
Abstract
Only a few studies have been published of the outcome of adolescent headache (HA). The aim of this study was to examine the predictors of the outcome of headache frequency. A population-based sample of 13-year-olds with or without HA (N = 228) was followed to the age of 16 years. HA was classified on the basis of a face-to-face interview and clinical examination. The outcomes of monthly HA (>1/month) and non-frequent HA (0-1/month) were studied. Frequent use of analgesics, female gender and multiple non-headache pain predicted the persistence of monthly HA (>1/month). Significant predictors for worsening non-frequent HA (from 0 to 1/month to >1/month) were female gender, consistent migraine and high basic educational level of one parent. Adolescents frequently using analgesics constitute a risk group for a poor outcome of HA. Especially girls meeting this criterion should be considered a target group in the planning and implementing of preventive measures.
Introduction
Little is known about the determinants of a poor or favourable outcome of adolescent headache (HA), although most adult patients with chronic headache (defined as HA at least 15 times a month) report that their HA started in adolescence (1) and frequent HA is a risk factor for later chronic HA (2–4). As chronic HA has proved difficult to treat (5), it is highly important to prevent the worsening of frequent but non-chronic HA (3). To prevent the worsening of HA, it is important to determine the predictors for the outcome. Various factors influence HA frequency and transform episodic HA into a more chronic form. One simple aetiology and a simple pathophysiological mechanism, however, cannot be expected. The biological mechanisms of chronic HA remain uncertain, but several hypotheses have been proposed (6). In adults, different factors have been studied and, for example, the aggravating role of overconsumption of analgesics (7–9), peripheral and central sensitization of nociceptors (2, 10, 11), muscle tenderness (11), psychosocial stress (12) and genetic factors (13) have been associated with chronic HA. However, it is uncertain whether these same predictors are important for the worsening of childhood or adolescent HA (14).
Most population-based studies of children and adolescents are cross-sectional, and drawing longitudinal conclusions from cross-sectional data is problematic. Of the few existing population-based outcome studies of childhood and adolescent HA, the most extensive have focused on the subgroup of children with migraine (15–18), showing that 66–83% of schoolchildren with migraine still have migraine after 6–7 years of follow-up (16–18). In a population-based follow-up study of overall HA in children aged 6–12 years (N = 798), 41% of HA sufferers had HA at the end of the follow-up (19). Previous studies have associated gender, age at onset of HA, anxiety, depressive disorders and maternal HA with the outcome of childhood or adolescent HA (17–25).
Subjects and methods
The present study is part of a population-based follow-up study of HA in schoolchildren. The original source population covered all 12-year-old schoolchildren in the city of Turku (total population of 175 000) in south-western Finland. The questionnaire on HA was completed acceptably by 1135 (81%) of the 1409 eligible children (26).
At the age of 13 years, from November 1998 to February 1999, 70 children were randomly selected by computer from each of the following HA groups: migraine (IHS 1.1–1.2), tension-type HA (IHS 2.1–2.2), migrainous disorder (IHS 1.7) and healthy controls. In addition, the entire group of 47 children with tension-type HA not fulfilling the criteria (IHS 2.3) was included in the study population. If a child was unable to participate (24% of children), another child of the same sex, randomly selected in advance, was recruited. The total number of participants was 311. Their HA type was reclassified at a face-to-face interview and clinical examination. As the second, present, edition of the International Classification of Headache Disorders (27) had not yet been published at the time of data collection, IHS criteria from 1988 were used (28). The details of the study design have been published previously (26, 29, 30).
At the age of 16 years, from February to April 2002, all the 311 adolescents were invited to the face-to-face follow-up study. The classification of the HA type was based on a structured interview, neurological examination and the criteria of the Committee of the International Headache Society (IHS) (28). At the ages of 13 and 16 years, monthly HA was defined as more than one HA episode per month during the preceding 6 months and non-frequent HA as one episode or less per month. This cut-off point of HA frequency (>1/month, ≤1/month) was chosen partly because of clinical relevance and also because of statistical needs. However, this is an arbitrary cut-off point. We present here the results of the follow-up study in children from 13 to 16 years of age.
Figure 1 presents the outcome and predictive variables. The outcome variables were: outcome of monthly HA at the age of 13 years, in which adolescents with unchanged monthly HA (>1/month) were compared with those with improved HA (from >1/month to 0–1/month); and outcome of non-frequent HA at the age of 13 years, in which adolescents with worsened HA (from 0 to 1/month to >1/month) were compared with those with unchanged non-frequent HA (0–1/month).
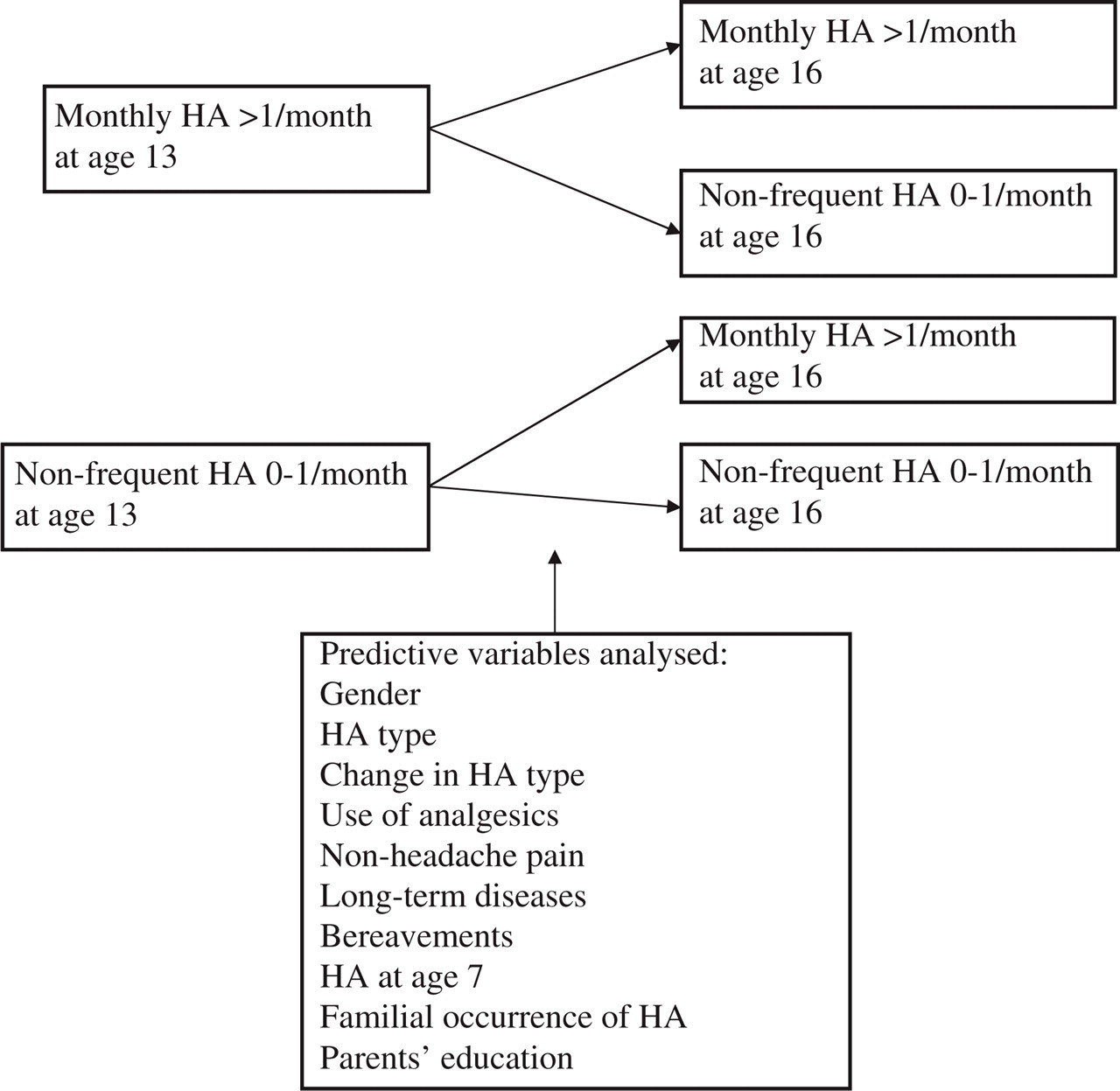
Examined factors for the outcome of headache (HA) frequency.
Definitions of predictive factors
Predictive variables (Fig. 1) included gender, HA type, change in the HA type, use of analgesics, occurrence of non-headache pain, occurrence of long-term diseases, recent bereavement, parents’ basic educational level, familial occurrence of HA and occurrence of HA at the age of 7 years.
A change in the HA type was described using four definitions: tension-type HA (IHS 2.1–2.3) evolving to migraine (IHS 1.1–1.7); migraine evolving to tension-type HA; consistent tension-type HA; and consistent migraine (28).
The use of analgesics was evaluated as the frequency of HA medication per month during the preceding 6 months. The analgesics used were non-steroidal anti-inflammatory drugs (ibuprofen 200–600 mg, N = 107; acetosalicylic acid 500 mg, N = 16; paracetamol 500 mg, N = 15; ketoprofen N = 5; naproxen N = 3; tolfenamic acid N = 1; non-defined anti-inflammatory drugs, N = 14).
Ten different types of non-headache pain (back pain, neck pain, abdominal pain, limb pain, sore throat, earache, eye ache, toothache, chest pain and other pain) were classified by frequency using a four-step scale (1 = no pain, 2 = pain <1/month, 3 = 1–3/month, 4 = ≥4/month during the preceding 6 months). Accordingly, the sum frequency could vary between 10 and 40.
Long-term illnesses consisted of diabetes mellitus, bronchial asthma, allergy, arterial hypertension, coeliac disease, lactose intolerance, thyroid disease, renal disease, heart disease, developmental language disorder, cancer, rheumatic disease and other disorders. The group ‘other disorders’ included epilepsy (N = 4), deformities of the spine or feet (N = 3), psoriasis (N = 2), Turner syndrome, spastic hemiplegia, colitis ulcerosa, von Willebrand's disease, anorexia, hearing problems and cataract, one of each.
Bereavements between ages 12 and 16 years included parental divorce, parental change of jobs, parental unemployment, relocation of home, economic problems, domestic quarrels, long-term disease in the family and death of a close relative.
The basic education of the parents was categorized according to whether both, one or neither of the parents had passed the secondary-school matriculation examination. The Finnish matriculation examination means acceptable completion of 12 years of schooling and a national written examination.
A question was asked about the occurrence of HA at the age of 7 years in a separate questionnaire study on HA at the age of 7 years, where 86% of the study population (N = 196) had also participated (31, 32).
Statistical analysis
The descriptive values are expressed as means and SD, medians and interquartile ranges, or frequencies and percentages. Univariate associations between categorical variables were evaluated using the χ2 test and Fisher's exact test when appropriate. Differences in continuous variables between the HA groups were calculated using the Mann–Whitney U-test and differences in changes using the Wilcoxon signed rank test. Changes in HA type were analysed using the test for marginal homogeneity. Gender-adjusted odds ratios were calculated for significant predictive factors of univariate analysis using logistic regression (33). For logistic models, continuous explanatory variables were divided into three classes consisting of the lowest quartile, the combined second and third quartile and the highest quartile, because of the non-linear relation of these continuous variables and logit-function. The results were quantified by odds ratios with 95% confidence intervals. P-values <0.05 were considered statistically significant. Statistical computations were done using the SAS System for Windows, release 8.02 (SAS Institute, Cary, NC, USA).
The study design and the informed consent procedures were approved by the Joint Ethics Review Committee of the Turku University Medical Faculty and the Turku University Central Hospital.
Results
Outcome of headache frequency
At the age of 16 years, 228/311 adolescents (73%; 82% of girls and 65% of boys) participated in the follow-up study. The number of drop-outs varied from 20 to 27% in the HA groups and was 31% in the healthy controls. The difference was statistically non-significant (P = 0.31).
Table 1 shows the overall changes of HA frequency from 13 to 16 years. The mean HA frequency increased in girls from 2.6 to 3.1 times a month (P = 0.28). In boys, HA frequency decreased from 2.1 to 1.2 times a month (P = 0.0002) during the follow-up. The mean HA frequency at the beginning of follow-up was 4.5 times a month (SD 4.2) for monthly HA (>1/month) and 0.39 times a month (SD 0.38) for non-frequent HA (≤1/month). The overall percentage of adolescents suffering from monthly HA was virtually the same at age 13 years (35%) as at age 16 years (36%). However, internal changes in the study group appeared. Table 2 shows the outcome of monthly and non-frequent HA. In half (49%) of the 13-year-olds with monthly HA, HA improved to non-frequent HA, and in equally many (51%) HA remained unchanged. Of adolescents with non-frequent HA, in more than one-quarter (28%) HA worsened to monthly HA, while in 72% HA remained unchanged. A significant difference was found between boys and girls in the outcomes of both monthly and non-frequent HA (Tables 3 and 4).
Changes in headache (HA) frequency from 13 to 16 years of age

Outcome of monthly and non-frequent headache from 13 to 16 years of age

Univariate analysis of factors associated with the outcome of monthly headache in children from 13 to 16 years of age

M, Migraine (= ICHD 1); TTH, tension-type headache (= ICHD 2); Improved, headache >1/month at 13 years, 0–1/month at 16 years.
χ2 or Fisher's exact test.
Mann–Whitney U-test.
Univariate analysis of factors associated with the outcome of non-frequent headache in children from 13 to 16 years of age

M, Migraine (= ICHD 1); TTH, tension-type headache (= ICHD 2); Worsened, headache 0–1/month at 13 years, >1/month at 16 years.
χ2 or Fisher's exact test.
Mann–Whitney U-test.
Factors associated with outcome of headache frequency
Frequent use of analgesics, female gender and non-headache pain were associated with unchanged monthly HA when compared with improved HA (Table 3). The familial occurrence of HA was associated with unchanged monthly HA in boys (P = 0.04) but not in girls (P = 1.00). In adolescents with tension-type HA, HA frequency persisted monthly more often in girls than in boys (P = 0.03). When worsened HA was compared with unchanged non-frequent HA, worsened HA was associated with female gender, consistent migraine and the matriculation examination of one parent compared with parents with no matriculation examination. Further, there was a trend of HA worsening with the use of analgesics (Table 4). The other predictive factors studied did not associate with the outcome of HA frequency (Tables 3 and 4).
Multivariate gender-adjusted logistic regression analysis
Gender-adjusted odds ratios were calculated for factors that were significantly associated with unchanged monthly HA or worsened HA in the univariate analyses. Frequent use of analgesics was the most powerful determinant of unchanged monthly HA. Non-headache pain proved to be a less significant explanatory factor after categorization (Table 5). Two factors showed an independent association with worsened HA in the gender-adjusted analysis (Table 6), namely the matriculation examination of one parent and consistent migraine when compared with migraine evolving to tension-type HA.
Multivariate gender-adjusted logistic regression analysis of significant associated factors for the outcome of monthly headache
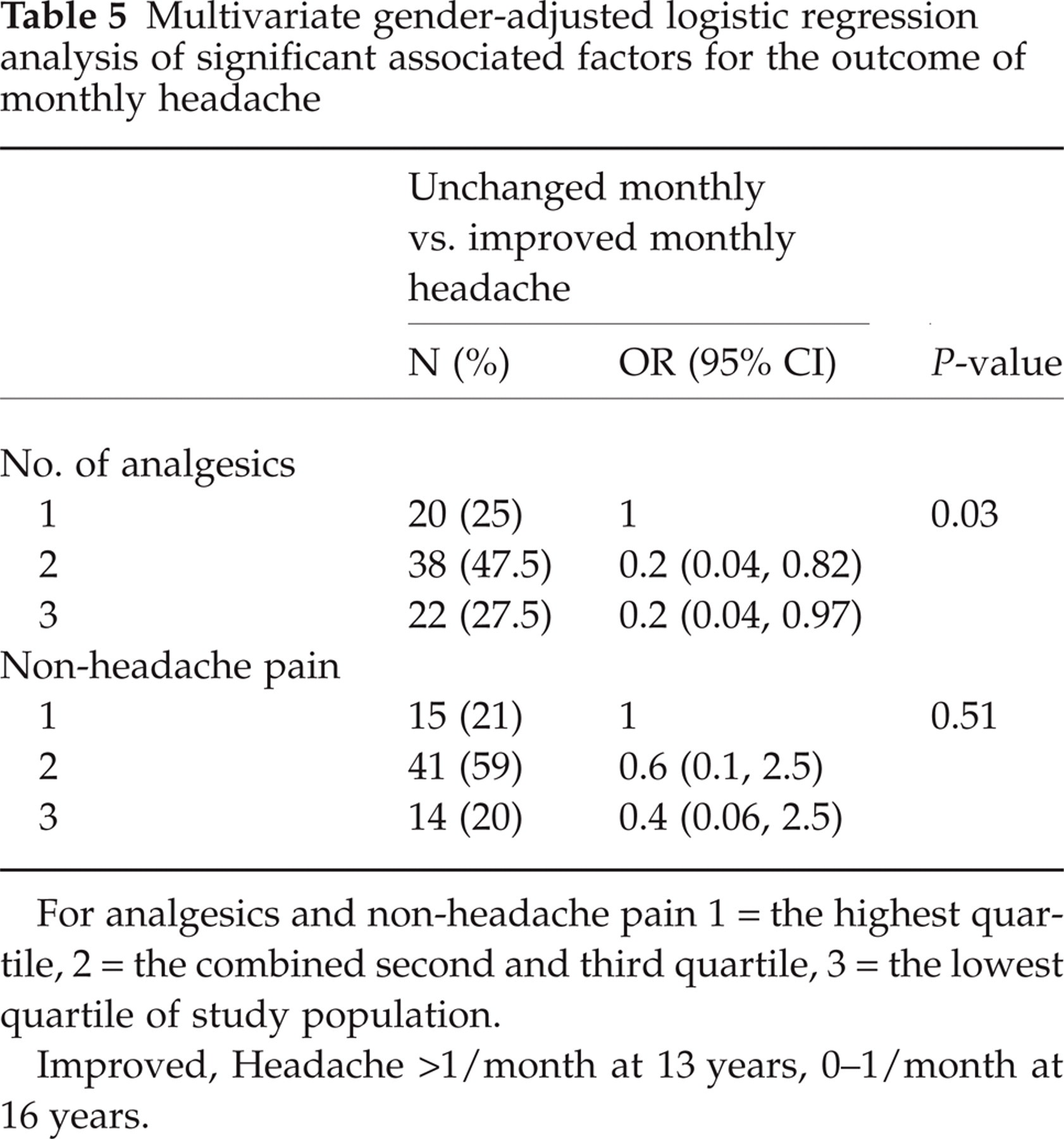
For analgesics and non-headache pain 1 = the highest quartile, 2 = the combined second and third quartile, 3 = the lowest quartile of study population.
Improved, Headache >1/month at 13 years, 0–1/month at 16 years.
Multivariate gender-adjusted logistic regression analysis of significant associated factors for the outcome of nonfrequent headache

M, Migraine (ICHD 1); TTH, tension-type headache (ICHD 2); worsened, headache 0–1/month at 13 years, >1/month at 16 years.
To exclude the confounding effect of HA frequency on the effect of the use of analgesics, we separately analysed adolescents experiencing HA in excess of five times a month at the beginning of the follow-up period. With increasing use of painkillers, the probability of unchanged monthly HA increased also (P = 0.03), although no difference was seen in the median of HA frequency at the beginning of follow-up between adolescents with unchanged monthly HA and adolescents with improved HA in this frequency group (P = 0.45).
Discussion
Female gender, frequent use of analgesics, consistent migraine and higher basic educational level of one parent were independently associated with unchanged monthly HA or with HA transforming to monthly HA during the adolescent years. Many previous studies have evaluated the predictors for the occurrence of HA, mainly cross-sectionally. Our study focused on predictors for changes in HA frequency instead of predictors for the prevalence of HA, which is important for finding ways to prevent an unfavourable course of HA. The predictors determined in our study may indicate or contribute to the worsening of HA.
Frequent use of analgesics proved to be a determinant of unchanged monthly HA, and its influence was not explainable by the primary frequency of HA or by excessive use of analgesics. Analgesic overuse has been shown to predict chronic migraine (at least 15 times a month) and persistence of chronic daily HA in adults and in the elderly (7–9). In recent clinic-based studies, however, adolescent medication overuse has emerged as an uncommon cause of chronic daily HA in adolescents (34, 35). In our study, the frequency of use of analgesics was low in terms of the ICHD diagnostic criteria of analgesic overuse HA (analgesics >15 days/month) (27). Only one subject in our study group used analgesics 15 times a month and only eight of 228 participants used analgesics weekly. The mean frequency of analgesics use was 1.79 times a month (0–15/month) for monthly HA and 0.20 times (0–1) for non-frequent HA. Instead of being explicable by the analgesic overuse HA, our results could indicate either changing sensitivity to pain (36) or a changing attitude to pain during the process of HA becoming chronic. The increased use of analgesics in those with a poor outcome of HA would thus be a sign of increased physiological or psychological sensitivity to pain instead of a cause of the increasing frequency of HA. As this study was not a clinical trial, we could not systematically optimize the analgesic use and we do not have detailed data on the timing of analgesic taking. Even though our results on the predictive importance of the frequency of analgesic use are clear, the explanation for the findings needs further studies. On the basis of our results, we do not claim that it is harmful to treat HA; on the contrary, it is considered important to treat HA episodes properly to arrest the pain sensitization process.
We found that monthly HA was more likely to begin and persist in females than in males. Similarly, previous clinic-based follow-up studies (15, 23, 37) have found a favourable outcome of HA mainly in boys. This might depend on differences in the genetic background of HA between girls and boys and the earlier age of onset of migraine in boys (38). Several mechanisms have been suggested as explanations for gender differences in overall pain sensitivity: Sex hormones, biological differences in processing noxious stimuli and psychosocial factors such as gender role beliefs, pain coping strategies, moods, pain-related expectations and familial factors may alter pain responses (39–42).
In univariate analysis, unchanged monthly HA could also be predicted by non-headache pain. In previous cross-sectional studies, children with HA have reported more non-headache pain (43–45). Our results indicate that the spreading of pain is a marker for the chronicization of HA. If different types of pain do not have a common pathogenesis or are not associated via a third factor, such as depression, the spreading of pain could be due to sensitization (10, 11) and such neurophysiological changes could be coupled with different cognitive and emotional processes.
Our results do not confirm those of the previous studies, according to which migraine has a poorer outcome than the other types of HA (15, 18, 23). The HA type at the beginning of follow-up was not associated with the outcome of non-frequent or monthly HA. However, consistent migraine compared with migraine evolving to tension-type HA was associated with worsened HA. Using the IHS criteria of 1988 (28) instead of new ICHD criteria (27) did not influence the results, because the one-digit criteria for migraine and tension-type HA are identical in these two versions.
The associations between socioeconomic factors and HA are controversial in different cross-sectional studies (18, 19, 45–49). The high educational level of a parent is supposed to cause demand for the child's academic success and, thus, stress at school. In the present study, a difference in the basic educational level of the parents measured by a passed matriculation examination was associated with worsened HA; yet no clear explanation can be offered for this finding. The demand for success at school may be even more intensive for adolescents only one of whose parents has reached a higher educational level, or children both of whose parents have a higher educational level already cope with the demands during their first few school years instead of adolescence.
Our study showed a trend for persistence of monthly HA if there were other HA sufferers in the family. A genetic risk exists for HA, especially for migraine, while other family factors such as coping methods and social functions of the family also contribute to the outcome of HA (50–52). In agreement with earlier follow-up studies, concomitant diseases (19) or HA in early life (19, 23, 53, 54) did not predict worsening or persistence of HA at puberty.
Many previous studies of children and adolescents have reported varying associations of stress factors with HA (19, 21, 22, 35, 49, 55–58). One aspect of experiencing stress is the anxiety and depressive disorders that are associated with HA and may predict incidence of HA (20, 22, 24, 25). In our study it was possible to analyse associations between changes in HA frequency and bereavements occurring concurrently, which has not been analysed in earlier studies. No causal relationship was evident between the report of personal loss and change in HA frequency. This indicates that even though stress factors may have a temporary provoking role for headaches, they do not have the capacity to change the overall outcome of HA in adolescence. However, measuring the influence of stress factors is complex. Responses to different stress factors are highly subjective, and timing of severe anguish after bereavement is difficult. For example, parents’ quarrels may be a burden to the children years before a divorce. Psychiatric disorders, anxiety and depressive disorders associated with HA may predict its incidence (20, 22, 24, 25) and may also be important for predicting the outcome of HA in an individual, but they were not included in the present analysis.
Although we found important predictors of HA, more studies are needed, because this epidemiological study design does not permit a thorough explanation of the association between the outcome of HA and the use of analgesics or multiple pain. The number of subjects with truly chronic HA (at least 15 HA episodes a month) was low in our population and our results can not be directly applied to this group of patients. The timing of the follow-up was slightly different from the original face-to-face study (November to February–February to April). Increased amounts of natural light during the spring may influence HA frequency in some patients. However, school attendance, exam periods and school vacations do not differ significantly between these two time periods. As we asked for the mean frequency of HA during the past 6 months, we consider that the difference in the timing should not affect the results.
Conclusion
Adolescents with frequent use of analgesics constitute a risk group for the poor outcome of HA. Girls fitting this description particularly should be considered a target group when planning and implementing preventive measures.
Footnotes
Acknowledgements
This study was supported by grants from the city of Turku, the University of Turku and the Turku University Central Hospital. We acknowledge Olli Kaleva BSc for his skilful computation of the statistical analyses, Mrs Riikka Bäcklund for her practical assistance and Mrs Inger Vaihinen for her secretarial assistance.