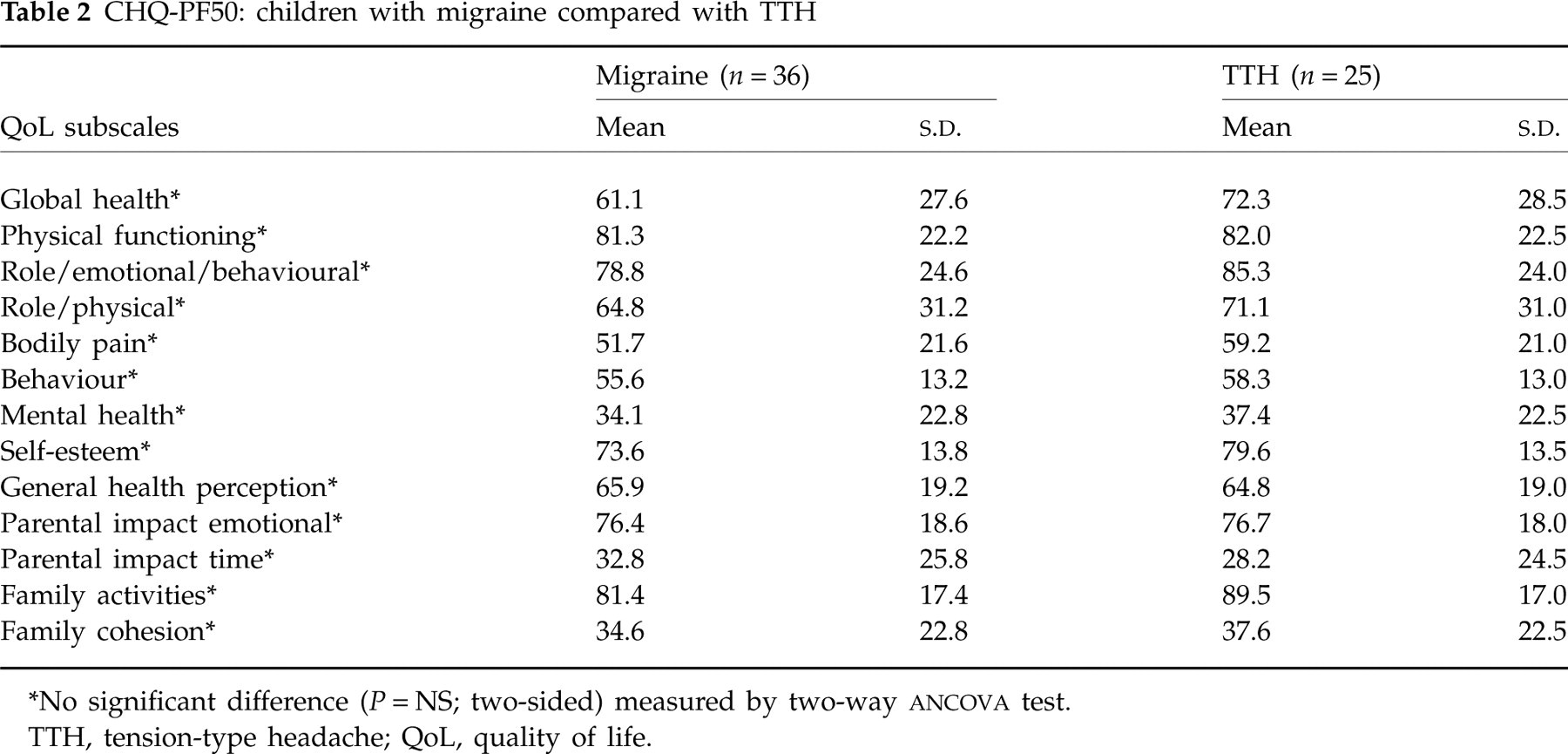
∗No significant difference (P = NS; two-sided) measured by two-way
TTH, tension-type headache; QoL, quality of life.
Children with migraine compared with children with tension-type headache
Table 2 presents the means and
Discussion
The QoL in our group of children with primary headache was significantly decreased on 12 of the 13 life domains of the CHQ compared with a group of healthy children from the same region after adjustment for gender and age. This is in agreement with our hypothesis and the studies of Powers and Nodari, in which children with primary headache reported a lower QoL on all subscales compared with a cohort of healthy children (8–10). No data were available regarding the presence of headache among the control group of children. Nevertheless, as the exclusion of these patients would have rendered the differences in QoL between our patient and control group even larger than found, this would not have influenced our conclusions.
QoL research in children is a rapidly expanding area, and reports on the impact of various chronic diseases on paediatric and adolescent QoL are beginning to appear (9). We measured QoL with a validated Dutch version of the CHQ (6). The CHQ is not disease specific; it provides information on a broad range of 13 life domains, whereas other clinical studies have examined only six or nine domains (6, 8–10, 12, 16). The CHQ also gives insight into the burden placed on the family and parents of the child with primary headache, which is missing in the QoL measurement tools in other clinical studies such as the Pediatric Quality of Life Inventory (PedsQL) (8, 9) and the Quality of Life in Youth Questionnaire (QLH-Y) (10). From this study, the conclusion seems justified that a child with primary headache, severe enough to consult a specialist, places a heavy burden on its parents and brothers and sisters.
The data from this study allow us to conclude that the QoL of children with headache is very poor, with particular impact on the domains of mental health, parental impact time and family cohesion. The question arises whether this is the consequence of the headache of the child itself, or whether the headache is a consequence of the poor QoL. To address this question, longitudinal headache studies in children are needed, with headache frequency and intensity as a primary outcome measure and QoL as a secondary outcome measure, to evaluate how both outcome measures influence each other.
In contrast to most of the above-mentioned clinical studies, we measured QoL in children with TTH as well as with migraine (8–10). Only Nodari et al. (10) have measured QoL with TTH and migraine in a tertiary headache centre using the QLH-Y. This latter questionnaire was originally developed by Langeveld et al. (7) and was translated and validated for the Italian population; because there was no analysis tailored to the children with TTH and migraine, it was not possible to detect differences in QoL between them. In the present study we included 26 children with TTH and 36 with migraine; no significant differences in QoL were found between them on any subscale after adjustment for gender and age. The average difference on the 13 variables in terms of Cohen's d between migraine and TTH patients was 0.15. In order to detect a difference of this size at a nominal level of significance α= 0.05 (two-sided) and β= 0.20, the sample size required is 845 patients in both migraine and TTH patients. Assuming that the 13 variables can be adequately represented in two dimensions, the actual level of significance was α= 0.025 (two-sided). Therefore, conclusions about the absence of differences in QoL between children with migraine and TTH have to be drawn with caution because of the low number of children in both groups and, consequently, the low power of this comparison. Nevertheless, we speculate that the absence of differences might be due to the system of healthcare in the Netherlands, in which the GP is the key person in referring the child to an out-patient paediatric department. We believe that the most important factor in referral is this physician's perception of the burden placed on the child and its family as induced by the headache. Thus, it is not so much the type of headache that is the reason for referral, but rather the severity of the headache and its impact on the QoL of the child and its family.
We compared the QoL in children with primary headache with that of children in the USA with asthma or with ADHD. Due to absence of data on the subscale of global health and family cohesion, comparison on these domains was not possible for children with asthma or with ADHD. Furthermore, because there were no data on the subscale of family activities in the children with asthma, a comparison on this domain was also not possible.
In seven subscales (i.e. role/emotional/behavioural, role/physical, bodily pain, behaviour, mental health, self-esteem and parental impact time) the QoL of the children with primary headache was significantly lower than that of children with asthma; on the subscales physical functioning and parental impact emotional no significant differences were found. On the subscale of general health perception, QoL was significantly higher in children with primary headache. Therefore, we conclude that QoL of children with primary headache is in general lower than in children with asthma.
The QoL of children with ADHD was on six subscales (i.e. physical functioning, role/physical, bodily pain, mental health, general health perception and parental impact time) significantly higher than in children with primary headache. The QoL of the subscales role/emotional/behavioural, self-esteem, parental impact emotional and family activities was significantly higher in children with primary headache than in children with ADHD. There was no significant difference on the subscale behaviour between the groups. We conclude that QoL in children with primary headache is in general worse than in children with ADHD, but is better with regard to impact on the family. Because of the different origins and cultural background of the children, and possible differences in the meaning of the items due to the different languages, any conclusions about the differences in QoL between children's primary headache on the one hand and asthma and ADHD on the other have to be drawn with caution. Also, the different clinical setting and the time elapsed since the study on QoL of children with asthma was performed (in 1994) may be of relevance. Furthermore, adjustment for differences in the demographic character of the samples was not possible because we did not have the original databases at our disposal. We have compared the QoL data of the boys in the headache group with the QoL data of the ADHD and asthma sample, as both samples contained a relatively high percentage of boys (81% vs. 69%). We found no marked differences in comparison with the QoL data of the whole headache group. Therefore, we cautiously conclude that adjustment for gender in the ADHD and, to a lesser extent, in the asthma sample will not substantially influence the original (
To gain more insight into the impact of different types of headache, a QoL study using the same questionnaire should be performed in children with ADHD, asthma and headache from the same out-patient department.
Finally, we believe that QoL is an important concept, to gain insight not only into the effect that a disease has on the emotional and physical well-being of a child and the impact on its family, but also into the dynamic aspects of the disease or the response to treatment. There is a lack of longitudinal studies with QoL as outcome measure in the field of primary headache in children. More longitudinal studies with QoL as outcome measure are needed to gain more insight into the dynamic aspects of primary headache in children and especially on the relation between headache and QoL. With respect to treatment, every treatment or intervention has in general not only expected beneficial effects, but also adverse effects. Most intervention studies in this field (primary headache in children) usually describe the adverse effects as mild and safe. However, the simple description of the kind and number of adverse effects gives insufficient insight into the severity and appreciation by the child (19), combined with the beneficial effects of the intervention. QoL in these studies, measured on a broad range of life domains, combined with such primary outcome measures as headache frequency and intensity, can provide this insight. Therefore, we recommend that more QoL studies in this field should be performed, not only descriptive but also dynamic assessments, in which QoL is used as an outcome measure in intervention and longitudinal studies.
Conclusions
Headache is a common problem in childhood. The present study has shown that in children with primary headache referred to a paediatric out-patient department of a Dutch general hospital, the QoL is considerably lower than the QoL of healthy controls. Also, we conclude from this study that a child with primary headache places a considerable burden on its parents and family. Within the group of children with primary headache, the QoL of children with TTH is similar to that in children with migraine. There are indications that primary headache in children affects QoL in a broader spectrum of life domains and to a larger degree than does asthma or ADHD.
Footnotes
Acknowledgements
The authors thank all the children and their parents who participated in this study. Special thanks go to the paediatricians in the Vlietland Ziekenhuis for their support and referral of the patients: Coby Langendoen, MD, Lia van Wijk, MD, Bert den Exter, MD, Arjan Pijning, MD, Esther Hentzen, MD, Brigitte de Bie, MD and Evelyne van Boeckel, MD.