
Abstract
Headache is the most frequent neurological symptom and commonest manifestation of pain in childhood. Measuring the impact of headache in terms of health status, functioning and quality of life can inform the prioritization of competing resource claims, screen for unmet need, improve communication between patient and physician and monitor response to treatment. We undertook a critical review of the literature measuring the impact of headache in children and identified 33 papers that contained relevant information. Findings reflected a wide range of settings, age groups, methodologies and outcome measures. Considerable methodological limitations affected all studies, including inadequate description of study design, methodology and data analysis. Nevertheless, although we found the existing literature to be of inconsistent quality, the impact of headache in children and adolescents is substantial. Rigorous studies are required to quantify this burden using measures that are valid and reliable and whose development has been informed by both theoretical and practical perspectives.
Keywords
Introduction
Headache is the most frequent neurological symptom and commonest manifestation of pain in childhood (1). Estimates of the prevalence of headache in children (age 8–12 years) and adolescents (13–17 years) vary widely depending on setting and on the methodology and diagnostic criteria applied. Studies have reported annual prevalence rates in children of between 3 and 11% for migraine (2–4) and between 0.9 and 24% for tension-type headache (4, 5). The prevalence of ‘self-reported’ headache is higher. Between 20 and 30% report headaches at least weekly and 6% have headaches several times a week or daily (6–10).
Information on the impact of a disease can inform the prioritization of competing resource claims, screening for unmet need, improving communication between patient and physician, monitoring response to treatment, and supporting clinical audit. The impact of paediatric disease consists of three elements (11):
Health status. This concerns a child's biological and physiological dysfunction in terms of symptoms and illness control (12). For headache, frequency and intensity of pain is the most obvious symptom. However, other painful conditions, including neck, abdominal and back pain, are also more common (13), as are sleep disorders (14, 15).
Functional status. Functional status captures the child's ability to perform activities that are essential to meet basic needs, fulfil roles and maintain well-being. School attendance is the most common and accurately measured index of this domain.
Quality of life. The recognition that personal burden of illness cannot be fully described by clinical and functional measures alone has led to the development of measures of health-related quality of life. A review of quality of life instruments in children has identified the diversity of conceptualization and lack of empirical evidence for many of the fundamental assumptions in instrument design and application (11).
There is an emerging consensus that for chronic health conditions both generic (designed to be applicable to all population subgroups and useful for comparing outcomes between them) and disease-specific (designed to be applicable to one group and useful in detecting changes in the condition) health-related quality of life measures should be administered. This consensus also applies to paediatric practice (16).
The aim of this paper is to review the extent, findings and quality of the literature reporting the impact of headache in children and adolescents on functional status and quality of life.
Methods
The science citation index and social sciences citation of the Web of Science was searched for entries from 1914 to December 2006. The terms used were (quality of life OR health OR functioning) AND (headache OR migraine) AND (paediatrics OR children OR adolescents).
Although formal guidelines for assessing the quality of randomized controlled trials and accepting them into a review are recognized, similar methods do not exist for descriptive studies. We therefore undertook a critical review of pertinent studies and not a systematic review with defined quality criteria.
Two hundred and thirty-nine papers were identified, of which 13 contained relevant information. Relevant references and citations from each paper were searched. Citations of authors active in the field were reviewed and relevant journals ‘hand searched’. Papers reporting the epidemiology of headache and chronic pain in children were reviewed for relevant references to quality of life. These searches identified a further 20 papers.
Reports were included only when they reported on impact on function or quality of life. Papers reporting psychological, personality or behavioural characteristics were excluded due to the uncertain direction of causality.
Results
Thirty-three papers were identified that contained relevant information.
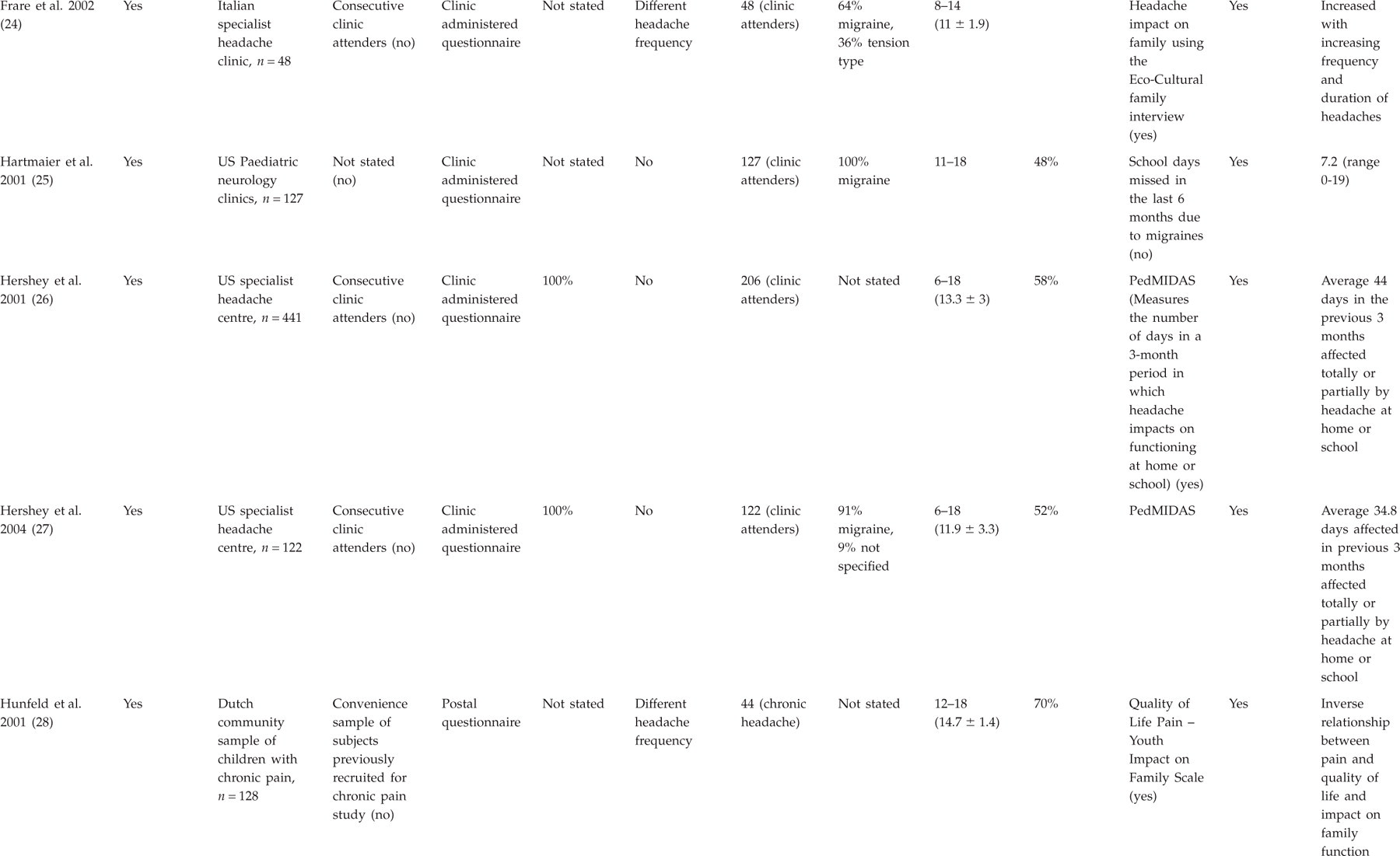
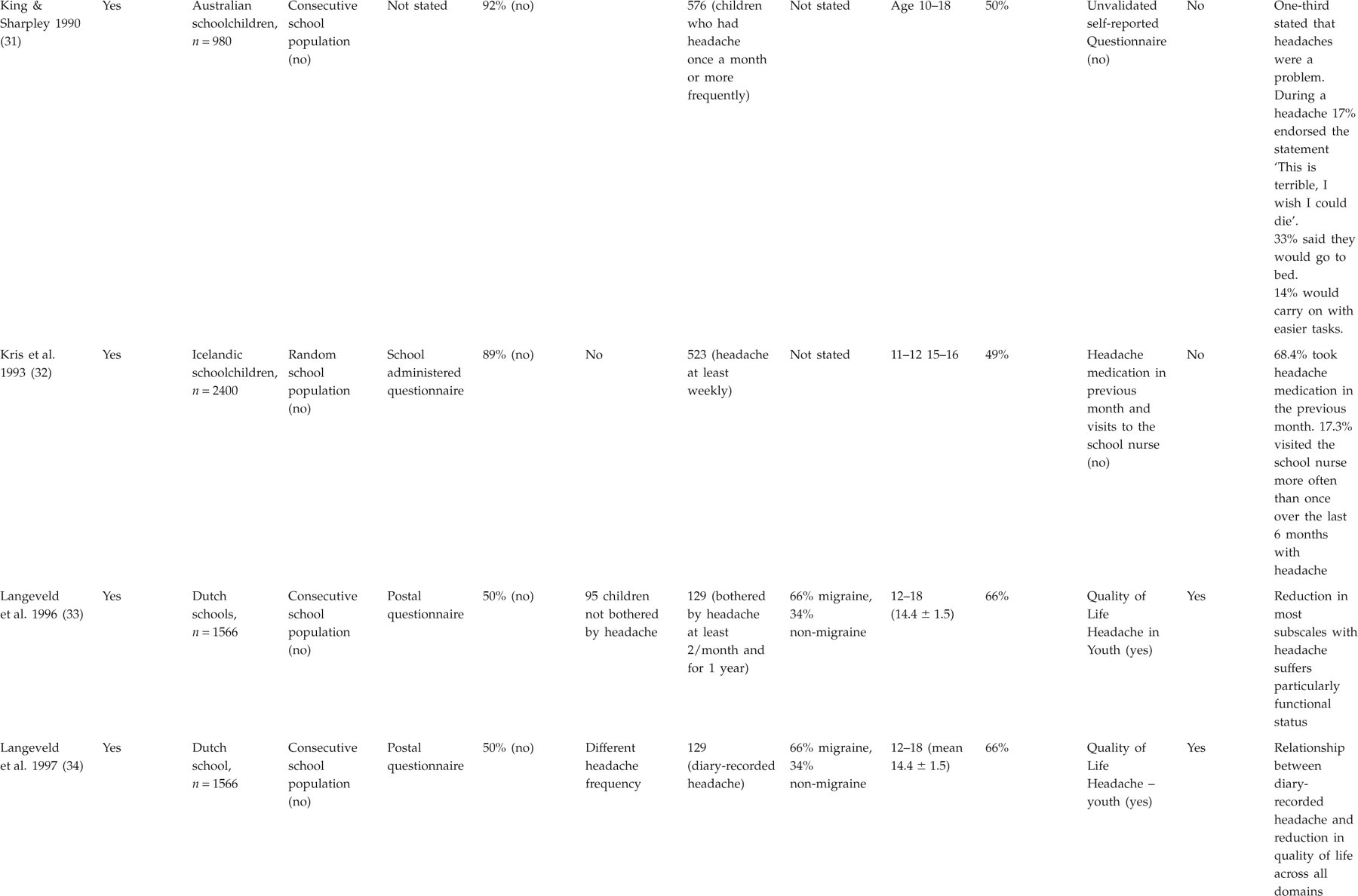
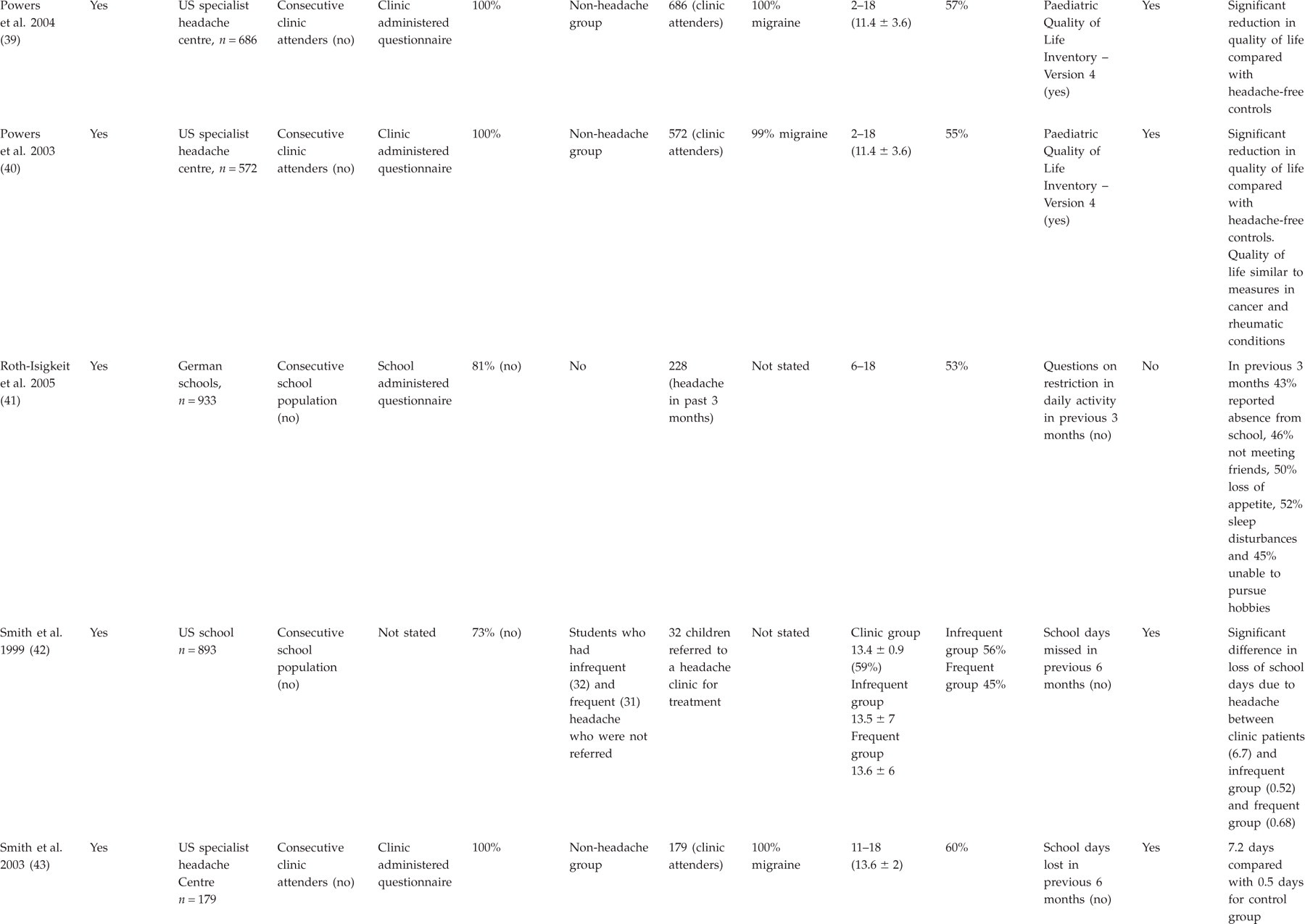
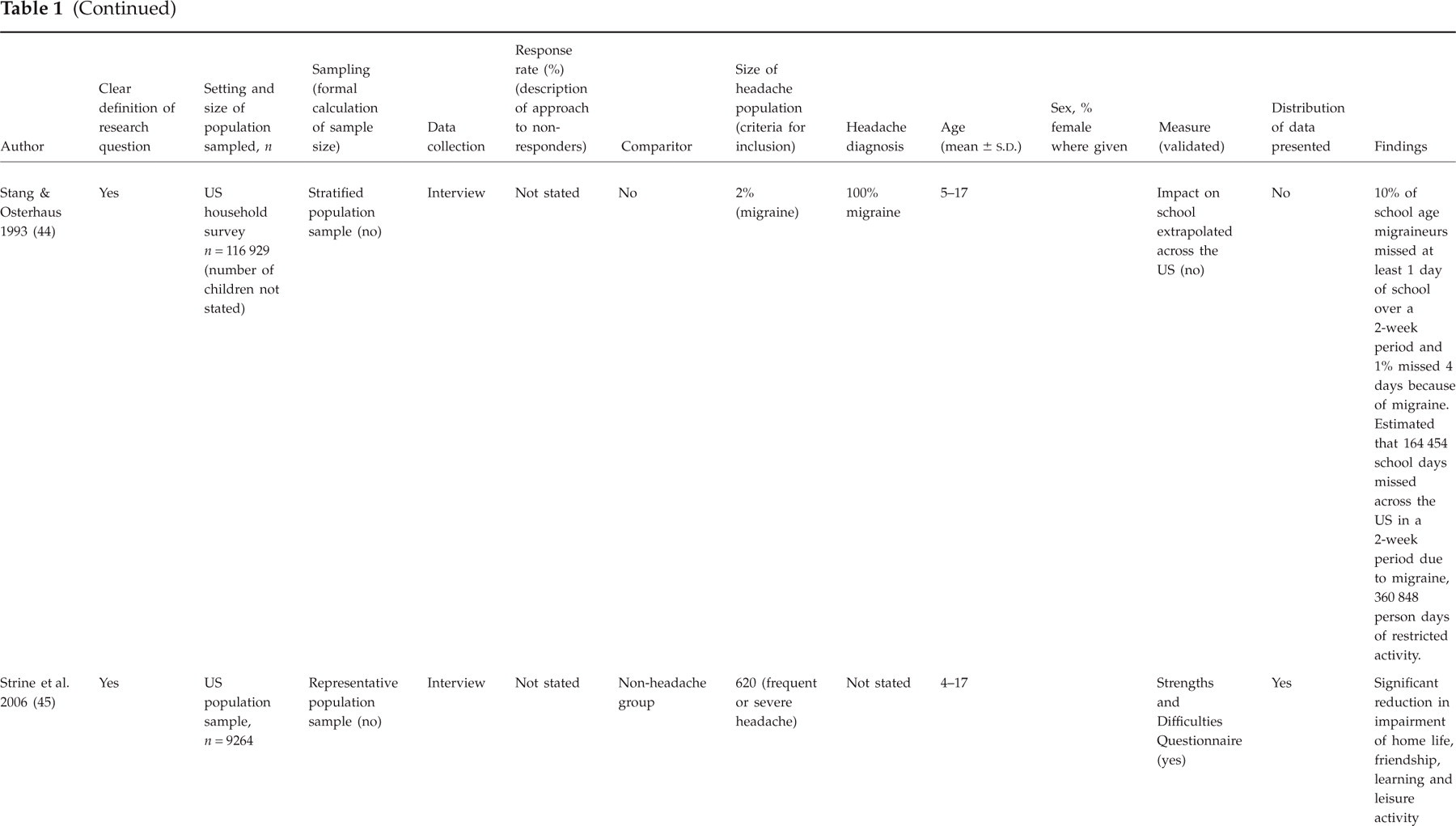
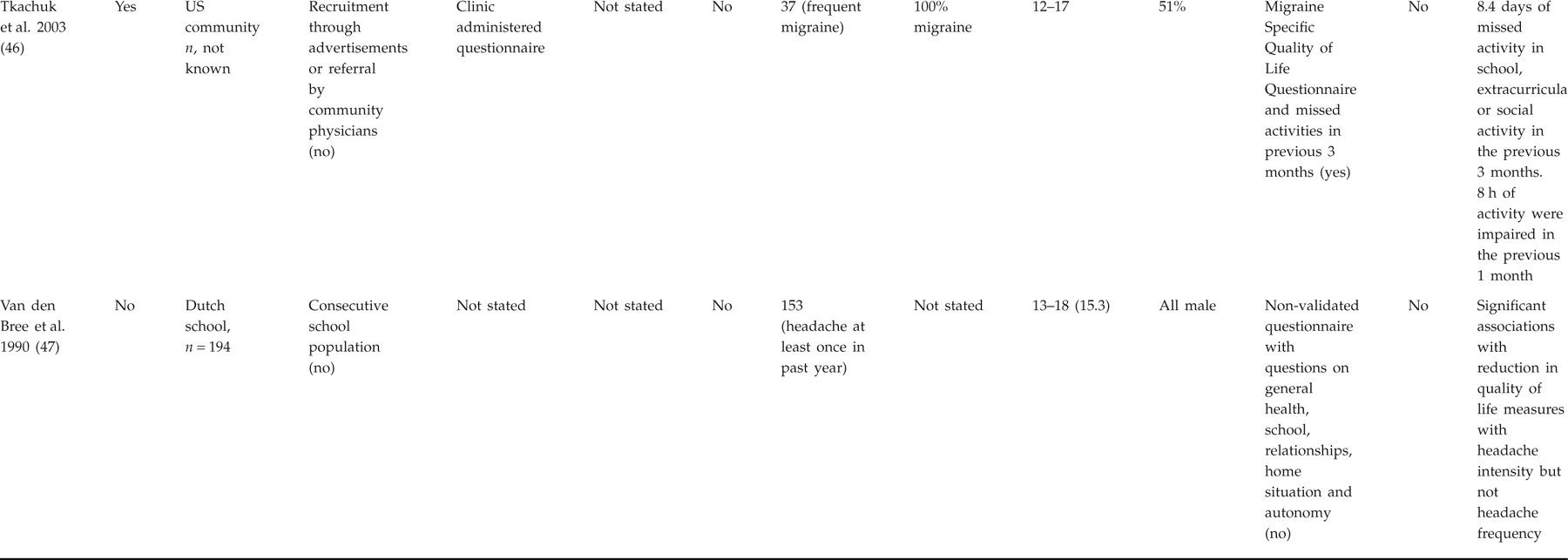
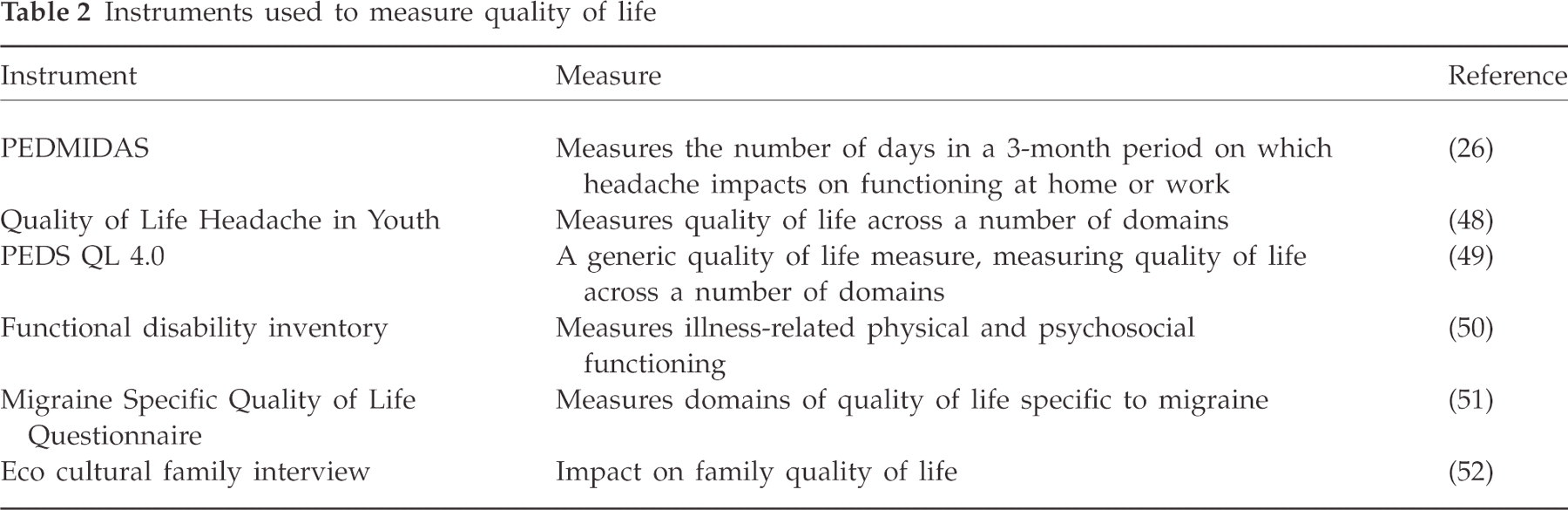
Findings reflect a wide range of settings, age groups, methodologies and outcome measures (see Table 1). The validated quality of life instruments used are shown in Table 2.
Literature review




Instruments used to measure quality of life
Although all papers clearly defined a research question, none provided statistical estimates of sample size requirements. There were a variety of sampling approaches, but five (15%) did not specify the sampling method. In general, the description of the methodology was poor. For example, where non-responders were identified, the approach to follow-up was not described.
Seventeen studies (52%) compared results with a control group, but the characteristics of the comparators were never described. Fourteen (42%) papers offered headache diagnostic categories, but diagnostic criteria were not stated or the diagnostic difficulties in this age group acknowledged.
Two studies (35, 38) used qualitative approaches, reporting feelings of insecurity, difficulties with lessons, anger and frustration that were attributed to headache. Both studies lacked the methodological rigour normally required for qualitative research.
The most common quantitative measure reported was impact on schooling. In total, eight studies reported an average of 8.3 (standard deviation 4.3) days' school loss extrapolated to a 1-year period due to headache. Three studies obtained from children attending specialist headache care centres (17, 26, 27) suggested that in a 3-month period, an average of 32 days were totally or partially affected by headache. Only three studies that reported school impact were representative of the general school population (4, 21, 42). In these, headache prevalence was 11, 3.8 and 9% with annual school loss of 2.8, 4 and 13.4 days, respectively.
Two studies reported school sick bay attendances with headache. These attendances may reflect an impact of performance at school. A UK study of 1451 children age 5–19 years found that 5% of this population reported in a 3-month period (21). An Icelandic study of 2400 school children age 11–16 years found that 4% of this population reported one or more times over a 6-month period (32).
Nineteen studies used questionnaires that sought to measure quality of life. Of these, 10 were headache specific, seven generic and two non-validated. Six studies found quality of life to be inversely related to headache frequency or severity (19, 23, 24, 28, 33, 34). Six studies used quality of life instruments and identified a significant reduction amongst headache sufferers compared with non-headache controls (20, 33, 37, 39, 40, 45). However, the characteristics of all control groups were not described, so it was difficult to ascertain the validity of the comparisons. One study (40) identified that quality of life in children attending a specialist headache centre was comparable to that of children attending special cancer or rheumatology clinics.
Discussion
What did we find?
This review has identified 33 studies reporting on the impact of headache on the functional status and quality of life of children. Considerable methodological limitations affected all studies, including inadequate description of study design, methodology and data analysis. There was an absence of design for adequate power for meaningful comparison between groups. Although a number of studies reported headache type, the difficulties of diagnosis in this age group were not acknowledged and diagnostic criteria not stated.
Half of the studies used a control group, but the characteristics of the comparators were never defined. Inferences from these findings should therefore be treated with caution.
Studies that used headache-related quality of life measures were limited by the lack of published validation studies to support them.
Despite these limitations, we identified a substantial headache-related morbidity for a significant number of children, most notably in days lost and affected at school. On average, studies reflecting school settings found that 8% of children lost 6 days/year of school. Headache impact was directly related to headache frequency and severity.
What were the weaknesses in our review?
Methods to synthesize research evidence are available to ensure consistency of reporting, but these focus on randomized controlled trials (53). The issues encountered in synthesizing descriptive and non-experimental evidence have not been formally explored, although the problems are recognized (54). Due to the wide range of methodological approaches and outcomes used, we were unable to synthesize the studies we reviewed into a coherent analytical framework.
We applied no quality criteria to our selection of studies as relevant guidelines for this exercise do not exist. Although formality and explicitness are desirable, inevitably they have to be allied constantly to judgement in reviews such as this. For example, when considering the impact of headache, the direction of causality may be uncertain as the interplay between headache, contextual factors, coping ability and impact remains poorly understood (55). The combination of headache and certain personality features may be the expression of a shared genotype; headache may be the result of a stressful environment, which itself may impact on quality of life and coping mechanisms; or the impact of headache may be a general feature of chronic pain and not specific to the disease itself. For this reason we only selected papers that described headache impact on function or quality of life, while recognizing that even then, the direction of causality may be reversed.
Setting the review into the context of existing literature
We are unaware of any previous reviews of the impact of headache in children. However, there is extensive literature on the impact of headache, and in particular migraine, in adults. In this population a number of barriers to care are recognized. Many sufferers do not consult their doctors, patients may not receive the correct diagnosis and even when a correct diagnosis is made, effective treatment may not be given (56).
These barriers are likely to be more prominent in the paediatric population, who are less able to articulate their problems and seek attention. Headache amongst children has a high risk of development into a chronic condition and persisting into adulthood (57). Children with headache also have a risk of developing other physical and psychiatric morbidity in adulthood (58). As simple, inexpensive, evidence-based approaches to paediatric headache treatment are available for the majority of headaches (59), it is important to identify and treat unmet community need, particularly where the burden is large. As with adults, impact, particularly in terms of health-related quality of life, is an important marker of this burden and the identification of patients needing particular attention (60).
Recommendations for further research
Information on the impact of disease is essential if politicians, consumers, commissioners and providers are to make decisions aimed at providing cost-effective, high-quality care.
From a theoretical perspective, the difficulties of inferring findings from adult quality of life research to a heterogeneous childhood population are recognized. Here there are different cognitive, self-regulation and psycho-social issues that arise at various stages of development, while the conceptualization of pain and its severity change across different cultures and with time (61). Parent proxy reports of impact can also be affected by the domain investigated, the age of the child and the parent's own quality of life (62). For example, clinical features of headache can be different from those experienced by adults, and children may be less well able to verbalize their concerns. Although health, functional status, quality of life and health-related quality of life are related, they are not interchangeable. There is a need for the development of validated and reliable instruments to access these domains in children both generic and headache specific.
More specifically, rigorous studies are needed on the impact of headache compared with non-headache controls in well-defined samples that use relevant and valid measures and that are adequately powered. The policy context of the study should be clearly identified and an instrument chosen that is relevant to this context, recognizing that impact consists of elements of health, function and quality of life.
In conclusion, despite theoretical limitations and studies of inconsistent quality, this review has found that the impact of headache in children and adolescents is substantial. More rigorous and representative studies are required to quantify this burden with the aim of identifying and addressing unmet need in this population.