
Abstract
Introduction: Despite the high prevalence of headaches, multidisciplinary headache clinics are few and their efficacy still needs validation. The objective was to characterise patients and treatment results in a tertiary headache centre.
Subjects and methods: A systematic review of all referred patients in the Danish Headache Centre in a 2-year period. Outcome results were analysed with respect to diagnoses and sociodemographics.
Results: A total of 1326 patients with a mean age of 43.7 years and male : female ratio of 3 : 7 were included. In total, frequency and absence rate from work were reduced from 20 to 11 days (P < 0.001) and 5 to 2 days/month (P < 0.001), respectively. Predictors for good outcome were female gender, migraine, triptan overuse and a frequency of 10 days/month, whereas tension-type headache and overuse of simple analgesics predicted a poor outcome.
Conclusions: The present analysis provided support for a multidisciplinary approach in a tertiary headache centre. Further evaluation of specific treatment strategies and outcome predictors are important for future planning.
Introduction
Over decades, multidisciplinary clinics have been established for the treatment of general pain disorders and the International Association for the Study of Pain (IASP) has published guidelines for the organisation and structure of such clinics (1–3). In recent years, the need for specific headache clinics has become evident and their numbers are growing; however, despite the frequency of both pain and headache clinics, documentation of their results and organisation have been poorly described or evaluated (4–8).
Globally, headache disorders represent a substantial burden, not only on individual patients and their families, but on the whole of society (9–13). While headache research has progressed enormously during the last decade, few have been interested in the organisation of optimal headache care. This is a matter of concern since, in the general adult Danish population, the life-time prevalence of a headache-related consultation was 32% with primary care physicians, 16% had had a neurological consultation and 3% had been admitted to hospital because of headache (13).
This significant use of healthcare resources by headache patients calls for a national healthcare plan. Guidelines for the organisation of headache clinics have recently been published from the European Headache Federation (EHF) (14). These guidelines suggest a three-tier system – general practice, neurological specialist and multidisciplinary tertiary referral centre. However, proper evidence for the suggested multidisciplinary treatment approach and the cost-benefit of such clinics are still lacking.
In 2006, we described the organisation and initial results from the Danish Headache Centre (DHC) (6), but similar studies that describe procedures and large-scale outcome results are lacking. With this background, we aim to describe the treatment strategies and the outcome results from the DHC.
Subjects and methods
Organisation of the Danish Headache Centre
DHC was inaugurated in 2001 as a tertiary out-patient referral headache centre, organised within the Department of Neurology, Glostrup Hospital (6). The main uptake area was Copenhagen County with a population of 600,000. In addition, DHC also functioned as the only national referral centre for severely affected headache patients in Denmark (in total 5.5 million inhabitants).
The capacity was initially 700 new patients per year; due to excessive demand, the intake was increased to 1000 patients per year during the following years. In addition, the headache centre co-operated closely with the Clinical Department of Neurology and an initial in-patient facility with two beds was made available for severely affected patients with medication overuse or in need of specific and planned observation. This capacity was increased to six beds in 2005. Acute, general, neurological service in the emergency room is available, but DHC offers no specific service for patients with acute headache attacks.
Initially, the staff in the headache centre consisted of 4 part-time senior headache specialists supplemented by junior doctors on rotation, 2 physical therapists, 2 psychologists, 2 part-time nurses and 3.5 secretaries; during the following years, the staff has gradually expanded. Patients must be referred from a general practitioner (GP), from practicing neurologists or from other neurological departments. All levels of medical consultation are publically financed in Denmark and free of cost to the patient, whereas medication is only partially reimbursed.
Diagnosis
Before their first visit, all patients receive a diagnostic headache diary and are told to record headache characteristics, including type and amount of medication used, prospectively for at least a 4-week period (15). They also fill out a questionnaire regarding status of health, impact on work, family and social life and prior headache treatment.
A detailed headache history is obtained by means of a standardised procedure at the initial consultation that lasts 90 min (junior doctors supervised by neurologists) or 60 min (neurologists). The history is supplemented by the diagnostic headache diary and the general medical questionnaire. After a complete general physical and neurological examination, all first visit patients were classified according to ICHD-I (16) and later to ICHD-II (17).
The diagnostic headache diary was examined and ICHD-diagnoses, headache frequency, intensity and medication consumption at the time of the initial consultation are recorded as baseline values.
A detailed treatment strategy is planned with the patients, based on optimized medical treatment, self-responsibility, education and repeated visits in the clinic. Depending on need, patients are referred to a physical therapist, psychologist and/or nurses. During the treatment period, most patients are seen by the neurologist at control visits lasting 20 min every 2–4 months and they are encouraged to use a headache calendar recording attack frequency, severity and medication use during their entire treatment period. When the headache condition is stable and acceptable, patients are referred back to their GP with detailed information about further treatment strategy and plan in case of relapse. For each discharged patient, the following data are available: the medical record, a diagnostic diary, a detailed questionnaire, a headache calendar and an outcome questionnaire recorded by the doctor at the final visit describing headache diagnoses, frequency, use of medication and missed workdays.
Physical therapy
Patients suffering from tension-type headache (TTH) or combined headaches with significant pericranial muscle tenderness are referred to physical therapists. The sessions are individual. They consist of a detailed examination of posture and muscular function. Patients are instructed in active exercises and detailed information about identification and avoidance of possible muscular stress factors. Patients are also encouraged to a daily, individualised exercise programme. Passive treatment strategies such as massage or ultrasound are avoided.
Psychological therapy
Patients with stress, anxiety or suspected psychological trigger factors are referred to psychologists. They primarily use group sessions (8 patients) and focus on stress management (cognitive and behavioural techniques) and bio-feedback relaxation. All referred patients are interviewed by psychologists and thereafter included in the relevant group therapy programme. Only a minority of patients is offered individual psychological guidance or therapy in the centre.
Headache nurses
Patients who fulfil the diagnostic criteria for medication overuse headache (MOH) are referred to our specialised nurses for treatment which consists of: (i) individual detoxification after detailed information; (ii) an out-patient teaching programme (The Headache School) where groups of 5 or 6 MOH patients are guided through their detoxification period; or (iii) an in-patient programme for 2 weeks (18). The nurse’s main responsibility is as co-ordinator of the multidisciplinary treatment of MOH and as a medical co-advisor for headache treatment in general. In MOH patients, all acute headache medication is discontinued abruptly and patients are kept medication free for 2 months with frequent support from the nurses (18).
Other medical specialities
Structured relations with other departments in the hospital are formalised and co-operation with the Department of Neurosurgery regarding trigeminal neuralgia, idiopathic intracranial hypertension, hydrocephalic conditions and similar problems is established. Likewise, an efficient collaboration with the Department of Gynaecology has been developed due to the problems related to menstrual migraine, hormonal treatment and pregnancy. An experienced anaesthesiologist performs the blood patch treatment to the patients with low-pressure headache. If co-morbid psychiatric disorder is suspected, a referral to a specific psychiatrist with interest in headache and pain is initiated. A dentist with specific orthodontic experience has also been allocated once a month for a specialised evaluation of selected patients.
Statistical analysis
We present data for all patients discharged from DHC in a 2-year period. All data were loaded in a Microsoft Access database and the Wilcoxon signed rank test used for paired comparisons. P-levels below 0.05 (two-tailed) were chosen as level of significance.
Predictive factors for outcome were included in the analyses on the basis of significance in prior studies. A positive outcome was defined as a reduction in headache frequency (days/month) of 50% or more. Variables included in the model were: age, gender, migraine, familial disposition, educational level, marital status, work conditions, social compensation claim, head or neck trauma, early start (onset before the age of 20 years), headache frequency, co-existing primary headaches, frequent use of medicine, use of prophylactic treatment (migraine), sleep problems, snoring, chronic illness, self-rated health, physical activity and smoking. Marital status was dichotomised to single if the participant was not married or co-habitating with a partner or as not-single. Social compensation claim was dichotomised to YES/NO and the highest achieved educational level was dichotomised to any secondary education (vocational training, college degree or university degree) or no secondary education (obligatory primary schooling including high school). Included diagnoses were migraine without aura (MO), migraine with aura (MA), TTH, cluster headache and MOH. Age, baseline frequency, medicine use, duration, absence from work were modelled by smooth non-linear functions in a generalised additive model (19) and tested against simpler functions. The generalised additive model is a flexible model, which includes the usual multivariate logistic regression model as a special case. In the generalised additive model, we allow the relationship between the log-odds (the linear predictor) and the predictors on continuous scale to be smooth functions estimated from data, whereas these in the usual logistic regression model are restricted to be linear functions. The smooth functions can be tested for significance and against simpler functions alternatives such as linear functions. In Table 4, for example, the function for the initial frequency could be simplified to two regimens each consisting of a linear function. In all analyses, the generalised additive model could be reduced to the standard multivariate logistic regression. Sub analyses for outcome of patients with and without MOH were performed.
The predictive factors were further analysed with univariate and multivariate logistic regression. Odds-ratios and 95% confidence limits were calculated, statistical significance is present if the confidence interval for the odds-ratio does not overlap 1. Multivariate models for each category of risk factors were constructed by including relevant risk factors. Hosmer and Lemeshow’s Goodness-of-fit test was used as control of model fit. All data analyses were made using the SAS statistical package V8e, SPSS v.12.0-16.0 and R v.2.7.1.
Results
During a 2-year period, a total of 1907 new patients were referred and a complete dataset of 1326 treated patients were analysed. All treated patients who had finalised their treatment during this 2-year period were included in the present results. The mean age was 43.7 years (range, 13–92 years) and the male : female distribution was 3 : 7 with 406 males and 920 females (Table 1). The mean duration of headache was 10.6 years with a wide range from 0–76 years. Their mean treatment period was 477 days (median, 10 months), 43 (3.2%) patients were only seen once and 20% were finalised due to administrative reasons such as loss of contact or absence from scheduled appointments. The overall frequency of headache at admission is displayed in Figure 1.
Distribution of patients in relation to frequency at admission to the Danish Headache Centre (n = 1326). Clinical characteristics of patients from Danish Headache Centre (n = 1326) Mean values with range or percentage value indicated in brackets. Indicates missing values. Regarding employment status, 22.1% were unskilled, 8.6% skilled workers, 55.4% salaried employees and 4.6% self-employed with an expected male/female distribution where skilled work was more frequent in males and salaried employment more frequent in females. Regarding public social compensation, 93.4% did not receive social compensation due to headache, 2.7% had applied for or received early retirement pension due to headache, 1.4% for other compensation and 2.4% had on-going insurance or compensation claims.

Concerning demographics, all patients were Caucasian. Fifty-eight patients (4.4%), 47 females and 11 males, were unable to speak Danish and needed translational assistance.
The most frequent diagnoses of primary headache were migraine without aura (50.9%), frequent episodic tension-type headache (f-ETTH; 21.6%) and co-existing migraine and TTH (32%). The distribution of migraine, TTH and co-existing migraine and TTH in relation to frequency is presented in Figure 2.
Distribution of patients with migraine, tension-type headache or co-existing migraine and tension-type headache in relation to frequency at admission to the Danish Headache Centre (n = 1326).
Distribution of ICHD-II diagnoses according to gender

Absolute values are indicated with percentage values (of male : female ratio and of the total population, respectively) in brackets. On average, 1.7 ICHD diagnoses were encountered per patient.
MO, migraine without aura; MA, migraine with aura; PM, probable migraine; fETTH, frequent episodic tension-type headache; CTTH, chronic tension-type headache; PTTH, probable tension-type headache; TAC, cluster headaches and other trigeminal autonomic cephalalgias; TN, trigeminal neuralgias.
Characteristics of headache and their treatment outcome in relation to diagnosis

Mean values are indicated with range in brackets and level of significance with asterix (*P < 0.05, **P < 0.01 and ***P < 0.001).
#Indicates missing values; aindicate migraine or TTH without MOH and §indicates that 31/49 cluster headache patients were headache free after treatment.
When chronicity was defined as headache for 15 days or more per month, 55% (n = 729) had chronic headaches on admission including those 337 individuals with MOH (Figure 1). When subjects with MOH were subtracted, chronicity was most pronounced for patients with tension-type headache where 81% presented with a headache frequency of 15 days per month or more, whereas the similar figure was 54% for the mixed migraine and tension-type headache (Figure 2). Chronic migraine (≥15 days per month with headache fulfilling the core ICHD-II criteria for migraine) without co-existing MOH occurred in 14% of the pure migraine population and only in less than 3% of the entire patient population. According to the appendix criteria for chronic migraine, only 7% of patients without MOH had chronic migraine (migraine ≥8 days per month and headache ≥15 days per month) (20).
On average, these 1326 patients were seen 5.6 times in DHC. Of these 337 patients with MOH, 67 patients participated in the headache school, 33 had been treated in our in-patient detoxification programme and the remaining 238 patients managed their detoxification individually after careful instruction and follow-up visits.
In the total material, the frequency of headache was reduced from 20 days/month on admission to 11 days/month at the end of treatment, with a major variation between diagnoses – migraine having the most prominent reduction. Among the 49 patients with cluster headache, 31 (63%) became completely headache-free; among the remaining 18 patients, both attack intensity and duration decreased significantly (P < 0.001). Regarding severity and duration of other headaches, the dataset was not complete but a significant reduction was also seen in all groups (Table 3).
Non-Danish speaking patients had a significant effect of their migraine treatment (from 4.3 days to 2.8 days/month; P < 0.01) whereas there was no effect on TTH frequency (from 13.5 to 15.0 days per month; P = 0.5).
Sickness absence from work decreased significantly from 5 days per month initially to 2 days per month after treatment, with a significant reduction in all major headache groups (Table 3).
Predictive factors for a good outcome (≥50% reduction of frequency) of the treatment programme in DHC (n = 1326)
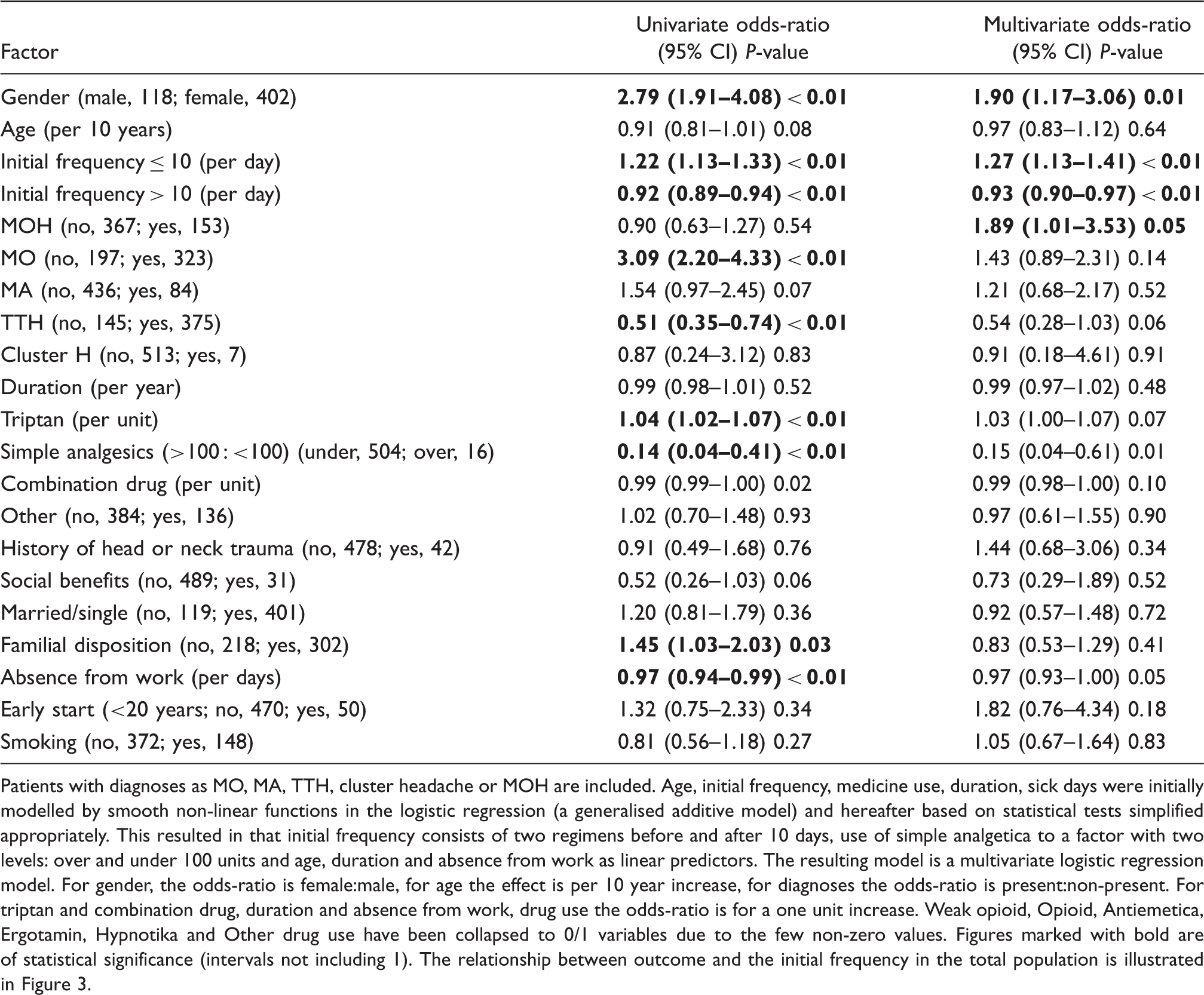
Patients with diagnoses as MO, MA, TTH, cluster headache or MOH are included. Age, initial frequency, medicine use, duration, sick days were initially modelled by smooth non-linear functions in the logistic regression (a generalised additive model) and hereafter based on statistical tests simplified appropriately. This resulted in that initial frequency consists of two regimens before and after 10 days, use of simple analgetica to a factor with two levels: over and under 100 units and age, duration and absence from work as linear predictors. The resulting model is a multivariate logistic regression model. For gender, the odds-ratio is female:male, for age the effect is per 10 year increase, for diagnoses the odds-ratio is present:non-present. For triptan and combination drug, duration and absence from work, drug use the odds-ratio is for a one unit increase. Weak opioid, Opioid, Antiemetica, Ergotamin, Hypnotika and Other drug use have been collapsed to 0/1 variables due to the few non-zero values. Figures marked with bold are of statistical significance (intervals not including 1). The relationship between outcome and the initial frequency in the total population is illustrated in Figure 3.
Non MOH

Predictive factors for a good outcome (≥50% reduction of frequency) of the treatment programme in DHC for patients without MOH. The analysis is as in Table 4, but with the simple analgesics as the number of units.
MOH

Predictive factors for a good outcome (≥50% reduction of frequency) of the treatment programme in DHC for patients with MOH. The analysis is as in Table 4, but with the initial frequency having a single regimen and the cluster headache omitted since no cases are present.
Discussion
Optimal controlled study designs are very difficult, if not impossible, to apply to multidisciplinary headache treatment. Several presumably beneficial interventions are applied at the same time to these severely affected patients, who are threatened by job loss or other social distress. Paradoxically, this complex group of patients is most in need of improved treatment strategies. We, therefore, publish our clinical data, which is collected in a systematic and prospective design to achieve knowledge and evidence. Randomisation to either specialised treatment or a control group would be preferable, but difficult, for practical and ethical reasons. Our treatment results should be interpreted with some caution while between-group comparisons and multivariate analyses are less likely to be biased.
With the present analysis, we may contribute to the development of future and proper state-of-the-art studies. Despite increasing popularity, only very few headache centres are based on academic neurological traditions, evidence for the applied multidisciplinary treatment approach are scarce (5–8), and large-scale cost-effect analysis of such clinics are lacking. Likewise, randomised controlled studies to document the effect of the individual elements of a multidisciplinary treatment are also very few; to our knowledge, documentation of the various combinations of elements is non-existing. The need for a systematic quality control and continuous evaluation of our own clinical activities is also emphasised as the present treatment results vary considerably between the different patient groups. Patients with post-traumatic headache (PTH) have, for example, a poor outcome documented in a prior study of a rather small group of patients from our centre (21). This calls for a complete re-evaluation of the treatment strategy of post-traumatic headache and a randomised controlled treatment study has been initiated. The outcome of migraine and MOH is, on the other hand, positive in agreement with prior reports from other highly specialised centres in Europe and the US (5–8,20,22–25).
Overall, the results from our national headache centre are fairly positive. A certain placebo effect is obviously expected although patients referred to our headache centre have previously been regarded refractory or very difficult to treat in primary or secondary care. This patient group has, on average, suffered from headache for 10.6 years, have several prior healthcare contacts and their expectations are low. In prior interventional studies of chronic tension-type headache with a long duration of disease (26,27), the placebo response rate was below 15% whereas the placebo effect in episodic migraine may be above 30% (28–30), indicating that the present outcome with an overall reduction in headache frequency of 45% in our difficult-to-treat patients is unlikely to be a placebo effect.
Our criteria for referral to our centre are refractory headaches, rare or atypical headaches or facial pain including trigeminal neuralgia. Denmark has a managed healthcare system free of cost to patients. Organisational or financial barriers for patients are, therefore, unlikely to influence our results, also supported by the fact that the societal status in our patient sample is representative to the general Danish population. The age and sex distribution is similar to other clinical settings (4,31) and, as expected, the male : female ratio is according to the headache diagnosis from 1 : 3 in migraine to 2 : 1 in cluster headache.
The ICHD-II classification is the diagnostic standard in the centre. Others have found it complicated and difficult to use (32–34); however, the present study demonstrates that it is useful in a tertiary headache centre with severely affected patients. Only 0.2% (24/1326) could not be classified according to ICHD-II which is an exhaustive system in our hands. A systematic use of ICHD-II combined with the prospective headache diary ensures precise diagnosis for almost all patients. The major complaint about ICHD-II is that several diagnoses are necessary per patient. In the present sample, 1.7 diagnoses were applied per patient and a detailed analysis will be published later. Our patients are probably similar to other materials from other tertiary centres, as 55% had chronic headaches at admission with considerable variation among diagnostic groups. Chronic headache is most prevalent in patients with MOH and TTH and less prevalent in migraine patients and intermediate in patients with mixed migraine and TTH.
Only 3% of the patient population had chronic migraine without co-existing MOH according to the official ICHD-II criteria and 7% if the suggested appendix criteria are applied (20). The vast majority of chronicity in our migraine patients was thus related to medication overuse. The fairly high frequency of MOH and the very low frequency of chronic migraine contrasts with other reports from specialised centres (35,36) and may be due to our strict application of ICHD-II criteria and the requested, prospective use of a headache diary to record intake of analgesics and migraine drugs for at least 4 weeks.
In the general population, 42% of migraineurs and 45% of those with frequent tension-type headache reported a spontaneous resolution over a 12-year period (37). In clinical series of severely affected headache patients, spontaneous resolution is unknown. In the general population, it was demonstrated that risk factors for a poor outcome in migraine were early onset of disease (age < 20 years) and a high migraine frequency whereas in chronic TTH life-style factors such as poor sleep and not being married indicated a poor outcome (37). In the present study, female gender and MOH, especially with an overuse of triptans, were predictors of a good outcome (meeting the strict frequency reduction of 50% or more) whereas overuse of simple analgesics indicated a poor prognosis. Unexpectedly, age, duration of headache, number of absence days from work or receipt of social benefits did not influence the outcome in the present study. Other variables of possible importance for the outcome may be defined in future studies.
Outcome in relation to diagnosis
Migraine with and without aura had a positive outcome independent of age and headache duration. Likewise, TTH patients had a substantial reduction in headache frequency, although more modest than seen in migraineurs. Cluster headache also had a very positive outcome yet the underlying chronobiology with periodic symptoms probably makes a large contribution. As documented in a prior publication by Jensen et al. (38), correct diagnosis and information are, nevertheless, of major importance in cluster headache; after treatment in our centre, the use of medical contacts was dramatically reduced. Outcome of MOH was also very favourable. It may be resource demanding and involve several members of the multidisciplinary team. Ninety percent of the MOH patients were treated on an out-patient basis whereas only 33 patients in the present data set had been admitted to the in-patient programme (for further details, see Zeeberg et al. (6,39)). According to our data, the predictors of a good outcome of MOH-patients were triptan-overuse, whereas a marked overuse of simple analgesics (such as 100 tablets or more per month) or combinations of analgesics was predictive of a poor outcome.
An interesting, predictive indicator for our selected outcome parameter with 50% reduction in headache frequency was the initial frequency at admission for all patients (Figure 3) and it was also present in relation to a diagnosis with and without MOH. It can be seen that the initial frequency with the highest chance of a successful outcome is 10 days, whereas lower frequencies lead to a much lower chance of a successful outcome with regard to frequency, e.g. the chance of a successful outcome with a frequency of 4 days is the same as for 30 days. The most likely explanation for the fairly specific frequency of 10 days could be that it is more complicated to modify the exact frequency in patients with less frequent headaches, i.e. menstrually related migraines or tension-type headache, whereas the attack duration and/or intensity may be markedly reduced by the applied treatment strategies. In contrast, a less favourable outcome was expected in patients with a higher headache frequency, especially in those with chronic headaches occurring 15 days or more per month. It could, therefore, be of interest to apply this statistical model to future studies, with a specific focus on diagnostic criteria for chronicity and the problematic diagnostic groups as chronic migraine or chronic tension-type headache.
Odds-ratio for initial frequency. Reference is a initial frequency of 10 days. Black curve is the multivariate (corrected) effect and hatched line the univariate.
The present dataset contains relatively few patients with secondary headaches other than MOH and a detailed outcome analysis of the individual diagnoses could not be performed. A prior study from our centre demonstrated a poor outcome in patients with PTH. Only those PTH-patients with a subsequent medication overuse demonstrated some benefit from the multidisciplinary treatment (21). These results suggest that a different treatment strategy should be developed as discussed above.
Study limitations
The limitations of our study are the absence of a control group and missing data. The various combinations of pharmacological and non-pharmacological treatment strategies within the same patient over time may be very positive for final outcome but we find the contribution of the individual therapeutic elements difficult to quantify. The dataset represents only those patients who have finalised their treatment in DHC, and not our entire intake of patients during this 2-year period. We defined a clear cut-off and requested finalisation of the treatment in this outcome study. This selection may, therefore, be in favour of a positive outcome as the difficult to treat patients, i.e. with chronic cluster headache, post-traumatic headache, significant co-morbidity or complexity were offered to have longer lasting connection to DHC.
The advantage of the study is the free healthcare system, the standardised treatment approach, the large group of severely affected patients, the careful diagnostic process according to the ICHD-system, the systematic use of diaries and follow-up consultations per need.
Our previous epidemiological, clinical and basic research covering most aspects of headache has been fundamental for the construction of, and have helped us in devising, the clinical approach to patients at the Danish Headache Centre. Likewise, the multidisciplinary team offers several advantages to a clinical centre with a high complexity of patients as it allows dialogue, education and promotes further development of methods in addition to an increased capacity.
Detailed reviews of a comprehensive treatment programme have been published from a private US clinic (7,8). Like the present results, a positive 6-month outcome of treatment in a multidisciplinary headache centre was reported despite a severely affected patient population, classified as refractory or difficult to treat at admission (8). Although such data may be difficult to apply to the individual patient, they may guide the headache specialist to inform the patients on a much better scientific background and provide the patient with more realistic expectations. A balance between patient expectations and the available treatment possibilities is probably the best indicator for a positive outcome, although difficult to study and measure in clinical practice.
Whether an early, combined intervention with pharmacological prophylaxis and life-style changes can improve the long-term outcome remains also to be documented and should be studied in large-scale, long-term studies.
However, we were not able to identify the most significant individual predictor for a poor or a good outcome, as most of the included factors are closely related. Overall, it is our clinical impression that severe co-morbidity, especially depression and anxiety, personality disorders and insufficient coping strategies are of major influence for the outcome, but unfortunately we have not recorded these variables such systematically in the present dataset. Identification of outcome predictors and cost-benefit analysis are, nevertheless, very important for future treatment, guidance and planning of headache services and collection of such detailed information is now on-going for subsequent publication. According to our referral system, our patients are highly selected and, obviously, the present results cannot be transformed to primary or secondary practice in other settings. On the other hand, those severely affected patients are those that are in need for effective treatment; despite their so-called refractory headache disorder it is nevertheless possible to reduce their headache frequency and improve the disability markedly.
Conclusions
This study has provided support for the usefulness of a multidisciplinary approach to the complex headache patient. Prospective and controlled outcome studies of specific diagnostic categories are needed, as are studies of the effect of the different components of the multidisciplinary treatment.