
Abstract
The aim of this study was to evaluate the validity of the headache diagnoses (migraine and tension-type headache) obtained from short interviews by nurses, where the subjects were asked to identify their headache(s) based on recognition of typical headache descriptions. All students in junior high schools and high schools aged 12-19 years in Nord-Tr⊘ndelag county, Norway, were invited to participate in the youth part of the Nord-Tr⊘ndelag Health Study ('Helseunders⊘kelsen i Nord-Tr⊘ndelag'-HUNT), 1995-1997. In this cross-sectional study a total of 8984 students (88%) completed a comprehensive questionnaire with different health-related items. Of these, 6149 were also interviewed by nurses about their headache complaints by giving them two alternative headache descriptions accordant with either migraine or tension-type headache (Head-HUNT-Youth). The headache diagnoses obtained from nurse interviews were validated in a stratified random sample enriched with headache subjects from the interviewed population. Out of 159 invited individuals, 112 (70%) participated in extensive semistructured interviews by neurologists. The overall chance-corrected agreement (K) was 0.76 (confidence interval (CI) 0.66-0.86), which is considered good. For migraine, the positive and negative predictive values were 89% and 90%, respectively, and the chance-corrected agreement (K) was 0.72 (CI 0.58-0.87). For tension-type headache, positive and negative predictive values were 83% and 91%, respectively, and chance-corrected agreement (K) was 0.74 (CI 0.62-0.87). There was good agreement between the headache diagnoses obtained from the short interviews by nurses and the extensive interviews by neurologists. Short interviews based on recognition of typical headache descriptions seem to be an alternative and efficient way to identify migraine and tension-type headache sufferers among adolescents. The method can be useful in epidemiological research, e.g. in estimation of headache prevalence.
Introduction
Headache is one of the most common complaints in childhood and adolescence. The reported prevalence rates vary between different studies (1–16), possibly because of differences in study methodology, diagnostic criteria and population samples (17). Introduction of the International Headache Society (IHS) criteria (18) has improved the sensitivity and specificity of headache diagnosis, but headache in children differs from that in the adult population (19–24) and the ability to describe and conceptualize pain is also age related (25). As children age, their descriptions and understanding of pain and headaches become more complex (26). Hence the applicability of the IHS criteria in children and adolescents has been debated (27–36). In order to increase the sensitivity for diagnosing migraine and tension-type headache some modifications of the current 1988 IHS criteria have been proposed (34).
When assessing headache diagnoses in epidemiological studies it is preferable to use clinical interviews (37), but for economic and practical reasons this is impossible in large population-based studies. Therefore, in the present study, headache diagnoses (migraine (MI) and tension-type headache (TTH)) were made from short interviews performed by nurses, who asked the subjects to identify their headache(s) on the basis of typical headache symptom descriptions. The main purpose of the present study was to evaluate the validity of these diagnoses by comparing them with diagnoses based on extensive clinical interviews by neurologists, with several years of experience in clinical management of headache disorders.
Materials and methods
During a 2-year period from August 1995 to June 1997, all students in junior high schools (aged 12–15 years) and high schools (aged 16–19 years) in Nord-Tr⊘ndelag county in Norway were invited to participate in the youth part of the Nord-Tr⊘ndelag Health Study (‘Helseunders⊘kelsen i Nord-Tr⊘ndelag’ = HUNT). Nord-Tr⊘ndelag, which is one of 19 Norwegian counties, is located in the middle part of the country. The population is scattered, and no city has more than 21 000 inhabitants.
In total, 8984 (88%) of the students (mean age 16.0 years, 49.7% girls) completed a self-administered questionnaire with more than 100 health-related items. The questionnaire was filled in during 1 school hour. Within a month after completing the questionnaire specially trained nurses interviewed 6149 students about their headaches (mean age 16.0 years, 52.1% girls). The interviews were performed at the schools and during school hours. During the interview the nurses first asked the students whether they ever had experienced recurring headaches not related to cold, fever or any other type of disease, and whether they had experienced such headaches during the last 12 months. Two typical headache symptom history descriptions, one for MI and one for TTH, were then read for the students and the students were asked to classify their headache(s) according to those descriptions.
The descriptions contained typical features for both MI and TTH in accordance with the IHS criteria, but the number of attacks or episodes and the duration of headaches were not included (see Appendix). The students were also given a third alternative (‘non-classifiable headache’), in case none of the two descriptions resembled their headaches. The nurses filled in the students’ answers, and they could also answer questions from the students regarding the headache descriptions. Headache frequency was also registered. Each interview took less than 10 min.
The headache diagnoses obtained from nurse interviews were validated in a stratified random sample enriched with headache subjects from the whole interviewed population within 2 months after completing the questionnaire. Out of 159 invited students, 112 (70%) participated in extensive semistructured interviews by neurologists (mean age 16.3 years, 63.4% girls). The neurologists had several years of experience in clinical management of headache disorders. The proposed revision of the IHS criteria was used for the headache diagnosis (34). In a few cases, the neurologists made diagnoses in patients whose headache was not in strict accordance with the IHS criteria. In these cases, a consensus about the diagnoses was formed among the neurologists performing the interviews. If more than one headache type coexisted in one person, the person was classified according to the dominating headache type. Thus, both nurses and neurologists classified the headache as MI, TTH, and other headache (and no headache) for the statistical analyses.
All participants signed a written consent, and for students < 16 years old a written consent was given by the parents. The Regional Medicine Ethical Committee and the Norwegian Data Inspectorate Board approved the study.
Statistical analyses
Sensitivity, specificity, predictive values and Cohens’ κ with 95% confidence intervals (CI) were calculated individually for each of the three headache types (three 2 × 2 tables with counts for the actual headache type vs. the others were constructed). κ was also calculated for the overall agreement in the 4 × 4 table. The paired differences between the prevalences estimated by the two methods were compared with McNemar's test. Data analysis was performed with the Statistical Package for the Social Sciences (SPSS), version 10.0 (Chicago, IL, USA).
Results
Ninety-two of the 112 subjects interviewed by neurologists had headache. Of these, 32 (29%) had MI, 46 (41%) had TTH and 14 (13%) had headache that could not be classified. In this same sample of 112 subjects, the prevalence of MI, TTH and non-classifiable headache based on nurse interviews was 23%, 43% and 13%, respectively. The paired differences between the prevalences estimated by the two methods were not significant (P = 0.15, 0.79 and 0.72; McNemar's test). The agreements between nurse and neurologist rates are shown in Table 1. The overall chance-corrected agreement (κ) was 0.76 (CI 0.66–0.86), which is considered good (38).
Correspondence between nurse diagnoses based on recognition (nurse's descriptive interviews; rows) and diagnoses based on clinical interviews by neurologists (gold standard; columns)

MI, Migraine; TTH, tension-type headache.
At the neurologists’ interview a total of 11 headache sufferers indicated that they suffered from a combination of MI and TTH. Of these, 10 individuals indicated that MI was the most bothersome headache. Only one indicated TTH as the most bothersome headache, mainly due to the frequency of this headache. At the nurse interviews only five of the 11 individuals had indicated that they had two different headaches.
The comparison between sensitivity, specificity and predictive values obtained by the nurses and the neurologists for each diagnosis is shown in Table 2. The predictive values were of the same order of magnitude for MI (89–90%) and TTH (83–91%). The chance-corrected agreement (κ) was 0.72 and 0.74 for MI and TTH, respectively (Table 2).
Sensitivity, specificity, and predictive values of recognition-based headache diagnosis (nurses’ interviews of 112 subjects, 92 of whom suffered from headache)

MI, Migraine; TTH, tension-type headache.
The clinical characteristics in different diagnostic groups for the main diagnoses based on the gold standard (extensive interview by neurologists) are shown in Table 3. The non-classifiable headache group consisted of eight individuals that fulfilled all but one of the migraine criteria (IHS 1.7), while six had headaches that were not classifiable (IHS 15). In the latter group three had frequent headaches, i.e. between 1 and 5 days per week. Twenty-eight of the 47 subjects not participating in the neurologist's interview had headache, six (12.2%) had MI, 17 (34.7%) had TTH, and five (10.2%) indicated non-classifiable headache.
Clinical characteristics in different diagnostic groups (main diagnoses) based on the gold standard (extensive interview by neurologists)
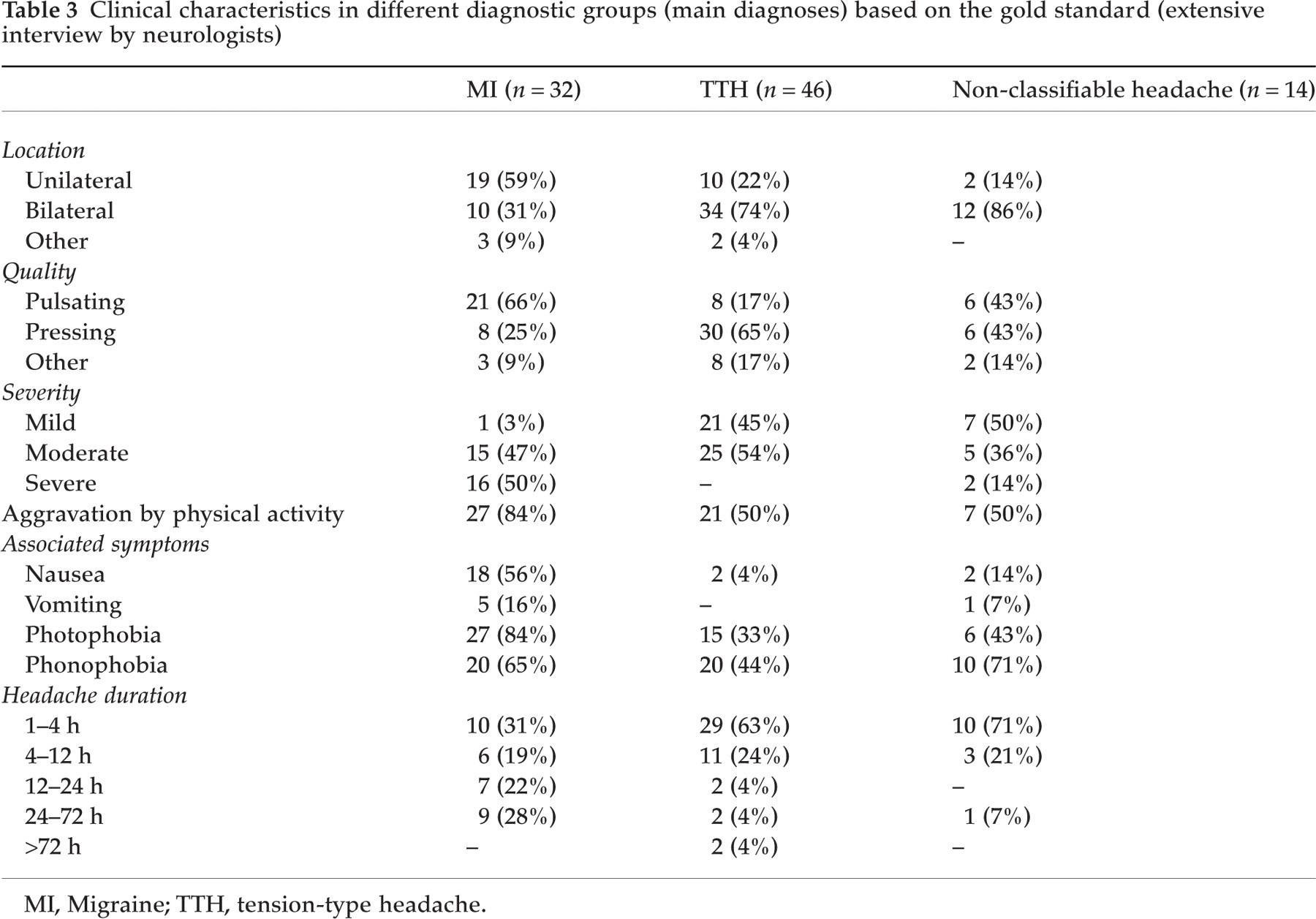
MI, Migraine; TTH, tension-type headache.
Discussion
In the present study we have shown that the agreement between headache diagnoses based on short typical descriptions and extensive interviews by neurologists is good (38) both for MI and TTH. In addition, the positive and negative predictive values were high. This indicates that the probability of correct diagnosis is high when a short interview like the present one is administered (38). This will enable researchers to estimate headache prevalence reliably and efficiently.
Self-administered questionnaires are often used in epidemiological research and have been validated by comparing the questionnaire responses with clinical interviews, which are considered the ‘gold standard’ (37). Interviews are more time-consuming, more expensive and often difficult to apply in larger population samples. Since headache features and the ability to describe pain may change with increasing age (25, 26), the use of headache descriptions for recognition rather than headache-specific items in a questionnaire may be a better way to obtain valid information for diagnosis. However, we have not compared the validity of diagnoses based on a headache questionnaire vs. clinical interviews.
The students were invited to the neurologist interviews after school hours and the interviews were performed outside the school area, thus subjects with headache complaints might have been more likely to attend than those without any headache or with only minor complaints. Among the 47 invited subjects that did not participate in the neurologists’ interviews 19 were without headache and 17 had TTH. The purpose of the present study, however, was to validate the nurse interviews and not to estimate the prevalence of migraine and tension-type headache.
This study used a headache-enriched sample for validation. The sensitivity of the recognition-based technique will accordingly be slightly less when applied in an unselected population. This technique slightly underestimated the true MI prevalence because nine students were classified as MI in the neurologist interviews but not in the nurse interviews. There was no significant difference in the number of subjects with MI in the nurse compared with the neurologist interviews (23.2% vs. 28.6%, McNemar's P = 0.15). The difference may accordingly reflect a non-systematic random discrepancy between the two methods. A possible underestimation cannot be excluded, however, and if so, its cause is not clear. It might be conceivable that adolescents pay less attention than adults to self-observation of associated symptoms like nausea, exercise intolerance or photo- and phonophobia, particularly if the headache history is short or if attacks are infrequent. In that case, the associated symptoms may be revealed only during a more lengthy interview. The recognition-based technique may also underestimate the occurrence of more than one headache, since only five out of 11 with a combination of MI and TTH indicated this in the nurse interviews.
The number of migraine attacks was not considered in the present study (8, 16). In addition, we omitted the criterion of attack duration (4–72 h) in the descriptions given during the nurse interviews because several studies have shown that the duration is often shorter in children and adolescents (27, 29–31, 33–35) than what has been outlined in the IHS criteria (18).
It seems that the criterion of headache location was fulfilled more often in adolescents than in children for both MI and TTH (36). One study reports unilateral headaches in> 75% of migraineurs aged 10–18 years (21). The results of our study show for the whole group that MI was unilateral in 59% of the cases, whereas TTH was unilateral in only 26%. Among MI sufferers under the age of 16, however, only 37% had unilateral headache, in contrast to 68% of those over the age of 16. A similar trend was found for TTH patients, in whom the headache was bilateral in 62% under and 86% of the cases over the age of 16 years.
The description given by the nurses did not exclude bilateral manifestations in MI sufferers or unilateral manifestations in TTH sufferers. Children may have particular difficulties in realizing the unilaterality of the pain, and details of the exact location of the headaches are not always easily obtainable in children and may not be helpful to the diagnosis (4, 23). Pain is usually bilateral in younger children and becomes more unilateral with age (12, 15, 22).
The quality of pain was included in both headache descriptions, but the relevance of this criterion in the differential diagnoses of the headaches is debated (3, 20, 32, 35). The intensity of the pain was also incorporated in the descriptions, but this characteristic is considered by some authors to be less important (3, 5, 13, 20, 24), while others conclude that intensity is useful in the differentiation between TTH and MI (27, 31, 36).
In adults aggravation of pain by physical activity has been found in 95% of MI patients and in 28% of TTH patients (39). In the present study, however, 84% of MI patients and 50% of the TTH patients reported aggravation by physical activity in the neurologist interview. Some consider aggravation of pain by physical activity to be a useful criterion for the differentiation between TTH and MI in children and adolescents (36), but other investigators state that this criterion should not be considered mandatory for migraine in these age groups (26).
The occurrence of nausea or vomiting is considered to be necessary for migraine diagnosis (13, 20, 23, 24), but these symptoms may become less frequent in older children (15). The presence or absence of nausea is considered important for the differentiation between MI and TTH (27, 36). This is in accordance with the present study, because 56% of all migraine sufferers and only 4% of those with TTH had nausea.
The presence of photo- and phonophobia in children and adolescents is reported to be specific but not sensitive for MI, whereas their absence is sensitive but not specific for TTH (36). In the present study photo- and phonophobia was included only in the migraine description, and was found to be more frequently present among those with MI than TTH in the neurologist interviews. Quantitative measurements of photo- and phonophobia in adults show that both MI and TTH patients are significantly more sensitive than healthy controls to light and sound, even outside attacks and in headache-free periods (40–42). In addition, both photo- and phonophobia seem to be unrelated to the severity of the attacks and nausea. Some investigators, however, state that grading accompanying symptoms (nausea, vomiting, photophobia, and phonophobia) rather than merely noting the presence or absence of these symptoms, may improve the ability to differentiate between MI and TTH (27).
There was a good agreement between the headache diagnoses obtained from the short interviews by nurses and the extensive interviews by neurologists. Short interviews based on recognition of typical headache descriptions seem to be an alternative and efficient way to identify migraine and tension-type headache sufferers among adolescents. The method can be useful in epidemiological research, e.g. in estimation of headache prevalence.
Footnotes
Acknowledgements
The Nord-Tr⊘ndelag Health Study (The Young-HUNT Study) is a collaboration between the HUNT Research Centre, Faculty of Medicine, The Norwegian University of Science and Technology (NTNU), Verdal, The National Institute of Public Health, and Nord-Tr⊘ndelag County Council. This part of the study was also supported by an unconditional grant from Pfizer AS, Norway. J.-A.Z. receives a research grant from the Norwegian Research Council.
Appendix
Headache descriptions used in nurse interviews: