
Abstract
Despite the high prevalence of headaches, multidisciplinary headache clinics are few and their efficacy still needs validation. We set out to describe the procedures, characterize the patients and evaluate the treatment results in Danish Headache Centre. All clinical records for patients discharged in 2002 were systematically reviewed. Diagnoses were classified in accordance with ICHD-II. Outcome results were analysed with respect to headache diagnoses, frequency, intensity, absence from work and medication use. Five hundred and five patients were included and 336 were eligible for the study. Mean age was 46 years and male/female ratio 1 : 2.4. For patients without medication overuse headache (MOH) a reduction in headache frequency (P < 0.01) and intensity (P < 0.05) was seen for frequent episodic and chronic tension-type headache (TTH), migraine, cluster and other headaches. No reduction was seen in post-traumatic headache. Absence from work decreased significantly for migraine (P < 0.001) and frequent episodic TTH (P < 0.05). For patients with MOH a reduction in headache frequency was seen for TTH and migraine (P < 0.001). A specialized headache centre is valuable in treatment of patients with complex headache disorders.
Introduction
Multidisciplinary pain treatment is now an established discipline and there are hundreds of such clinics throughout the world. Recently, a controlled trial has documented the value of this approach in pain treatment (1). Usually these clinics do not treat severely affected headache patients, who are cared for by neurologists. Multidisciplinary headache clinics or tertiary specialized headache clinics are not common and very few are based in an academic neurological department. This contrasts with a huge need, because headache disorders are so common (2) and cause so much disability (3). We have been unable to find studies that describe procedures and results in multidisciplinary academic headache clinics.
Against this background and because a controlled study to document the effect of multidisciplinary treatment is extremely resource and time demanding, we thought it useful to publish methods and results from the Danish Headache Centre (DHC), even if uncontrolled. To ensure the quality of our data, we have used standardized methods for the initial evaluation of our patients and for follow-up and discharge. For diagnostic purposes we have used The International Classification of Headache Disorders, 2nd edn (ICHD-II) (4). Realizing the shortcomings of such a study, we aim to describe the procedures of the centre, the classification of our patient material and the preliminary treatment results.
Organization
The DHC was inaugurated in 2001 as a tertiary out-patient referral headache centre, organized in the Department of Neurology, Glostrup University Hospital. The main uptake area is Copenhagen County with a population of 600 000. In addition, DHC also functions as the only national referral centre for severely affected headache patients in Denmark (5 million inhabitants).
The capacity was initially 700 new patients per year, but during 2002 the intake was increased to 1000 patients per year. Patients are either referred from general practice (GP), from practising neurologists or from other neurological departments. All levels of treatment are publicly financed in Denmark and free of cost for the patients.
The staff consists of four part-time senior headache specialists supplemented by junior doctors on rotation, two physical therapists, two psychologists, three nurses and 3.5 secretaries.
Treatment strategies
Before their first visit all patients receive a diagnostic headache diary and are told to record prospectively headache characteristics, including type and amount of medication used, for a 4-week period (5). They also fill out a questionnaire regarding status of health, work and prior headache treatment. This detailed standardized information is supplemented with a medical interview and a physical and neurological examination at the first visit. The medical treatment is then optimized at repeated visits with a specialist and, depending on need, referral is made to physical therapist, psychologist or nurses. At discharge patients are returned to their GP with detailed instructions for further treatment strategies.
The physical therapists see patients suffering from tension-type headache (TTH) or combined headaches with significant pericranial muscle tenderness. The sessions are individual. They consist of active exercises and detailed information about identification and avoidance of possible muscular stress factors. Passive treatment strategies such as massage or ultrasound are avoided.
The psychologists primarily use group sessions (eight patients) and focus on stress management (cognitive and behavioural techniques) and biofeedback relaxation. Referral to a psychologist is initiated if comorbid psychiatric disorder is suspected, if pharmacological treatment is insufficient or if the patient expresses specific interest in psychological treatment.
The nurses’ main responsibilities are as coordinators of the multidisciplinary treatment of patients with medication overuse headache (MOH). Patients who fulfil the diagnostic criteria for probable MOH (pMOH) (4) are referred to the so-called headache school. All acute headache medication is discontinued abruptly and patients are kept medication free for 2 months. The programme consists of six group sessions within a 3-month period. The first session takes place 3 weeks before withdrawal. The second session is followed by abrupt discontinuation of all acute headache medication. The last four sessions takes place at 2-week intervals after withdrawal. During these sessions the patients are informed about the mechanisms underlying pMOH, psychological influences on pain perception and instructed by the physical therapists in active exercises. In general, the patients are absent from work for 2 weeks during withdrawal, usually the first 2 weeks. Levomepromazine is allowed as the only rescue medication during withdrawal, primarily to be used for the first 1–2 weeks. Two months after withdrawal, headache diagnoses are revised and prophylactic treatment is initiated if needed. At this time a modest amount of symptomatic medication is allowed, but with a strict upper limit agreed by the patient. In-patients follow a highly structured 2-week programme, and thereafter a similar out-patient programme for the following 6 weeks.
Materials and methods
All clinical records for patients discharged from DHC in 2002 underwent retrospective audit, and data were loaded in a Microsoft Access 2002 database. The patients were primarily diagnosed according to ICHD-I, but data allowed a subsequent reclassification according to ICHD-II.
For each patient the following items were available: the medical record, a diagnostic diary, a questionnaire recorded by the patient before the first visit concerning status of health, work and prior headache treatment, and a questionnaire recorded by the doctor at the final visit describing headache diagnoses, frequency, medication use and missed workdays. Finally, an evaluation questionnaire was recorded by the patient at the final visit regarding their satisfaction with the level of information and their scoring of the treatment results.
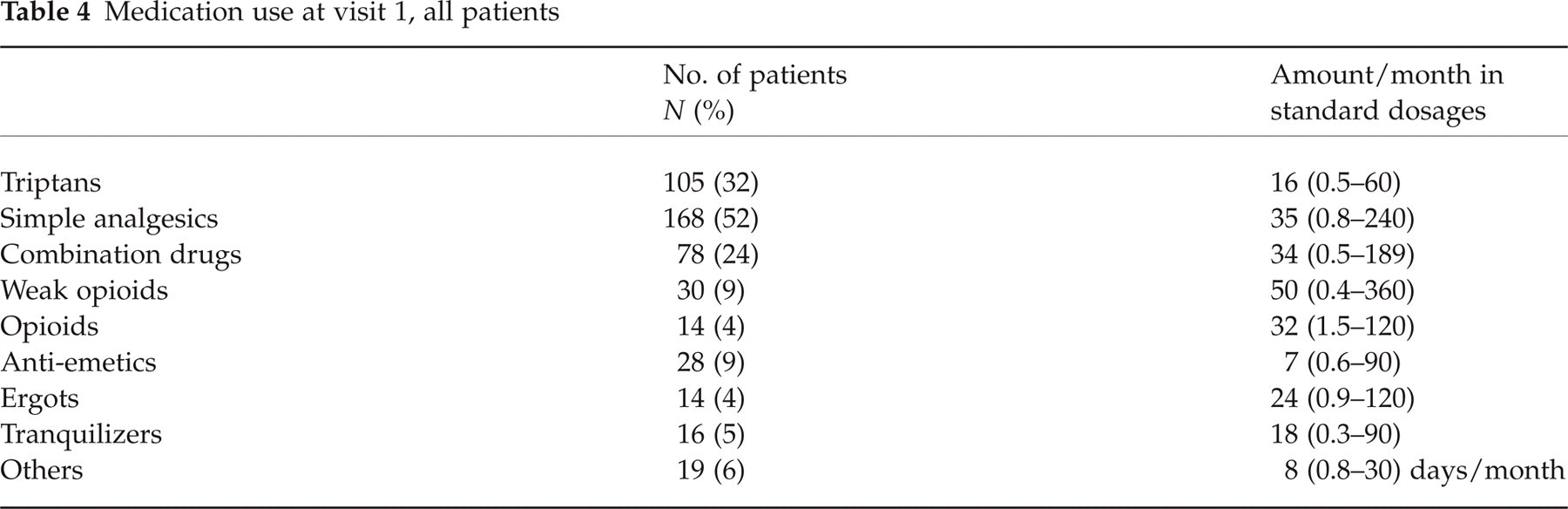
All diaries were examined and International Headache Society diagnoses, headache frequency, intensity and medication consumption prior to the first visit established the baseline values. Medications used were transformed to standard dosages (SD) and sorted into nine groups. Examples of SD in the different groups could be 50 mg sumatriptan, 1 g acetaminophen, 500 mg acetaminophen in combination with 30 mg codeine, 50 mg codeine, 10 mg morphine, 20 mg metoclopramide, 1 mg ergotamine, 5 mg diazepam. Drugs that could not be sorted in one of the first eight groups were placed in others and registered as days/month of drug use. In MOH, headache frequency, intensity and diagnoses after withdrawal were also established. A 50% reduction in either frequency or intensity after withdrawal was defined as cut-off for diagnosing MOH. A final diagnosis of pMOH was given if the patients did not complete withdrawal from the overused medication or if the necessary information about frequency/intensity was incomplete.
Thus, the diagnosis of MOH is based on headache frequency/intensity after withdrawal, but the presented results are comparisons between baseline and discharge values.
Statistics
Statistical analysis was performed with SPSS version 12.0 (SPSS Denmark A/S, Holte, Denmark), and the Wilcoxon signed rank test was used for paired comparisons. P < 0.05 (two-tailed) was chosen as the level of significance.
Results
Five hundred and five patients were discharged from DHC in 2002. One patient was referred twice, making 506 courses of events. Of these, 14 had other diagnoses than headache and for seven patients the medical files were lost. These 21 patients were excluded from the study. Seventy-two patients were discharged because of repeated failures to appear, 22 were seen and discharged the same day and 56 patients were discharged administratively, either due to alterations in administrative practice or because they had not been seen for a year or more. Table 1 presents the demographics and headache diagnoses of these 150 patients on whom no further analyses were done.
Demographics and diagnoses of patients excluded from the study

The diagnostic groups are not mutually exclusive.
The remaining 336 patients had a mean age of 46 years (16–82), with a male/female ratio of 1 : 2.4. On average their treatment period was 7.8 months (0–18) with 5.7 visits (2–26). They were divided into two groups, based on whether they had a final diagnosis of MOH or pMOH. These two groups were then subdivided into mutually exclusive groups of headache diagnoses.
Table 2 presents the demographic and clinical characteristics of the 269 patients without MOH or pMOH. Overall, these patients had a mean age of 45 years (16–82), with a male/female ratio of 1 : 2.1. On average their headache frequency was 19 days/month (0–30) and their primary headaches had lasted 16 years (0–70).
Clinical characteristics at visit 1 of included patients without a diagnosis of medication overuse headache or probable medication overuse headache

The diagnostic groups are mutually exclusive.
Mean values are presented with range in parentheses.
Missing values.
Three patients fulfil criteria for chronic migraine,
two patients fulfil criteria for chronic migraine,
27 patients fulfil criteria for CTTH.
FETTH, Frequent episodic tension-type headache; CTTH, chronic tension-type headache.
Table 3 presents the demographic and clinical characteristics of the patients with MOH or pMOH. Initially, 106 patients fulfilled the diagnostic criteria for pMOH, but for 39 patients the MOH diagnosis was rejected since their reduction in headache frequency/intensity after withdrawal, was less than our defined cut-off at 50%. The remaining 67 patients consisted of 35 patients with MOH and 32 patients with pMOH. The pMOH diagnosis was given in 31 cases because the patient did not complete withdrawal and in one case because the necessary information about frequency after withdrawal was incomplete. Overall the patients with MOH or pMOH had a mean age of 46 years (20–74) with a male/female ratio of 1 : 3.8. On average their headache frequency was 27 days/month (15–30) and their primary headache had lasted 21 years (1–58).
Clinical characteristics at visit 1 of included patients with a diagnosis of medication overuse headache or probable medication overuse headache

The diagnostic groups are mutually exclusive.
Mean values are presented with range in parentheses.
Missing values.
TTH, Tension-type headache.
Table 4 presents the medication use of all patients at their initial visit, except for 10 patients where data were incomplete. The most widely used medications were simple analgesics (52%), triptans (32%) and combination drugs (24%), while ergots were rare (4%).
Medication use at visit 1, all patients
For the purpose of evaluating treatment efficacy, comparisons between first and final visits were made according to diagnoses, which implies that the groups are not mutually exclusive in the following.
Migraine, chronic TTH (CTTH) and frequent episodic TTH (FETTH) accounted for 83% of the diagnoses in patients without pMOH or MOH. Figure 1 shows headache frequency per month for these patients. A significant reduction in headache frequency was seen for FETTH, CTTH, migraine, cluster headache (P< 0.001) and other headaches (P< 0.01), while virtually no reduction was seen in the post-traumatic headache group.
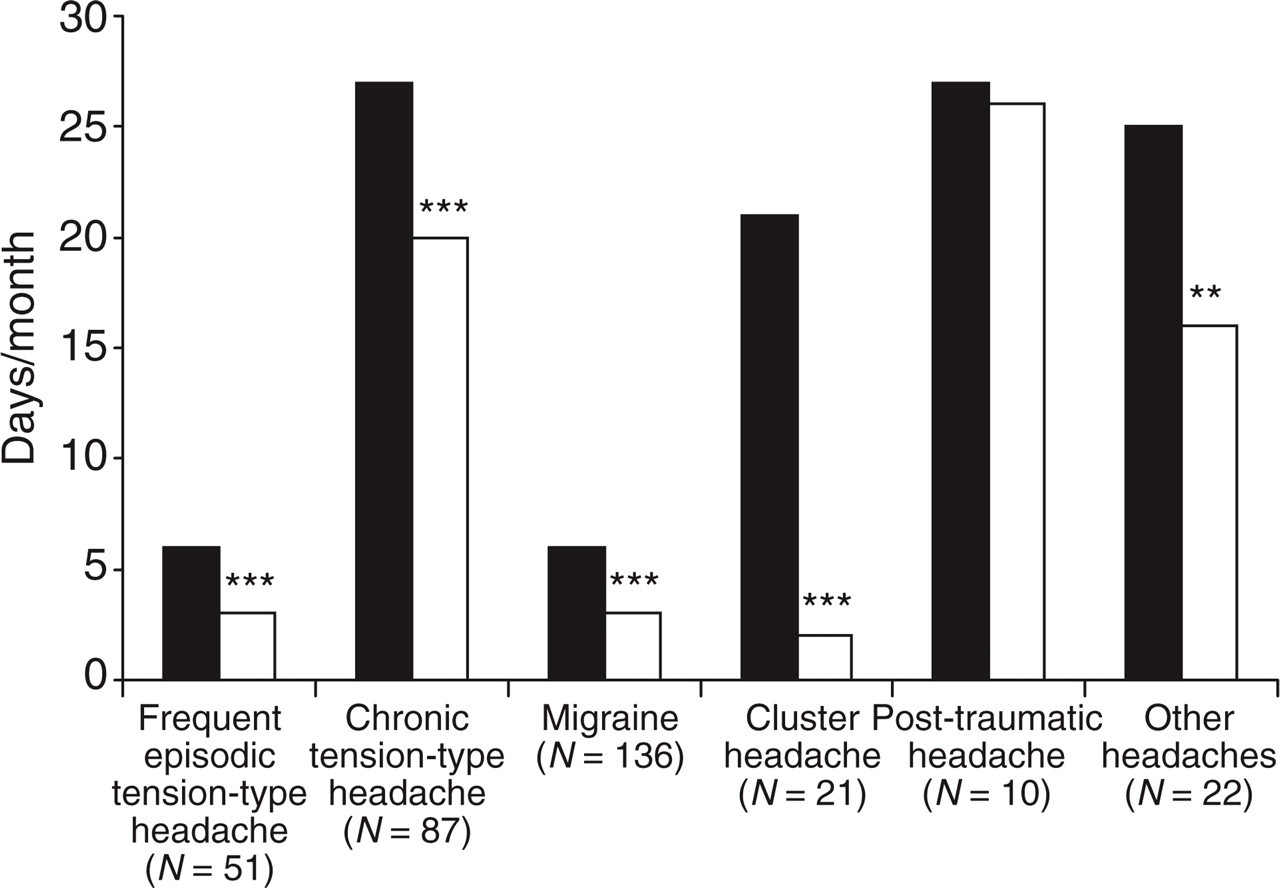
Headache frequency in days per month at first visit (▪) and at discharge (□), for patients without medication overuse headache/probable medication overuse headache. ∗∗∗P < 0.001; ∗∗P < 0.01; ∗P < 0.05.
Figure 2 shows headache intensity for patients without MOH. All groups, except the post-traumatic headache group, had a significant reduction in headache intensity.

Headache intensity (0–3 scale) at first visit (▪) and at discharge (□), for patients without medication overuse headache/probable medication overuse headache. ∗∗∗P < 0.001; ∗∗P < 0.01; ∗P < 0.05.
Figure 3 shows missed workdays for the same diagnostic groups as presented in Figs 1 and 2. All groups, except the post-traumatic headache group, reduced their number of missed workdays, but the reduction was significant only for migraine (P< 0.001) and FETTH (P< 0.05).

Missed workdays per month at first visit (▪) and at discharge (□), for patients without medication overuse headache/probable medication overuse headache. ∗∗∗P < 0.001; ∗∗P < 0.01; ∗P < 0.05.
For the MOH/pMOH group, the overall headache frequency per month is shown in Fig. 4. A significant reduction was seen for both TTH and migraine (P< 0.001).

Total number of headache days at first visit (▪) and at discharge (□), for patients with medication overuse headache/probable medication overuse headache. ∗∗∗P < 0.001; ∗∗P < 0.01; ∗P < 0.05.
Figure 5 shows specific headache frequency per month for the MOH/pMOH group. A significant reduction was seen for both migraine (P< 0.001) and TTH (P< 0.01).

Specific number of headache days at first visit (▪) and at discharge (□), for patients with medication overuse headache/probable medication overuse headache. ∗∗∗P < 0.001; ∗∗P < 0.01; ∗P < 0.05.
Table 5 presents the use of prophylactics for patients without MOH. Overall, 11% were on prophylactic treatment at first visit compared with 39% at discharge.
Use of prophylaxis for patients without a diagnosis of medication overuse headache or probable medication overuse headache
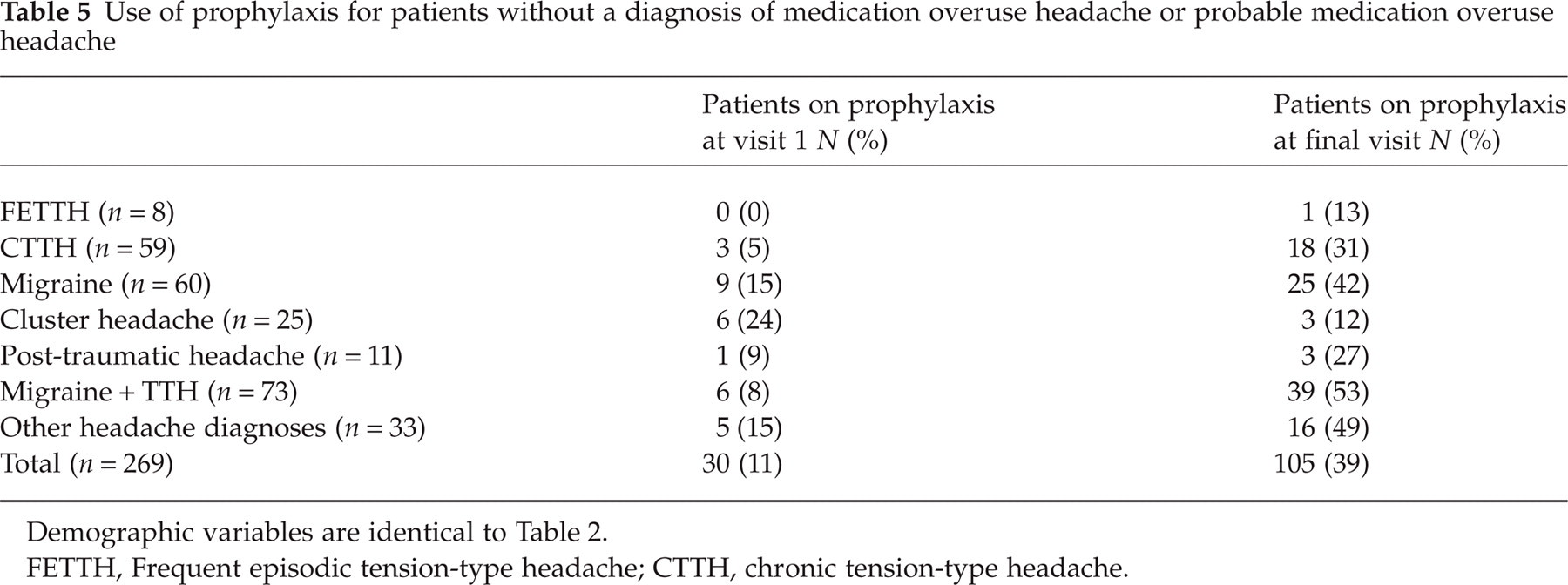
Demographic variables are identical to Table 2.
FETTH, Frequent episodic tension-type headache; CTTH, chronic tension-type headache.
Table 6 presents the use of prophylactics for patients with MOH/pMOH. Overall, 13% were on prophylactic treatment at first visit compared with 51% at discharge.
Use of prophylaxis for patients with a diagnosis of medication overuse headache or probable medication overuse headache
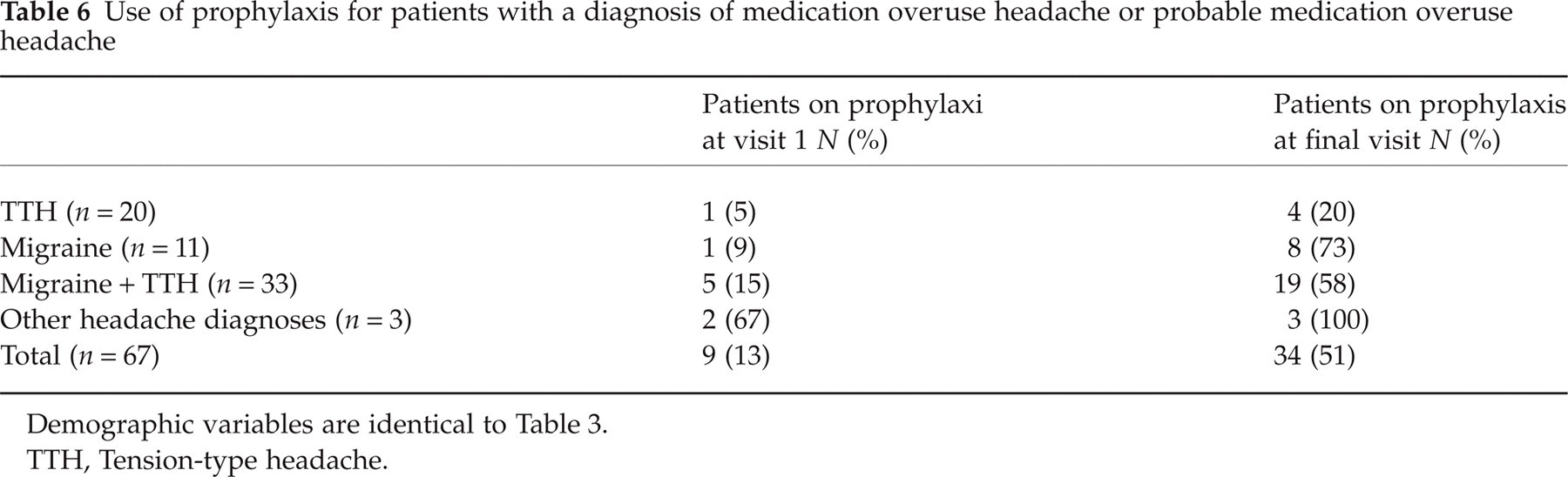
Demographic variables are identical to Table 3.
TTH, Tension-type headache.
Overall, 32% of the patients were referred to physiotherapy and 10% were seen by a psychologist.
During medication withdrawal 66% of the patients needed rescue medication while 34% stayed medication free. The average amount of levomepromazine used was 5 SD during a 2-month period (i.e. 1 SD equals 25 mg of levomepromazine).
With regard to prior prophylactic treatment, 26% of the patients had tried one prophylactic drug and 19% had tried two or more prophylactics before referral to DHC. Non-pharmacological headache treatment such as physiotherapy, acupuncture, chiropractor and different kinds of alternative treatment had been tried by 66% of the patients.
Discussion
The present study characterizes the patient population at the Danish Headache Centre during its first full year. To our knowledge, this is the first study to describe an entire headache centre population in detail with respect to headache diagnoses and treatment results for each diagnostic subgroup.
While most headache patients are treated in the primary care setting, complex or treatment-refractory headaches are usually referred to a specialized clinic. In order to justify the more expensive multidisciplinary treatment, it is essential for the tertiary headache centres to describe and evaluate their methods and results. Presenting the treatment results for each diagnostic subgroup separately is the simplest way of doing this. Although bias is a distinct possibility in this kind of open study, it may at least be used as an instrument to ensure that there is an effect. Furthermore, different results in different diagnostic categories will be unbiased and such comparisons may demonstrate diagnostic groups where the intervention is ineffective. These groups should be treated differently or re-evaluated elsewhere.
While the total number of patients in the present study is large, the numbers in the diagnostic subgroups are relatively small. As in all clinical situations, many patients were lost to follow-up. These drop-outs tended to be slightly younger and with less female preponderance, but did not differ markedly in diagnoses or other characteristics.
We realize that the cut-off at 50% reduction in headache frequency or intensity chosen for diagnosing MOH is an arbitrary and very strict criterion to apply. Nevertheless, since ICHD-II does not establish a definition for headache improvement, we preferred a conservative approach in order to ensure the specificity of the MOH diagnosis. Future studies with larger numbers may provide better evidence on how to adjust this definition.
The advantages of our study are the prospective recordings in diaries and questionnaires, the classification of all patients in accordance with ICHD-II, a reasonable follow-up time and lack of social bias due to free treatment for all patients.
The overall age and sex distribution in our study is in accordance with other Scandinavian out-patient headache clinics (6), but our patients tended to be older and with less pronounced female preponderance compared with two American headache clinics (7). For the MOH/pMOH group the age and gender distribution is similar to a recent German study reported by Limmroth et al. (8).
Epidemiological studies of primary headache disorders have reported rather consistent prevalence rates in different parts of the world. The last year prevalence in the general population was approximately 10–12% for migraine, 35–68% for FETTH and 4–5% for chronic daily headache (CDH), representing 2–3% with CTTH and 1.5–3% with MOH (2, 9–12).
Reflecting the profound selection bias in tertiary headache centres, we found that in the group without MOH, the diagnosis of CTTH, migraine and the combination of migraine and TTH accounted for, respectively, 22%, 22% and 27% of the patients. This relatively high proportion of pure CTTH in our study is in contrast to the 3% of pure CTTH reported by Sanin et al. from the Houston Headache Clinic (13). Only a small proportion at 4% (n = 5) of the migrainers fulfilled the new diagnostic criteria for chronic migraine.
In the group with MOH/pMOH, the diagnosis of TTH, migraine and the combination of migraine and TTH accounted for, respectively, 30%, 16% and 49% of patients. This differs from the diagnostic distribution found by Limmroth et al., who found a higher proportion of pure migraine and a lower proportion of combined TTH and migraine (8).
Surprisingly, almost one-third (106 patients) of all patients fulfilled the diagnostic criteria for pMOH at referral and 20% of the entire headache population (67 patients) were diagnosed as MOH/pMOH after withdrawel, using our rather strict definition of 50% reduction in headache frequency or intensity. This ‘response rate’ of 63%[(67/106) × 100] is comparable to the 56% of patients with CDH and analgesic overuse who responded to withdrawal with a similar 50% reduction in headache frequency in a Swedish study (14). We find it very important to identify all subjects with pMOH or MOH, as the outcome of MOH after withdrawal is usually excellent.
At the time of referral, the group without MOH had an overall headache frequency of 19 days/month, a moderate headache intensity and eight missed workdays/month. The duration of primary headache was 16 years. The MOH group was even more disabled, with an overall headache frequency of 27 days/month, similar headache intensity, but they had missed 11 workdays/month and had suffered from primary headaches for 21 years. Thus, the referred patients are severely affected and disabled, implying that the human and financial benefits of headache improvement will be considerable. In a comprehensive analysis of patients attending an American tertiary referral centre for headache, Saper et al. found a similar headache frequency at referral of 23 days/month, but much fewer missed workdays, namely 5.5 days per 6 months period (15). There are no comparable European studies.
In contrast to expectations, our results indicate that it is possible and even highly rewarding to treat this severely affected group of patients seen in a tertiary headache centre. Both frequency and intensity of headaches and absenteeism from work decreased significantly, although there are differences between the diagnostic subgroups.
In the group without MOH the headache frequency for both FETTH and migraine was reduced by 50%, while the frequency of CTTH was reduced by only 26%. Despite the modest reduction in headache days in CTTH, the corresponding 35% decline in headache intensity yields a satisfactory treatment result and the reduction in frequency is comparable to prior clinical prophylactic trials of amitriptyline (16). Virtually no reduction in headache frequency or intensity was seen in the post-traumatic group, underlining the difficulty in managing these patients. This is in accordance with a recent study from the DHC, where Baandrup and Jensen analysed 53 patients with post-traumatic headache. They found that the prevalence of coexisting analgesic overuse was 42% and the treatment outcome for this subgroup of patients was just as favourable as in primary headaches. However, the outcome of chronic post-traumatic headache without MOH was poor (17).
In the MOH/pMOH group the reduction in total headache frequency was 50% for TTH and 72% for migraine, while the reduction in specific headache frequency was 35% and 80%, respectively. These findings suggest a better outcome for migraine than for TTH following withdrawal from MOH, a tendency also reported by Schnider et al., although not significant, in a 5-year follow-up study (18). The positive outcome in migraine may also reflect the better effect and higher number of prophylactic drugs for migraine, compared with CTTH.
Despite their long history of headache, relatively few patients used pharmacological prophylactic treatment at time of referral, namely 11% in the group without MOH and 13% in the MOH/pMOH group. At the time of discharge this was changed to 39% and 51%, respectively, which is undoubtedly a contributory factor to the obtained results. Still, it is important to emphasize that it is the effort of a combined multidisciplinary treatment that has shown efficacy, and not a single factor. The relatively small proportion of patients (10%) seen by a psychologist was due to a limited capacity in 2002. It is noticeable that almost half of the population had a history of prior pharmacological prophylactic treatment and two-thirds of patients had tried non-pharmacological headache treatment.
In interpreting our results, it is important to consider the possibility that our treatment results could be a placebo effect. However, the long duration of headache and the failure of multiple prior treatment strategies make this less likely. In clinical randomized trials of CTTH patients and other chronic pain patients with a similar duration of pain, the placebo effect varies from 10 to 15% (16). The long observation period is also likely to diminish the placebo effect.
With an average of 5.7 visits during 7.8 months, the management of these complex patients is not very time-consuming. If our results can be maintained, the present concept seems to be highly cost-effective for both patients and society.
Footnotes
Acknowledgements
We thank our laboratory technician Mrs Hanne Andresen for helpful technical assistance during the data collection. The study was supported by grants from ‘IMK Almene Fond’.