
Abstract
Introduction
After decades of research, the importance of psychological factors in child and adolescent headache is no longer in doubt. However, it is not clearly understood whether different types of headache are comorbid with specific kinds of psychopathology. To address this issue, we set out to establish whether young patients with migraine do or do not show significant levels of psychopathological symptoms compared with age-matched healthy controls and patients with tension-type headache (TTH).
Methods
Ten studies were selected on the basis of a widely used psychodiagnostic tool (the Child Behavior Checklist (CBCL)) and by applying rigorous criteria: The studies were compared in a meta-analysis in order to evaluate the presence of Internalizing (mainly anxiety and depression) and Externalizing (mainly behavioral problems) symptoms in different types of headache (and versus healthy controls).
Findings
Patients with migraine showed more psychopathological symptoms than healthy controls. TTH patients also had more psychopathology than controls, although the difference was more marked in the area of Internalizing disorders. Finally, no differences emerged between migraine and TTH.
Discussion and conclusion
Psychopathological symptoms affect children with migraine, but also children with TTH. Biological, pathophysiological and clinical links need to be established. Effective treatment of affected children and adolescents is imperative in order to prevent chronic evolution. In this context, the CBCL may be a good screening instrument with a view to developing a tailored clinical approach.
Introduction
Study of the psychological characteristics of migrainous children dates back half a century. In 1955, Vahlquist (1) identified neurovegetative instability, ambition and perfectionism, and anxiety in these children, and Bille (2) described them as more anxious, sensitive, deliberate, cautious, fearful, vulnerable to frustration, tidy and less physically enduring than control group children. A few years later, Koch and Melchior (3) found signs of nervousness, mental instability and immaturity in migraineurs and non-migraineurs from a pediatric university clinic. They suggested that these children displayed “a decreased resistance to psychological stress and conflict situations, rather than overt psychological disorder, or endogenous disease.” Maratos and Wilkinson (4), more than a decade later, found higher rates of anxiety and depression associated with “disturbed parental relationships” in children with migraine; an emotional upset was the most frequently reported headache trigger in this study. Subsequently, Guidetti et al. (5) identified the presence of feelings of exclusion from the family group and repressed hostility toward important figures in children with migraine, while Lanzi et al. (6,7) observed a neurotic, borderline personality organization or “white relation” in juvenile migraine and chronic tension-type headache (TTH) sufferers. Cahill and Cannon (8), in a population-based study, concluded that “migraine should be a headache subtype of particular interest for psychiatrists” given the significant association between stress, personality traits, psychiatric disorders and migraine.
Meta-analysis of CBCL scores (CBCLi, Internalizing scale scores; CBCLe, Externalizing scale scores) in studies comparing patients affected by migraine and healthy controls. Random-effect models were applied (test for heterogeneity Q = 36.66, p = 0.001, I2 = 59.09). The migraine patients showed significantly higher CBCL scores (CBCL Total, Hedge’s g = 0.562, p < 0.001) on both the Internalizing (CBCLi, Hedge’s g = 0.778, p > 0.001) and Externalizing (CBCLe, Hedge’s g = 0.349, p < 0.001) scales than healthy subjects.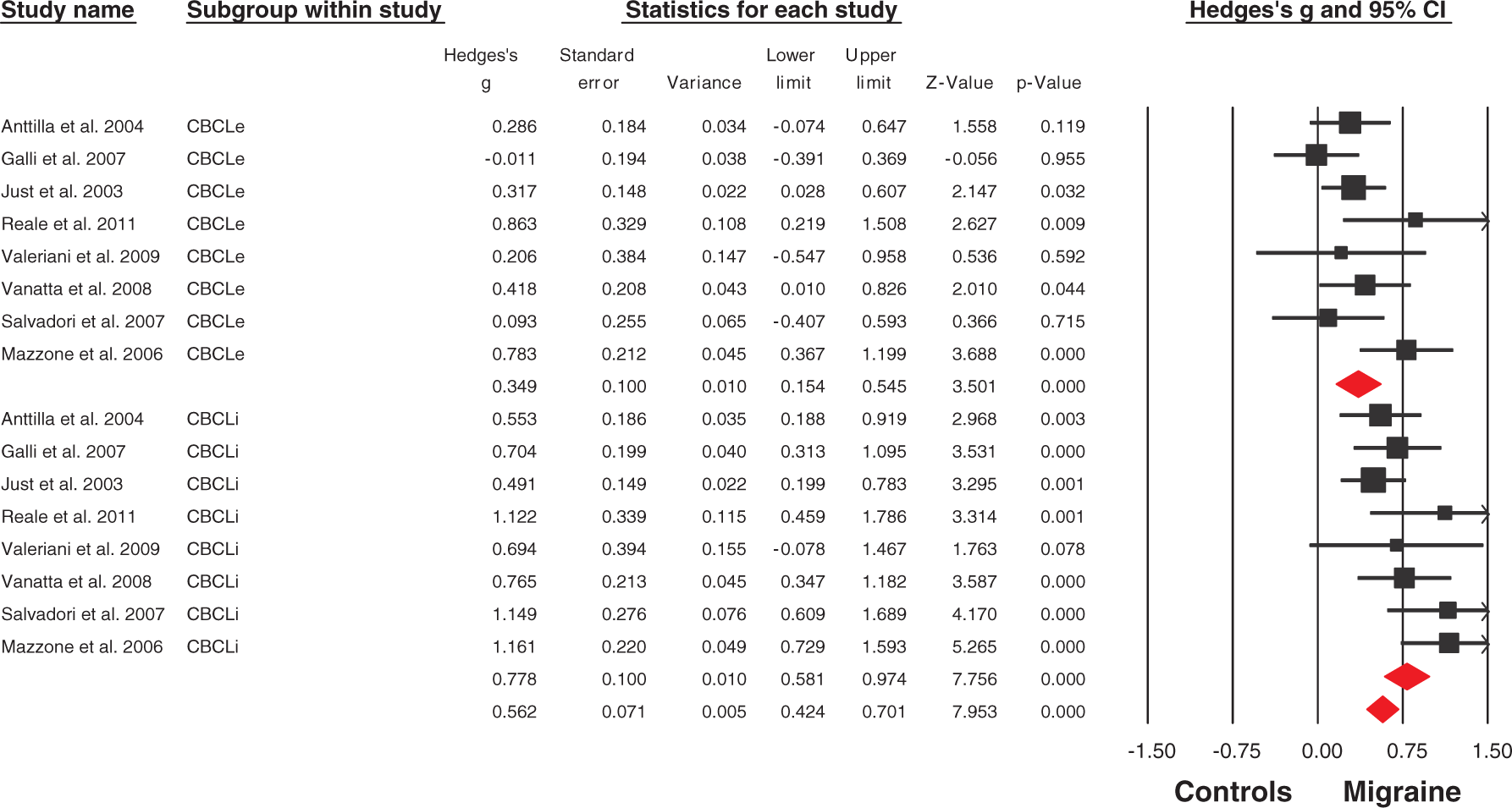
Although, on the basis of current knowledge on this topic, psychological factors seem to play an important role in headache, much remains to be understood. At the start of the 1990s, the concept of psychiatric comorbidity was introduced into the headache field (9); this was a key development as it gave the scientific community a common language to use in its approach to this complex issue. The term psychiatric comorbidity has been used to indicate the possible, unexplained but not casual, relationship between migraine and psychiatric disorders (10). Over the years, various studies have addressed this topic, both in adults and in children and adolescents, raising questions that remain unanswered today. For example, we still do not know the nature and direction of the relationship between migraine and comorbid psychiatric disorders (mainly anxiety and depression), whether the relationship is specific to migraine or related to attack frequency, or whether there exists an intrinsic and specific relationship between psychological factors and migraine (11). Another critical issue is that of the relationship between chronic pain and psychopathology (studied in adults and very little in children), because it has become increasingly evident that chronic medical conditions (not only headache, but also low back pain, pelvic pain, temporomandibular pain and fibromyalgia) are associated with higher rates of psychiatric disorders (mostly anxiety and mood disorders) (12,13). Hypotheses on the association between chronic pain and psychiatric disorders have been advanced (14), but definitive answers are still lacking.
Meta-analysis of CBCL scores (CBCLi, Internalizing scale scores; CBCLe, Externalizing scale scores) in studies comparing tension-type headache (TTH) and healthy controls. Random models were applied (test for heterogeneity Q = 546.15, p = 0.001, I2 = 97.99). The TTH patients showed significantly higher CBCL scores (CBCL Total, Hedge’s g = 1.572, p = 0.002). This result was mainly driven by significant differences on the Internalizing (CBCLi, Hedge’s g = 2.344, p = 0.009) rather than the externalizing (CBCLe, Hedge’s g = 1.207, p = 0.051) scale.
Most previous studies on psychiatric comorbidity in headache considered migraine, and less frequently, TTH. The first edition of International Classification of Headache Disorders (ICHD-I) (15) recorded psychosocial stress, anxiety and depression as potential “causes” of TTH, but contained no indications regarding migraine. The second edition of the ICHD (ICHD-II) made no reference at all to “psychological causes” in relation to either migraine or TTH, but did add, in the Appendix, the new category of “Headache attributed to psychiatric disorder”; this note, however, fails to provide any indication about the clinical characteristics of this form (16). Consequently, further studies are needed to evaluate the suitability of this diagnostic category both for adults and (especially) for children and adolescents.
Meta-analysis of CBCL scores (CBCLi, Internalizing scale scores; CBCLe, Externalizing scale scores) in studies comparing patients with migraine and patients with tension-type headache (TTH). Random models were applied (test for heterogeneity Q = 29.893, p = 0.002, I2 = 63.02). There were no significant between-groups differences in the CBCL Total score (Hedge’s g = 0.042, p = 0.730), or in the Internalizing (CBCLi, Hedge’s g = 0.009, p = 0.954) or Externalizing (Hedge’s g = 0.083, p = 0.649) scale scores.
Although most of the studies that have addressed these issues assessed the role of psychopathological factors in children affected by migraine, as mentioned above, it remains to be established whether these factors are specific to migraine or simply more studied in migraine than in (episodic or chronic) TTH patients. A recent review on this topic (17) even questioned the existence of psychological difficulties in children with migraine, concluding that children with migraine in a clinical setting “do not exhibit more psychological dysfunctioning and (to a lesser extent) do not exhibit more psychiatric comorbidity compared with healthy controls.” Moreover, we do not know whether (18) or not (19) psychosocial factors properly discriminate between migraine without aura and (frequent) episodic TTH.
To address these contrasting findings, we conducted a quantitative meta-analysis of studies that have investigated psychopathological symptoms in children with headache. Our main aim was to evaluate whether migraine patients do or do not show significant levels of psychopathological disorders compared with age- and sex-matched healthy controls and TTH subjects. The fact that the psychological functioning of children and/or adolescents is assessed, in available studies, using different diagnostic tools sometimes precludes comparison of their findings. Furthermore, differences and similarities between the psychological functioning of migraine and TTH patients have not been sufficiently explored in the literature. Shedding new light on this issue might have neurobiological implications and prompt new lines of research.
One existing line of study suggests that migraine (20–23) and anxiety and mood disorders (24,25) may be underpinned by a common biological milieu and by shared neurotransmitter system involvement (mainly serotonin and dopamine), although the exact mechanisms involved remain to be evaluated. The possibility of neurotransmitter system involvement has also been considered in relation to chronic daily headache (CDH), and it has been found to be associated with a higher rate of comorbid psychiatric disorders than other headache subtypes. Genes implicated in the regulation of dopamine metabolism have been hypothesized to be candidate genes for CDH (26). Finally, efforts to understand migraine from the neurobiological perspective are further complicated by the suggestion that there may be no differences, from the psychological point of view, between headache subtypes (27,28).
Methods
Selection procedures
Search strategies
A systematic search strategy was used to identify relevant studies. First, we carried out a PubMed, Science Direct, Scopus and PsycInfo search, looking for studies conducted in juvenile subjects affected by headache (see below). We used the following search terms: “headache,” “migraine”, “tension-type headache,” “chronic daily headache,” “child,” “adolescent,” “pediatric,” “psychopathology,” “psychiatric disorder,” “psychiatric comorbidity,” “psychological,” “psychological disorder,” “anxiety,” “depression,” “internalizing disorder,” “externalizing disorder,” and “behavioral disorder.” In a second step, the reference lists of the articles identified and selected for the review were manually checked for relevant studies not identified by the computerized literature search. Third, we selected a group of candidate studies for the meta-analysis on the basis of the following criteria: comparability (i.e. use of the same international criteria to classify headache and the same test to evaluate psychological functioning), presence of control group(s), sufficient sample size, and sufficient data reporting. Clinical as well as population studies could be included in the meta-analysis. Finally, we contacted the corresponding authors of these articles by e-mail requesting any details not given in the original manuscripts.
Child Behavior Checklist (CBCL)
The CBCL, first developed by Thomas M. Achenbach (29), has become, over time, one of the most widely used standardized and validated measures in child psychiatry. Translated into 75 languages and used in more than 6000 published papers worldwide, the CBCL is a parent-rating scale used to assess competences, emotional and behavioral problems in children and adolescents aged 4–18 years; it is an easy-to-administer measure that takes about 20–30 minutes to complete. The questionnaire consists of two parts: “Competences” and “Emotional and Behavioral Problems.” With regard to the latter, multivariate analyses have identified two main groupings of problems: “Internalizing scale” (anxious and inhibited behavior) and “Externalizing scale” (aggressive and antisocial behavior). The 118 items making up this second part (each scored from 0 to 2), variously grouped, are rated by parents as: “not true” (0), “somewhat true” (1) or “always or often true” (2). The items are grouped into eight narrow-band subscales: “Withdrawn,” “Somatic complaints,” “Anxious/depressed” (these first three subscales come under the “Internalizing scale”), “Delinquent behavior,” “Aggressive behavior” (under the “Externalizing scale”), “Thought problems,” “Social problems” and “Attention problems” (designated as neither “Externalizing” nor “Internalizing”). Thirty-three items that could not be assigned to any of these scales are grouped under “Other problems.” The “Total score,” an index of global psychological functioning, is obtained by summing all the items. The CBCL tends to be administered to the mother, as the parent who usually spends more time with the child. In this meta-analysis we considered the Internalizing scale score, the Externalizing scale score and the Total score, because they are the measures most representative of global psychological functioning.
Definition of headache groups
All but one of the studies selected used the same system for making the headache diagnoses (ICHD – first or second edition (15,16)). The remaining study (30) was included because the diagnostic criteria used made it possible, within the broad category of CDH, to distinguish between migraine and TTH.
Selection criteria
Studies were preliminarily included if they met the following criteria: (a) were reported in an original paper in a peer-reviewed journal, (b) had involved subjects affected by migraine, subjects with TTH or a matched control group, (c) had analyzed at least two of these groups using the CBCL, (d) had reported mean (SD) values for the CBCL Internalizing scale, Externalizing scale, and Total scores in both the groups considered, and e) had studied samples not overlapping with a previous sample.
Recorded variables
For each article included in the meta-analysis, the following variables were recorded: year of publication, sample size, age and gender of subjects, comorbidities, and drug and/or non-drug therapies. To ensure a high standard of reporting, we adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (31) and also the revised Quality of Reporting of Meta-analyses (QUOROM) statement (32).
Quality assessment
Although reliable quality assessments are possible in meta-analyses of experimental studies, their use in observational research is controversial, as there is, in this area, no clear consensus on rating methods or their appropriate use in meta-analysis (33). In the present meta-analysis, we used a simple objective rating system (based on the meta-analysis by Paulson and Bazemore published in the Journal of the American Medical Association (JAMA) (34)) whereby the quality of the studies was rated, on a scale of 0 to 10, through the assigning of a maximum of two points each for: (a) description of the sampling method; (b) presence of clearly stated inclusion criteria; (c) assessment of ethnic and (d) sociodemographic diversity; and (e) comprehensive description of the main outcome measure. Because evidence on the validity of quality ratings in observational research is lacking, we adopted the Meta-analysis of Observational Studies in Epidemiology (MOOSE) (35) approach of broadly including all studies and using sensitivity analysis to determine incremental effects of lower-quality studies.
Statistical analysis
Data were analyzed using Comprehensive Meta-Analysis Software, version 2 (Biostat, Inc., Englewood, NJ, USA). As a measure of effect size, the Hedges’ g was adopted, i.e. the difference between the CBCL means of the two groups, divided by the SD and weighted for sample size in order to correct for bias from small sample sizes (36). This metric is normally computed using the square root of the mean square error from the analysis of variance testing for differences between two groups, as indicated by the formula



In general, random-effects models are more conservative than fixed-effects models, and appear to better address heterogeneity between studies and study populations, allowing for greater flexibility in parsing effect size variability. Moreover, they are less influenced by extreme variations in sample size (37). Due to the heterogeneity of the studies included in this meta-analysis, random-effects models were used. Point estimates of between-study heterogeneity were assessed with the Q statistic, with magnitude of heterogeneity being evaluated with the I2 index (38). Studies with negative results are less likely to be published than studies with statistically significant results. The possibility of a publication bias in the present study was evaluated by visually inspecting funnel plots and applying the regression intercept of Egger et al. (39). In this way, we attempted to establish whether there was a tendency for selective publication of studies based on the nature and direction of their results. In addition, we used the fail-safe procedure (40) to generate the number of unpublished studies that would be needed to move estimates to a non-significant threshold. To assess the robustness of the results, we performed sensitivity analyses by sequentially removing each study and rerunning the analysis.
Results
Studies found
The combined search strategies yielded a total of 22 articles, of which nine did not meet the eligibility criteria. Of the 13 articles considered eligible, 10 (30,41–49), published between 1996 and 2011, met the criteria for inclusion in the present meta-analysis (Diagram 1). All 10 studies concerned clinical population, with the exception of one (43). The resulting database comprised, overall, 406 patients with migraine (mean age 11.6 ± 2.3 years, 51.16% females), 230 patients with TTH (mean age 12.3 ± 2.2 years, 55.5% females) and 488 controls (mean age 11.75 ± 2.35 years, 58.4% females), all well matched with respect to age, intelligence quotient (IQ) and gender (all p > 0.05) (see Table 1).
Search strategy used to find studies suitable for inclusion in the present meta-analysis. Overview of the studies included in the meta-analysis. ICHD-I: International Classification of Headache Disorders, edition 1; ICHD-II; International Classification of Headache Disorders, edition 2; SD: standard deviation.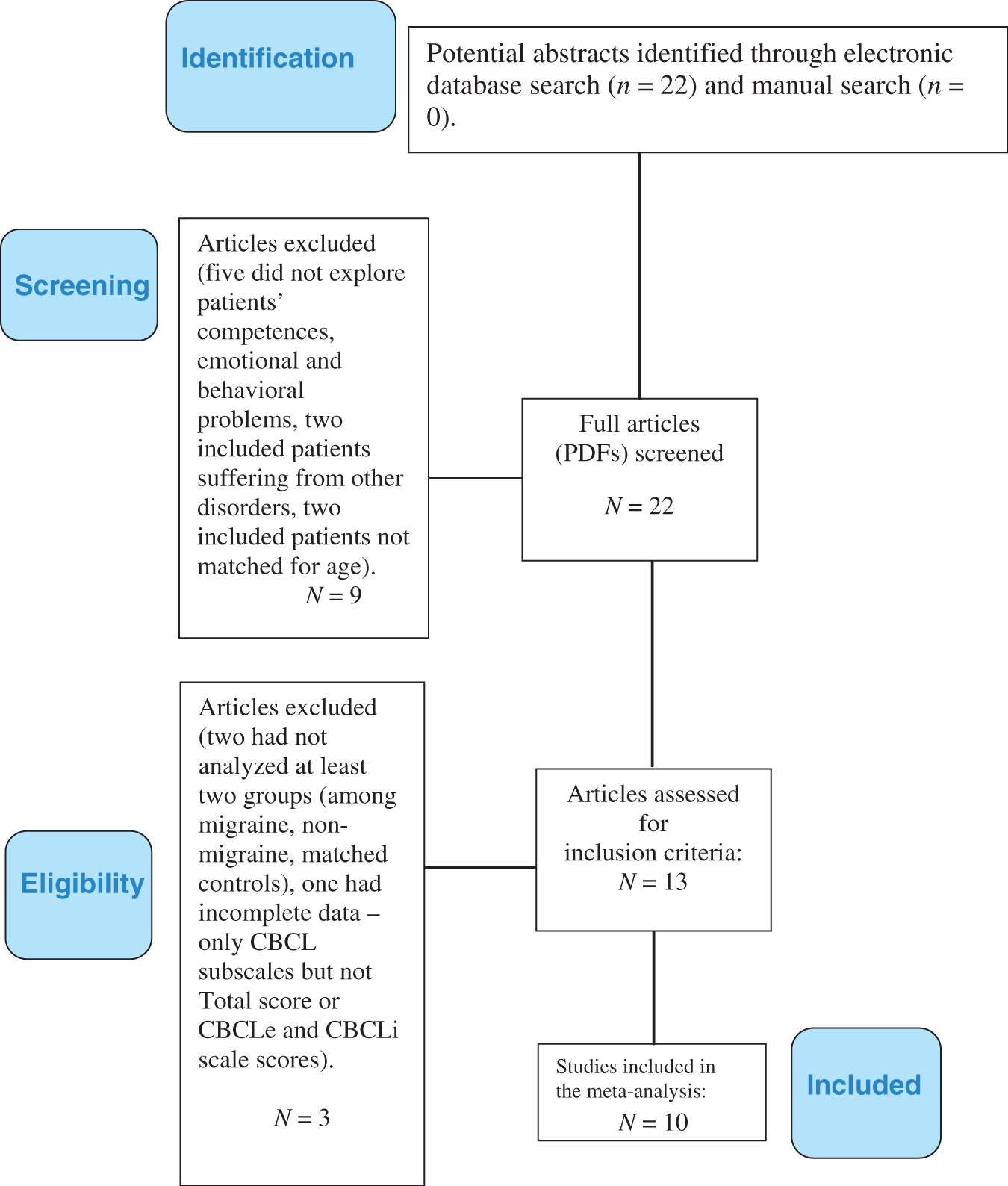

Migraine patients vs controls
Formal meta-analysis of CBCL scores (CBCLi, Internalizing scale score; CBCLe, Externalizing scale score, CBCL Total score) recorded in studies comparing patients affected by migraine and healthy controls revealed a moderate effect size toward higher Total scores (CBCL Total, Hedge’s g = 0.562, p < 0.001) in the patient group (test for heterogeneity Q = 36.66, p = 0.001, I2 = 59.09). The effect was more marked in the Internalizing than in the Externalizing scale (CBCLi, Hedge’s g = 0.778, p > 0.001; CBCLe, Hedge’s g = 0.349, p < 0.001).
TTH patients vs controls
Similarly, formal meta-analysis of CBCL scores recorded in studies comparing TTH patients and healthy controls revealed higher CBCL Total scores in the patient group (CBCL Total, Hedge’s g = 1.572, p = 0.002) with a strong effect size (Q = 546.15, p = 0.001, I2 = 97.99). However, this result was mainly driven by differences in the Internalizing (CBCLi, Hedge’s g = 2.344, p = 0.009) rather than the Externalizing (CBCLe, Hedge’s g = 1.207, p = 0.051) scale scores.
Migraine vs TTH patients
Finally, we directly compared TTH and migraine patients (test for heterogeneity Q = 29.893, p = 0.002, I2 = 63.02). There emerged no significant between-group differences in the CBCL Total score (Hedge’s g = 0.0042, p = 0.730), or in the Internalizing (CBCLi, Hedge’s g = 0.009, p = 0.954) and Externalizing (Hedge’s g = 0.083, p = 0.649) scale scores.
Tests for publication bias, heterogeneity, sensitivity analysis
Visual inspection of funnel plots revealed no evidence of publication bias. The quantitative evaluation of publication bias, as measured by the Egger intercept, was not significant (p = 0.132). The fail-safe procedure estimated that 15 unpublished studies would be needed to bring the overall meta-analytic estimate of transition rates to a non-significant level. Applying the criteria set by Higgins and Thompson (50), the heterogeneity in the published studies was found to be large in magnitude and statistically significant. Removing studies with poor quality ratings influenced the meta-analytic estimate by only 7%.
Discussion
To the best of our knowledge, this is the first meta-analysis on psychopathological functioning in children and adolescents affected by TTH and migraine. Applying rigorous inclusion criteria, we identified 10 studies on migraine and/or TTH suitable for inclusion in this meta-analysis. All were studies analyzing CBCL Total scores, Internalizing and Externalizing scale scores, and comparing migraine, TTH and healthy controls. The migraine patients were found to show more psychopathological symptoms (reflected both in Total scores and in internalizing/externalizing disorders) than the healthy controls. The TTH patients also had more psychopathology than the controls, although the difference was more marked in the area of internalizing disorders. Finally, no differences emerged between the migraine and TTH patients for any of the scales considered.
These findings highlight the critical role of psychopathological factors in migraine: not only internalizing symptoms, but externalizing ones, as well. While the role of anxiety and depression is well known in the literature (10), externalizing problems have been less frequently found to characterize migraine (51). In the TTH group we found a trend similar to that observed in the migraineurs, even though the weight of externalizing symptoms seemed to be less marked. However, comparison of the two headache subtypes failed to show a significant difference.
The presence of common psychopathological symptoms shared by migraine and TTH patients raises important questions from several perspectives – clinical, diagnostic, pathophysiological and therapeutic. It is, of course, not known whether some TTH patients will go on to develop migraine as well. Some authors argue in favor of a “continuum theory of headache syndromes” (27), hypothesizing the existence, in children, of a continuum between different headache subtypes having a shared neurobiological substrate. Furthermore, it can be very difficult to distinguish clearly between migraine and (episodic) TTH because of similarities in the clinical phenotypes, overlapping disease courses, and the frequent coexistence, in children, of migraine without aura and episodic TTH (28). Although we continue to think that there is probably little difference between migraine and TTH, there may nevertheless be other explanations for the shared psychiatric features in these conditions, and we should not necessarily think in terms of one disorder with different clinical characteristics. In our opinion, evidence from population-based studies shows that the occurrence of psychiatric disorders in headache patients cannot be interpreted as a bias related to clinical samples (the so-called Berkson’s bias): Anttila et al. (43), in a study of 1135 Finnish children, found a significant prevalence of family functioning difficulties, impaired social relationships and internalizing and global behavior disorders among primary headache patients. These findings are consistent with those obtained by Fearon and Hotopf in their study of 17,414 children (52). These authors concluded that headaches and migraine could be read as “signs of underlying psychosocial adversity.” Marmorstein et al. (53), analyzing a sample drawn from the Minnesota Twin Family Study (a community-based study of adolescents and their families), found that “parental depression, antisocial behavior and drug dependence were associated with offspring migraine.”
As outlined above, studies investigating the relationship between childhood psychopathological symptoms and headache have offered several, often conflicting, interpretations (11,17). In our study, both the migraine and the TTH groups, compared with the controls, showed (in their Total scores and Internalizing scale scores) a marked presence of psychopathological symptoms, even though migraine was also found to be associated with externalizing disorders. In the TTH group there emerged a strong statistically significant difference between Total and Internalizing scale scores. Instead, the direct comparison between the migraine and TTH patients did not show significant differences in any scores (Total, Internalizing scale or Externalizing scale). These findings raise several questions that need to be addressed by further studies: Does there exist a common substrate in childhood migraine and TTH? If so, is this common substrate related to the headache or to chronic physical illness in general? A recent meta-analysis (54) observed greater increases in internalizing than in externalizing problems in children and adolescents with chronic physical illness (including headache, with no distinction made between migraine and TTH). Moreover, the authors observed, in epilepsy and migraine/TTH, above-average levels of internalizing and externalizing problems, a finding that seems to point to a role of impaired brain function (e.g. chronic fatigue syndrome showed the largest effect size for internalizing problems without any increase for externalizing problems). Another meta-analysis by the same authors (55) revealed comparable levels of anxiety in children with migraine/TTH, chronic fatigue syndrome and epilepsy (levels that, surprisingly, were higher than in subjects with life-threatening diseases such as cancer or human immunodeficiency virus (HIV)). To further complicate the debate, a study conducted from the genetic perspective found a correlation between high levels of anxiety and migraine (56).
The present meta-analysis has some limitations due to methodological biases in studies carried out in the field of child and adolescent headache. Unfortunately, most of the studies assessed psychopathological symptoms in relation to the presence or absence of specific headache diagnoses, and without taking headache frequency into account. This is a major omission, since chronic pain is, per se, associated with psychological symptoms (44,54). Another likely source of bias is the patient’s first headache diagnosis (i.e. the form first diagnosed): Most studies, clinical as well as population based, tend to consider the most severe type of headache presented by patients, neglecting the possibility of the co-existence of more than one type of headache. In addition, while our decision to select studies only on the basis of the CBCL allowed us to reduce unwanted variation between them, this instrument does not allow clear diagnosis of psychopathological symptoms, so that no conclusion about the prevalence of specific psychological disorders can be made. Finally, we did not distinguish studies by age of the enrolled populations, but the limited number of studies included prevented the feasibility of meta-regression analyses to test the potential confounding effect of age.
Further studies are needed in order to analyze similarities and differences between psychopathological symptoms, migraine, TTH and other forms of chronic recurrent pain other than headache. The findings of our study did not allow us to disprove the presence of a Berkson’s bias (self-selection of more psychologically vulnerable patients in clinical studies), even though we chose not to restrict the meta-analysis to clinical studies. However, studies in the general population are needed in order to reduce the effect of the lack of population studies on this topic.
Moreover, in the headache field, it should be mandatory to compare different headache types, considering not only the clinical phenotype and attack frequency, but also the presence of more than one clinical diagnosis. In addition, the problem of “probable diagnoses” according to ICHD-II (16) should be better addressed in childhood headache studies given that childhood headache per se differs from and does not fulfill the criteria used for the adult form (57).
Notwithstanding the shortcomings of this study (e.g. the small number of studies, the failure to distinguish between children and adolescents, or to consider discrete psychiatric categories rather than psychopathological profiles and symptoms, the adoption of a self-report questionnaire data), it has nevertheless allowed us to highlight the risk of psychopathological functioning in migraine patients (reflected in their Total score, and in the presence of internalizing and externalizing symptoms, particularly internalizing ones). This risk also emerged in the TTH patients, in whom, however, it was more confined to internalization disorders. Notwithstanding these differences, the psychopathological profile, as defined by the CBCL, was very similar in these two forms of headache. This finding raises questions, also in light of genetic studies that are increasingly lending support to the hypothesis of a shared genetic linkage between migraine and anxiety and depression (56,58). Further studies are needed to explain these similarities, which seem to have two possible explanations: One hypothesis is that migraine and TTH are not separate entities and the other is that the development of psychopathological symptoms is influenced by the need to cope with a chronic, recurrent pain condition. Another possibility is that in migraine the cause might be a biological one with a genetic origin and in TTH a psychological one, i.e. the effect of continuously suffering from headache.
There is also a need for studies to compare the functioning of children affected by headache with that of pediatric patients affected by other forms of chronic pain, in order to clarify whether the psychopathological profile is headache related or, instead, reminiscent of that seen in chronic pain generally, as it has been found to be in adults.
Whatever the case, clinical work with headache patients demands, from the youngest age, an integrated approach (medical and psychiatric/psychological). In our view, a child with migraine or TTH does not necessarily need to be referred to a child psychologist or psychiatrist unless his or her clinical or behavioral features warrant such a referral. Psychological disturbances are often difficult to detect and treat, and the pediatrician or neurologist/child neuropsychiatrist therefore needs to be not only increasingly skilled in the management of the doctor-patient relationship, but also extremely well versed in the mind-body relationship. Authoritative researchers such as Kandel and McDougall (59,60) have always argued that there is an ongoing interaction between our health and our thoughts, emotions, concerns, anxieties and tensions.
In our opinion, the relationship between psychopathology and migraine and TTH deserves to be energetically researched by practitioners involved in diagnosing and treating affected children and adolescents, and in this context the CBCL may be a very good instrument for psychopathological screening. However, future research should point to allowing a diagnosis according to the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) criteria, adding other structured diagnostic tools to the screening made by the CBCL.
Eccleston et al. (61) found that “there is very good evidence that psychological treatments, principally relaxation and cognitive behavioral therapy, are effective in reducing the severity and frequency of chronic headache in children and adolescents”; furthermore, the recent updated and expanded version of their meta-analysis showed that this beneficial effect is maintained over time (62). Finally, it is critically important to consider emotional as well as familial factors when dealing with headache having onset in children or adolescents, because it is imperative to prevent a chronic evolution and medication overuse.
In conclusion, there remain many unanswered questions on the nature of the relationship between headache and psychopathology that call for more studies in this field.
Footnotes
Clinical work with headache in children and adolescents should include the psychological assessment because of the relevance of psychopathological symptoms.
Psychopathological symptoms are important for all sub-types of primary headache and should be a part of the daily clinical practice.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.