
Abstract
Background
The short-lasting unilateral neuralgiform headache associated with conjunctival injection and tearing or SUNCT syndrome was first described in the 1970s. This paper is the first in the literature that describes the successful use of stereotactic radiosurgery (SRS) using a non-invasive frameless technique, targeting both the trigeminal nerve and the sphenopalatine ganglion in the management of intractable SUNCT. We also discuss the role of selecting peripheral targets in the management of this rare headache syndrome.
Methods
Among patients treated for functional pain disorders in our radiosurgery unit using the frameless technique since August 2011, one patient with symptoms matching the International Classification of Headache Disorders-2 (ICHD-II) criteria of SUNCT syndrome was identified. The multi-disciplinary case records of this patient were retrospectively reviewed and reported.
Results
Our patient had symptoms resembling the ICHD-II diagnostic criteria of SUNCT, which was refractory to medical treatment. Ninety Gy was delivered to the trigeminal root entry zone and 80 Gy was delivered to the sphenopalatine ganglion. At 16 months’ follow-up, she was pain free with minimal side effects.
Conclusions
Frameless linear accelerator (linac)-based SRS targeting the trigeminal nerve and sphenopalatine ganglion remained successful in our patient at 16 months. Longer follow-up and further experience will determine the efficacy and safety of this approach. We suggest that frameless SRS is a convenient and attractive non-invasive option for patients with medically refractory SUNCT.
Keywords
Introduction
SUNCT is a rare headache syndrome describing a short-lasting unilateral neuralgiform headache associated with conjunctival injection and tearing (1). To date, multiple case reports and series of SUNCT treated with various strategies have been described but its exact pathophysiological mechanism remains unclear (2). Treatments that have been used for medically intractable SUNCT are divided broadly into central and peripheral approaches, whereby the central approach targets the hypothalamus using deep brain stimulation and the peripheral approaches target the greater occipital or trigeminal nerve with procedures including nerve blockade, rhizotomy, microvascular decompression and radiosurgery (3). Experience in the literature regarding stereotactic radiosurgery (SRS) is scarce and so far only four cases have been reported using Gamma knife (GK) with mixed results (4–6). We present a case of SUNCT treated in our institution using frameless SRS.
Materials and methods
Our institution transitioned from GK SRS to Novalis SRS in 2007. The Novalis system (BrainLAB AG) is a purpose-built linear accelerator (linac) system for the delivery of SRS that is capable of delivering radiosurgery using a frameless technique. Immobilization is achieved with a head mask system, while stereotaxis is achieved by image-guidance using an integrated stereoscopic X-ray-based localization system coupled with a 6D robotic couch (7) (Figure 1). Recently, initial outcomes of frameless SRS for trigeminal neuralgias have been reported and shown to be safe and effective (8). After gaining about four years of experience with frameless SRS and confirming the accuracy and reliability of our Novalis system with our physics department and from the literature (9), we started treatment of our trigeminal neuralgias (TN) without invasive frames in August 2011. Among patients treated for functional pain disorders in our unit, there was one patient with symptoms matching the ICHD-II criteria of SUNCT syndrome. This patient was managed in a multi-disciplinary setting involving neurology and pain management, along with the neurosurgeon and radiation oncologist who jointly performed radiosurgery. The multi-disciplinary case records of this patient were retrospectively reviewed and are reported below.
Novalis frameless radiosurgery system. Source: Used with permission from Brainlab AG, taken from http://www.novalis-radiosurgery.com.
Our patient is an 83-year-old woman who was seen at the pain clinic beginning in November 2010. Her pain was daily and episodic in the right temporal and orbital regions. It was described as sharp and electric-shock like, occuring between six and 10 times a day and lasting between five and 30 minutes. This was associated with tearing and injection of the right eye and rhinorrhea. It was exacerbated by touching of the right face, brushing, eating and chewing. There were no neurologic deficits and her magnetic resonance imaging (MRI)/magnetic resonance angiography (MRA) scans were normal, although there was a suggestion of mild neurovascular conflict at the root entry zone (REZ) of the right trigeminal nerve. She failed oxygen therapy and was treated with escalating doses of gabapentin and carbamazepine. Lamotrigine at 100 mg daily given in combination with carbamazepine 200 mg twice daily in the subsequent few months provided only partial relief. Five months later, her pain attacks were occuring eight to 20 times a day and each episode lasted a minimum of one to two minutes but not more than five minutes. She was given a trial of indomethacin 25 mg three times daily for about two weeks that failed, but there was some response to gabapentin. A month later, she reported that the pain had become more frequent, often occuring multiple times within an hour but shorter in duration, sometimes lasting only a few seconds. She went on to try accupuncture, which did not help. In summary, this patient’s pain evolved over a period of six months, becoming more frequent but shorter in duration while remaining similar in quality and intensity, and accompanied by autonomic symptoms during the attacks. Despite initial improvements with dose increments her pain kept returning, and the side effects of debilitating giddiness with gabapentin 400 mg twice daily and drowsiness with higher doses of carbamazepine ultimately limited further escalation. Up to that point, she had been on a combination of carbamazepine 100 mg twice daily, gabapentin 300 mg twice daily, and nortriptyline 20 mg every night. She was referred to the neurosurgeon, who discussed options of nerve block, microsurgery and frameless SRS. She opted for the least invasive option and had radiosurgery in October 2011.
Immobilization was performed with the Brainlab relocatable head mask, and computed tomography (CT) simulation was performed with 1 mm slices. MRI three-dimensional (3D) constructive interference in steady state (CISS) sequence with 1 mm cuts was performed and fused using the Brainlab iPlan software version 4.11. The trigeminal nerve was contoured and the sphenopalatine (SP) ganglion was identified by tracing the maxillary nerve out of Meckel’s cave and contoured accordingly. Using a 4 mm cone, the isocenter was placed at the REZ of the trigeminal nerve, ensuring that the 50% isodose line was at the edge of the widest width of the brainstem. The isocenter for the SP ganglion was placed at the center of the contoured SP ganglion, ensuring that the 50% isodose line encompassed the widest extent of the contoured ganglion. Ninety Gy was prescribed to the isocentre for the trigeminal nerve and 80 Gy was prescribed to the isocenter for the SP ganglion (Figure 2).
An image of the treatment plan showing the contoured trigeminal nerve (orange) and sphenopalatine ganglion (red) and placement of the isocenter (+) and the 50% isodose line. Brainstem is contoured green.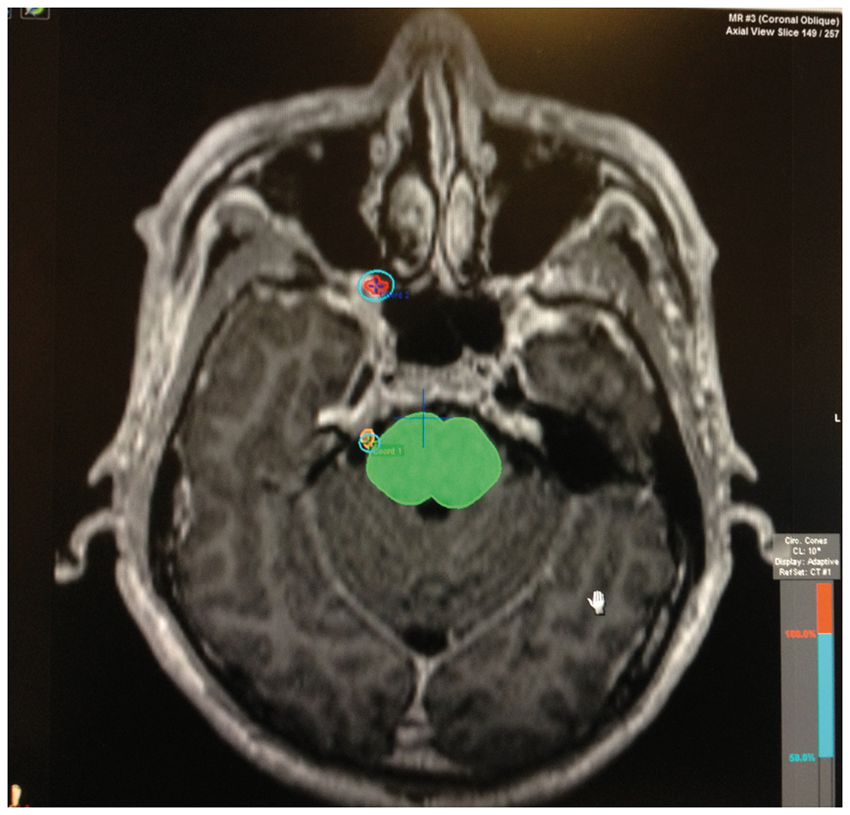
Treatment to the trigeminal REZ was delivered using eight dynamic conformal arcs with a 4 mm cone with a range of 120 degrees with avoidance of sensitive structures like the eye, optic nerve and chiasm. Treatment to the SP ganglion was delivered using seven dynamic conformal arcs with a 7.5 mm cone. Target localization was confirmed using the Exactrac system before commencing treatment and before every couch angle change. Total treatment time was about 37 minutes for the TN and 23 minutes for the SP ganglion.
Results
The follow-up length of our patient is 16 months to date. At one-week post-treatment, she reported a 60% reduction of pain, was off all medications at four months and at six months’ post-treatment she experienced only a slight pain, with a score of one to two out of 10. It was episodic and milder in nature and she had no tearing symptoms. There was also no facial numbness. Her pain continued to improve and at her last follow-up, she was completely pain free without any medications.
Discussion
The SUNCT syndrome was described as early as 1978 in a paper by Sjaastad et al. (1,10) and has been subsequently updated with more cases and reviews by the same and other authors (1,11). In 2004, SUNCT syndrome was included in the second edition of the International Classification of Headache Disorders (ICHD-2) (12). The diagnostic criteria for SUNCT specifies that the pain attacks last between five and 240 seconds and occur from three to 200 times per day, with the patient experiencing at least 20 attacks of such a nature. In the case of our patient, her symptoms were first thought to be cluster headaches, and oxygen therapy was instituted with no effect. As the pain evolved, a trial of indomethacin was given as for paroxysmal hemicrania but that did not respond either. Eventually, it appeared that the pain ‘maintained’ its characteristics of an SUNCT syndrome and was partially relieved by gabapentin and carbamazepine, which she eventually could not tolerate because of the side effects. It must be said that SUNCT has a male preponderance so this makes her a rare female patient. Before radiosurgery, she was adequately counseled concerning her treatment options based on available reports in the literature, their attendant risks and possible outcomes. She opted for frameless SRS for its non-invasive nature and was fully cognizant about the risk of facial numbness and potential radiation effects.
Regarding the mechanism of SUNCT pain, the posterior hypothalamus has been postulated to be a central trigger based on its increased activity on functional imaging during SUNCT attacks (13). Other sites in the brain have also shown increased activity during attacks such as the brainstem (14) and trigeminocervical complex (15), suggesting that there may be a link between these areas. SUNCT has been reported to be precipitated by trauma (11), associated with high levels of prolactin (16) and attributed to a meningioma in one case (17), suggesting a complex underlying etiology with both a central and peripheral component.
Initial attempts at treatment of the trigeminal nerve at the root entry zone by GK radiosurgery or by surgical intervention resulted in side effects and few benefits (4). In the report by Black and Dodick in 2002, the first of the two patients described was treated by glycerol rhizotomy, GK radiosurgery and microvascular decompression of the trigeminal nerve. The second patient was treated by GK radiosurgery and two microvascular decompression surgeries.
The side effects after these procedures for the first patient were anesthesia dolorosa, and the second patient experienced unilateral deafness, chronic vertigo and disequilibrium. Neither patient improved despite undergoing these neural destructive procedures. The suggestion then was that SUNCT syndrome arose from a central location and did not benefit from intervention of the peripheral portion of the trigeminal nerve. This was substantiated by a case that was successfully treated by deep brain simulation in 2005 (18). An electrode was implanted and continuous stimulation was directed to the posterior inferior hypothalamus. Adjustment was required on 12 occasions as the pain recurred, and the pain attacks subsided after lamotrigine was added. It was then suggested that long-term hypothalamic stimulation had modified circuits involving the hypothalamus that are implicated both in the pathophysiology of SUNCT and the mechanism of action of lamotrigine. In 2007 the same authors reported their experience of treating chronic trigeminal autonomic cephalalgia and atypical facial pains with deep brain stimulation of the posterior hypothalamus (19) in a series of 20 patients. One patient with SUNCT was reported to have benefited from the treatment.
In 2011, a report of a case of SUNCT successfully treated by GK with irradiation of both the trigeminal nerve and SP ganglion was published. A dose of 80 Gy was delivered to both structures and the patient remained pain free 39 months after treatment (5). A second similar case was reported in 2012 whereby a 50-year-old man with SUNCT refractory to medications received GK treatment (6). He was also given 80 Gy to the trigeminal nerve and the SP ganglion. At four months’ follow-up he had no more spontaneous attacks and only very occasional brief episodes of pain precipitated by touching. Together with our case, these three cases demonstrate the efficacy of treating peripheral targets in the management of SUNCT. However, unlike the intial GK experience, these authors postulate that the addition of the SP ganglion may be important for the favorable outcome in their patients because of its function in autonomic relay, but did not go into further mechanistic details. We postulate that the addition of the SP ganglion in combination with the trigeminal REZ as a target might have been important for complete pain relief because efferent parasympathetic outflow from it may be involved in further pain generation through the activation of trigeminovascular sensory afferents (20). Thus by ablating both targets, one might achieve peripheral blockade of all possible pain pathways, providing effective pain relief for the patient. These cases have also demonstrated that both targets can be treated safely with minimal side effects for the patient. The pathophysiology of trigeminal autonomic cephalalgias are certainly complex and they may indeed have a central mechanistic trigger. However, the success of these cases demonstrates that intervention at peripheral pathways might also be effective provided all the putative pathways are treated.
Our patient was treated with a linac-based radiosurgery system using the Novalis Classic machine and the frameless technique. This avoided any invasive procedures, and the simulation scans, treatment planning and radiosurgery delivery were spaced out over several days. This is unlike GK radiosurgery, whereby the patient has an invasive headframe attached to his skull for the entire day while the MRI scan and planning process are being performed. Our patient was able to leave after mask-making and simulation scans and returned for treatment on a separate day as an outpatient. Our patient has been followed up for more than a year but a longer follow-up will be necessary to determine the long-lasting effect of such an approach. If she remains pain free on longer follow-up, frameless SRS may prove to be, because of its added convenience, a very attractive treatment option for the unfortunate patient who suffers from medically refractory SUNCT.
Conclusion
SUNCT is a rare but debilitating cephalalgia that is difficult to control. After failed medical therapy, options include nerve blockades, deep brain stimulation, microvascular surgery or neuro-destructive procedures. Up to now, to the best of our knowledge, these options are all invasive to various degrees. We present the first reported case to be treated using non-invasive frameless SRS with the Novalis Brainlab system. Initial response to treatment has been excellent with minimal side effects. Longer follow-up and further experience with frameless SRS will determine the efficacy and safety of this option.
Clinical implications
Short-lasting unilateral neuralgiform headache associated with conjunctival injection and tearing (SUNCT) is a rare headache syndrome characterized by sudden brief attacks of severe unilateral head pain in the orbital, periorbital or temporal regions, accompanied by conjunctival injection and lacrimation. We report the first case in the literature of successful treatment with a non-invasive frameless stereotactic radiosurgery (SRS) technique targeting the trigeminal nerve and the sphenopalatine ganglion. Together with the two reported cases treated with radiosurgery on these two peripheral targets, there are now three cases of medically refractory SUNCT in the literature treated successfully with this modality with minimal toxicity, demonstrating that these two targets might need to be treated together for effective symptom control. We suggest that frameless SRS to the trigeminal nerve and sphenopalatine ganglion is an extremely convenient and attractive non-invasive option for patients with medically refractory SUNCT.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.