
Abstract
Background
Hemicrania continua (HC) and paroxysmal hemicrania (PH) belong to a group of primary headache disorders called trigeminal autonomic cephalalgias. One of the diagnostic criteria for both HC and PH is the absolute response to the therapeutic dose of indomethacin. However, indomethacin is discontinued in many patients as a result of intolerance to its side effects. Melatonin, a pineal hormone, which shares similar chemical structure to indomethacin, has been reported to have some efficacy for HC in previous case reports and series. To our knowledge, there is no literature regarding the use of melatonin in PH. We aimed to describe the clinical use of melatonin in the preventive management of HC and PH.
Methods
Patient level data were extracted as an audit from routinely collected clinical records in consecutive patients seen in outpatient neurology clinic at King’s College Hospital, London, UK, from September 2014 to April 2023. Our cohort of patients were identified through a search using the keywords: hemicrania continua, paroxysmal hemicrania, melatonin and indomethacin. Descriptive statistics including absolute and relative frequencies, mean ± SD, median and interquartile range (IQR) were used.
Results
Fifty-six HC patients were included with a mean ± SD age of 52 ± 16 years; 43 of 56 (77%) patients were female. Melatonin was taken by 23 (41%) patients. Of these 23 patients, 19 (83%) stopped indomethacin because of different side effects. The doses of melatonin used ranged from 0.5 mg to 21 mg, with a median dose of 10 mg (IQR = 6–13 mg). Fourteen (61%) patients reported positive relief for headache, whereas the remaining nine (39%) patients reported no headache preventive effect. None of the patients reported that they were completely pain free. Two patients continued indomethacin and melatonin concurrently for better symptom relief. Eight patients continued melatonin as the single preventive treatment. Side effects from melatonin were rare. Twenty-two PH patients were included with mean ± SD age of 50 ± 17 years; 17 of 22 (77%) patients were female. Melatonin was given to six (27%) patients. The median dose of melatonin used was 8 mg (IQR = 6–10 mg). Three (50%) patients responded to melatonin treatment. One of them used melatonin as adjunctive treatment with indomethacin.
Conclusions
Melatonin showed some efficacy in the treatment of HC and PH with a well-tolerated side effect profile. It does not have the same absolute responsiveness as indomethacin, at the doses used, although it does offer a well-tolerated option that can have significant ameliorating effects in a substantial cohort of patients.
Introduction
Hemicrania continua (HC) and paroxysmal hemicrania (PH) are primary headache disorders belonging to the trigeminal autonomic cephalalgias (1). HC and PH clearly differ from each other by the duration of pain, although both completely respond to a therapeutic dose of indomethacin (2,3). HC is characterized by the baseline background unilateral headache with intermittent exacerbations and ipsilateral cranial autonomic features. PH was first described by Sjaastad and Dale (4) as a new, treatable disorder, whereas hemicrania continua was defined by Sjaastad and Spierings (5), after an earlier mention of a phenotype incorrectly labeled as cluster headache (6). The incidence of HC in the general population is largely unknown. More than 1000 cases have been published so far in the literature (7), although not all are clearly indomethacin responsive. By contrast to HC, PH is characterized as severe unilateral pain lasting up to 30 minutes, which occurs more than five times per day together with ipsilateral cranial autonomic symptoms (2,8). The estimated one-year prevalence of PH is 0.5 per 1000 or less (9,10).
According to the International Classification of Headache Disorders, 3rd edition (ICHD-3), HC is defined as unilateral headache that persists for more than three months, with at least one of the ipsilateral autonomic symptoms including conjunctival injection, lacrimation, nasal congestion, rhinorrhea, eyelid oedema, facial sweating, miosis or ptosis and a therapeutic response to indomethacin (1). A recent review suggested the three most common symptoms associated with HC were lacrimation, conjunctival injection and restlessness or agitation (11). PH is defined as severe unilateral headache lasting for 2–30 minutes with ipsilateral autonomic features. The frequency of attacks should be up to five times per day (1).
The region of the posterior hypothalamus and dorsal rostral pons play a key role in the pathophysiology of HC and PH (12). It is hypothesized that the presence of cranial autonomic symptoms in trigeminal autonomic cephalalgias is partly a result of the hypothalamic activation with secondary disinhibition of the trigeminal autonomic reflex (12). Significant activation of contralateral hypothalamus and ipsilateral rostral pons during baseline pain of HC has been shown in a previous functional imaging study (13).
The mainstay of treatment for HC is currently indomethacin. However, some patients cannot continue on indomethacin as a result of their intolerance to its side effects. Melatonin, a pineal hormone sharing a similar chemical structure to indomethacin, has been reported to have some efficacy for HC in previous case reports and series (14,15). Indomethacin and melatonin share an indole structure (Figure 1), which may confer similar clinical effect to HC or PH patients (16). Up to two-thirds of PH patients eventually stop indomethacin because of its side effects despite the high efficacy of indomethacin (2). Other alternative treatments that have been suggested include other non-steroidal anti-inflammatory drugs and cyclooxygenase-2 inhibitors (17). By contrast to HC, to our knowledge, there is no literature regarding the use of melatonin in PH. Considering that PH and HC are likely different presentations of a similar condition, it is reasonable to consider melatonin in the preventive treatment of PH.

Chemical structure of melatonin and indomethacin.
Melatonin is a prescription medicine in the UK and it is not available over the counter without a doctor’s prescription. All the melatonin prescribed for headache disorders is directly supplied by the hospital pharmacy to the patients.
We aimed to describe the clinical use of melatonin in patients of HC and PH as an alternative or adjunctive preventive treatment.
Methods
Patient level data extracted as an audit from routinely collected clinical records in consecutive patients seen in outpatient neurology clinic at King’s College Hospital, London, UK, from September 2014 to April 2023. Audit in the UK does not require ethical approval. Our cohort of patients were identified through a search of the following keywords: hemicrania continua, paroxysmal hemicrania, melatonin and indomethacin. Clinical notes from all identified cases were carefully reviewed to confirm the presence of HC or PH and to collect clinical data systematically. All patients were diagnosed with HC or PH according to the ICHD-3 (1). Patients who were ever prescribed with melatonin were included. The formulation of melatonin used was a 2-mg sustained release tablet in this cohort. All the patients were advised to take melatonin two hours before sleep. Melatonin was prescribed at the discretion of the treating neurologist and the dose of melatonin was titrated as tolerated. Indomethacin could be either continued concurrently with melatonin or stopped. The effect of melatonin was assessed by the treating clinicians regarding the reduction of the frequency of headache exacerbation days, reduction of the severity of pain and/or increase in the headache-free period. Positive response was determined during each clinical visit as overall improvement based on these clinical assessments.
This cohort of patients has not been not reported in previous studies.
Descriptive statistics including absolute and relative frequencies, mean ± SD, median and interquartile range (IQR) were used for the results of this cohort.
Results
Hemicrania continua
Fifty-six patients who were diagnosed with HC were reviewed. Melatonin was prescribed in 23. Their mean ± SD age was 52 ± 16 years and 19 of 23 (83%) patients were female.
Fifteen (65%) patients had a positive intramuscular indomethacin test, whereas the remaining eight (35%) showed a positive response to an oral indomethacin trial. The equivalent daily dose of indomethacin was in the range 75–225 mg. Of 23 patients, 19 (83%) stopped indomethacin because of different side effects. Commonly reported side effects of indomethacin included nausea, vomiting, oral ulcer and abdominal pain (Table 1).
Side effects of indomethacin reported in HC (n = 23) and PH (n = 22) patients.
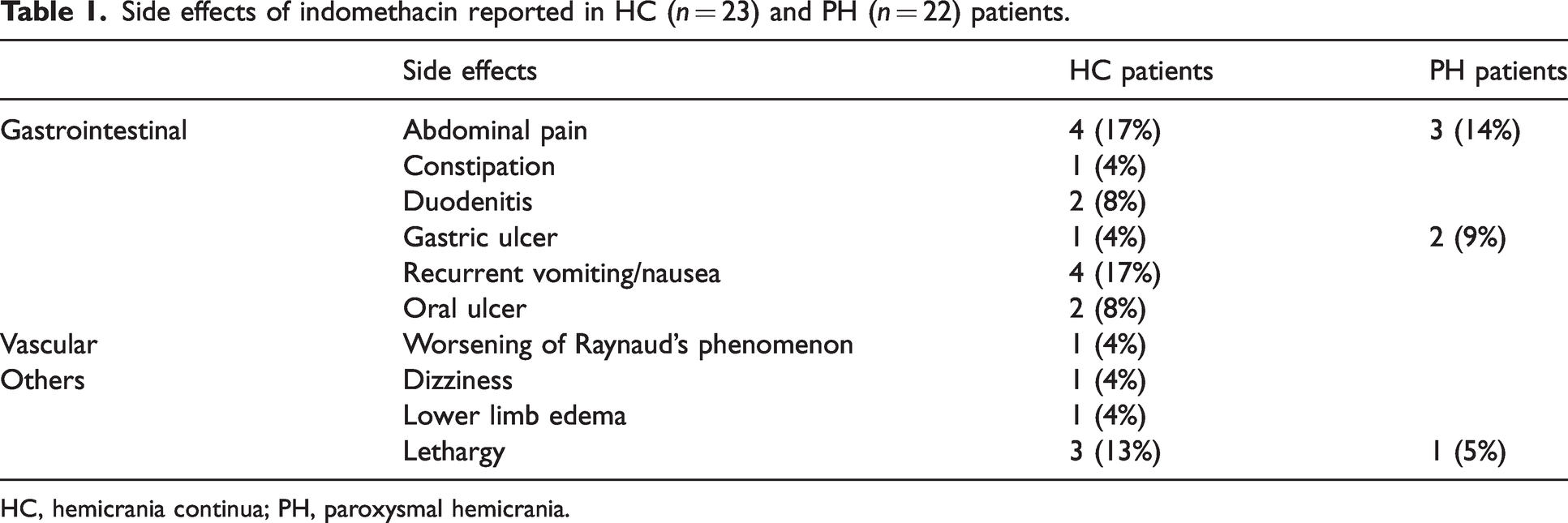
HC, hemicrania continua; PH, paroxysmal hemicrania.
Melatonin
Melatonin was taken once daily at night among these patients. The maximum dose reached of melatonin was in the range 0.5–21 mg. The median dose of melatonin was 10 mg (IQR = 6–13 mg). Patient reported clinical response during their first follow up in the time frame of six months. Fourteen out of 23 (61%) patients reported some positive relief for headache when on melatonin from 6 mg to 14 mg. The median dose for positive response was 9 mg (IQR = 6–12 mg). Nine out of 23 (39%) patients reported no headache preventive effect with doses from 0.5 mg to 21 mg. The median dose for those without a response was 10 mg (IQR = 6.5–20 mg) (Figure 2).

Melatonin in hemicrania continua.
None of the patients reported they were completely pain free with melatonin treatment. Two patients continued on indomethacin and melatonin concurrently for better symptom relief. Eight patients stopped indomethacin because of intolerance and continued on melatonin as the single preventive treatment. Side effects from melatonin were rare. One patient reported fatigue and one patient reported sleepiness after the use of melatonin. Two patients reported worsening of headache after taking melatonin and one patient stopped it because of pregnancy plan.
All HC patients experienced cranial autonomic symptoms including lacrimation, nasal congestion, conjunctival injection, facial flushing, ptosis and eyelid edema. The median number of cranial autonomic symptoms among HC patients was three.
Among HC patients taken melatonin, 20 out of 23 (87%) patients reported at least one migrainous feature: photophobia, phonophobia, osmophobia and cranial allodynia. The median number of reported features was two. Associated nausea was reported in 15 (65%) patients, whereas vertigo was present in 12 (52%) patients.
Paroxysmal hemicrania
Twenty-two patients with PH were included in this study. The mean (± SD) age at diagnosis was 50 ± 17 years and 17 of 22 (77%) were female. Most had chronic PH (n = 20; 91%) and four patients had a circannual pattern. More than half had an additional migraine diagnosis (n = 14; 64%): eight episodic and six chronic migraine. The median follow-up was 3.6 years (IQR = 1–7 years) and most patients had two or three clinical records. Six patients had a positive intramuscular indomethacin test, whereas the remaining 16 patients showed positive response to oral indomethacin. In six patients (6 of 22; 27.3%), indomethacin had to be discontinued because of adverse events (Table 1).
Melatonin
Six patients were given melatonin (median of 8 mg, IQR = 6–10 mg) of whom three found it helpful in reducing the frequency of headache at doses of 6, 8 and 15 mg, respectively. The three patients responded to melatonin were women with chronic PH (Figure 3).

Melatonin in paroxysmal hemicrania.
Case one was a 74-year-old woman that started to experience a new type of headache at 70 years old, being diagnosed two years later with PH. She had no history of migraine and had a diagnosis of multiple sclerosis since her forties. She was doing well on oral indomethacin (200 mg daily), stopping it because of gastrointestinal intolerance. Greater occipital nerve block (GON) and non-invasive vagus nerve stimulation were not effective. She was started on melatonin up to 15 mg. There was no change on the headache frequency, but she had less agitation during the episodes and the attacks were significantly less intense.
Case two was a 48-year-old woman with no history of migraine who was diagnosed with chronic PH at the age of 38 years. She was stable on indomethacin 225 mg daily but, after 24 months, her headaches worsened and she did not tolerate any further increase of indomethacin. She was started on melatonin up to 8 mg. At three-month follow-up, she was headache free.
Case three was a 57-year-old woman with history of episodic migraine since her twenties. She was diagnosed with chronic PH at the age of 53 years. She did not tolerate oral indomethacin. Previous ineffective treatments included lamotrigine, topiramate and GON injections. Treatment with melatonin up to 6 mg was very helpful with respect to suppressing the nocturnal attacks and decreasing the daily attacks.
Discussion
One of the crucial features of HC and PH is the absolute responsiveness to indomethacin. Unfortunately, most patients experience different side effects of indomethacin and, in many, this leads to its discontinuation. Gastrointestinal side effects are commonly reported (18). Long-term use of indomethacin may also result in renal toxicity. Alternative treatment is certainly needed. Clinical reviews have suggested options including cyclooxygenase-2 inhibitors, gabapentin, topiramate, non-invasive vagus nerve stimulation and melatonin (18,19). The evidence to support the use of these alternative options is limited and somewhat anecdotal. Melatonin is one of the commonly used options given its good safety profile and biologically plausible mechanisms of action.
There are several proposed mechanisms of melatonin in headache disorders. First, melatonin exerts its impact on the hypothalamus, which plays a role in the pathophysiology of hemicrania continua and paroxysmal hemicrania. Previous studies have shown that there are melatonin receptors (MT1 and MT2) in the suprachiasmatic nucleus of the hypothalamus and the use of exogenous melatonin can possibly exert beneficial effects through these receptors (20,21). Secondly, melatonin improves sleep, which is well known to play an important role in headache disorders. The circadian rhythm of humans being is closely related to melatonin, which is secreted by the pineal gland at night (22). The administration of melatonin can regulate the circadian clock and potentially be helpful for HC and PH. Therefore, patients are advised to take melatonin before sleep to match the endogenous circadian rhythm. Moreover, it has been demonstrated that melatonin has anti-inflammatory as a free-radical scavenger and anti-nociceptive properties, which result in the attenuation of the pain associated with inflammation (23). In addition, melatonin and indomethacin share a similar chemical structure because a methoxy indole nucleus is present in both of them (22).
In this cohort, melatonin showed positive effects in most HC patients and some PH patients. The median dose of melatonin used in HC was 10 mg and there was further room for up-titration in case the symptom control of HC was not satisfactory. The side effect profile of melatonin was modest in this cohort of patients and no serious adverse effects were reported.
Although melatonin was safe in terms of side effects, most patients could not achieve complete pain relief when using melatonin alone as the preventive treatment. As such, melatonin can be considered to be used concurrently with indomethacin and the dose of indomethacin can be titrated to the lowest possible dose to minimize its side effects. Melatonin has been shown to provide some protective effects against peptic ulcer so that the adjunctive use of melatonin may ameliorate the gastrointestinal side effects of indomethacin (24).
Apart from the constant unilateral headache and autonomic symptoms, features of migraine are commonly seen in HC and PH patients. Symptoms including nausea, vomiting, photophobia, and phonophobia are reported (2,3,8,11). In this cohort, most of the patients reported some migrainous features as well. Melatonin has been investigated (25) and used as the preventive treatment for migraine (26,27) and effective clinical responses have been reported. Whether the use of melatonin in HC and PH arises from an effect on migrainous biology remains an unanswered question.
Limitations
The treatment response of melatonin was largely determined clinically by the treating neurologist and more objective measures, such as diary data, would be useful going forward. The doses and duration of melatonin used was primarily titrated by the treating clinicians according to the tolerance and response without pre-defined escalation regimen. This limits general utility. Patients with negative response might benefit for longer duration or higher tolerated dose of melatonin use. Lastly, the data are open label and suggest that a placebo-controlled trial is warranted.
Conclusions
Melatonin showed some efficacy in the treatment of HC and PH with a well-tolerated side effect profile. It does not have the same absolute responsiveness as indomethacin at the doses used, although it does offer a well-tolerated option that can have significant ameliorating effects in a substantial cohort of patients.
Clinical implications
Indomethacin is discontinued in many HC or PH patients as a result of intolerance to its side effects. Melatonin offers a well-tolerated option with significant ameliorating effects in this cohort of HC and PH patients. Melatonin can be considered as an add-on therapy in the treatment of indomethacin-sensitive headache with a starting dose of 2 mg before sleep with gradual dose titration as tolerated.