
Abstract
Objectives: To characterize overall drug use in migraine in conjunction with multimodal behavioral treatment (MBT).
Methods: Seventy-six adults reporting at least two monthly migraine attacks underwent a randomized, controlled, 24-week MBT intervention. Migraine drugs and symptoms were registered in an Internet-based diary.
Results: During 4256 days of baseline registration, 859 drug doses were taken during 655 of the 856 days with migraine headache. Triptans and analgesics constituted 56.7 and 38.3% of all doses with efficacy ratios of 0.41 and 0.20, respectively. Men displayed significantly lower drug efficacy (p = 0.001), and used triptans significantly less (p < 0.001) and analgesics significantly more (p < 0.001) than women. At the end of the MBT, total drug consumption decreased by 22% (p = 0.029), corresponding to 27% fewer days with migraine headache. Drug efficacy increased during MBT from 0.30 to 0.52 (p < 0.001), mainly explained by an increased proportion of mild attacks, which also was the attack category that displayed the largest increase in drug efficacy.
Conclusions: Triptans were the most used and efficient drugs. MBT led to decreased and more efficient drug consumption. Men used triptans less frequently.
Introduction
Migraine is a disabling chronic headache disorder that is highly dependent on stress-related factors (1–4). Both pharmacological treatment and programs for lifestyle change have shown efficacy in alleviating migraine symptoms and are complementary to each another (5–11). Multimodal behavioral treatment (MBT), combining different modalities for obtaining behavioral modification, has shown promising results in migraine treatment (6, 7, 10).
The introduction of 5-hydroxytryptamine (serotonin) receptor 1B/1D (5-HT1B/1D) agonists (triptans) in the early 1990s marked a significant improvement in acute migraine treatment (12, 13). The initially high cost for these drugs hampered their use in several countries (14–16). However, Sweden has a public insurance system that sets a limit on personal annual drug expenses (presently €180), and for Swedish migraineurs, triptans became the predominant pharmacological treatment shortly after their introduction (17, 18).
Drug use in migraine, especially the use of triptans, has been extensively studied (19, 20), and several generations of triptans have been developed that show minor differences in efficacy (17, 19–22). Most pharmacological studies on migraine are clinical trials designed to test specific drugs, whereas we have found few studies that provide a description of complete migraine drug use – including the use of over-the-counter drugs (23, 24).
The aim of the present study was to characterize the change in overall drug use in a migraine population in conjunction with an MBT intervention (7), the purpose of which was to achieve improved coping with stress but which in itself did not include any intervention or new recommendations with regard to drug use.
Methods
Study design and study population
The participants and data in the present study were generated from a randomized, controlled study evaluating the efficacy of an Internet-administered MBT program for migraine (7). This program was implemented over a period of 24 weeks. Participants were recruited consecutively during an 11-month period from a preceding descriptive study on migraine (2), for which the participants had been recruited via advertisements in the local daily newspaper.
Eighty-three out of the 150 participants of the initial study agreed to the present study. Fifty-eight women and 25 men, all ≥18 years of age, were randomized into one of two treatment groups (n = 27; n = 28), of which one group also received massage, or a control group (n = 28). Figure 1 shows a flow chart of the study design and the number of dropouts in the three groups (altogether seven dropouts). A 56-day baseline registration was performed prior to randomization into the three study groups. After randomization the two intervention groups had a 3-month registration period with or without massage, followed by the 6-month MBT intervention. The control group went straight on to a 6-month placebo treatment consisting of a 15-minute muscular relaxation program communicated via a compact disc (CD), which was practiced ad libitum. It was considered important to omit the initial 3-month observation period for participants in the control group to avoid problems with compliance due to exhaustion.
Flow chart of the study design with group sizes and dropouts. MBT: multimodal behavioral treatment; CD: compact disc; R: randomization; Q: questionnaires.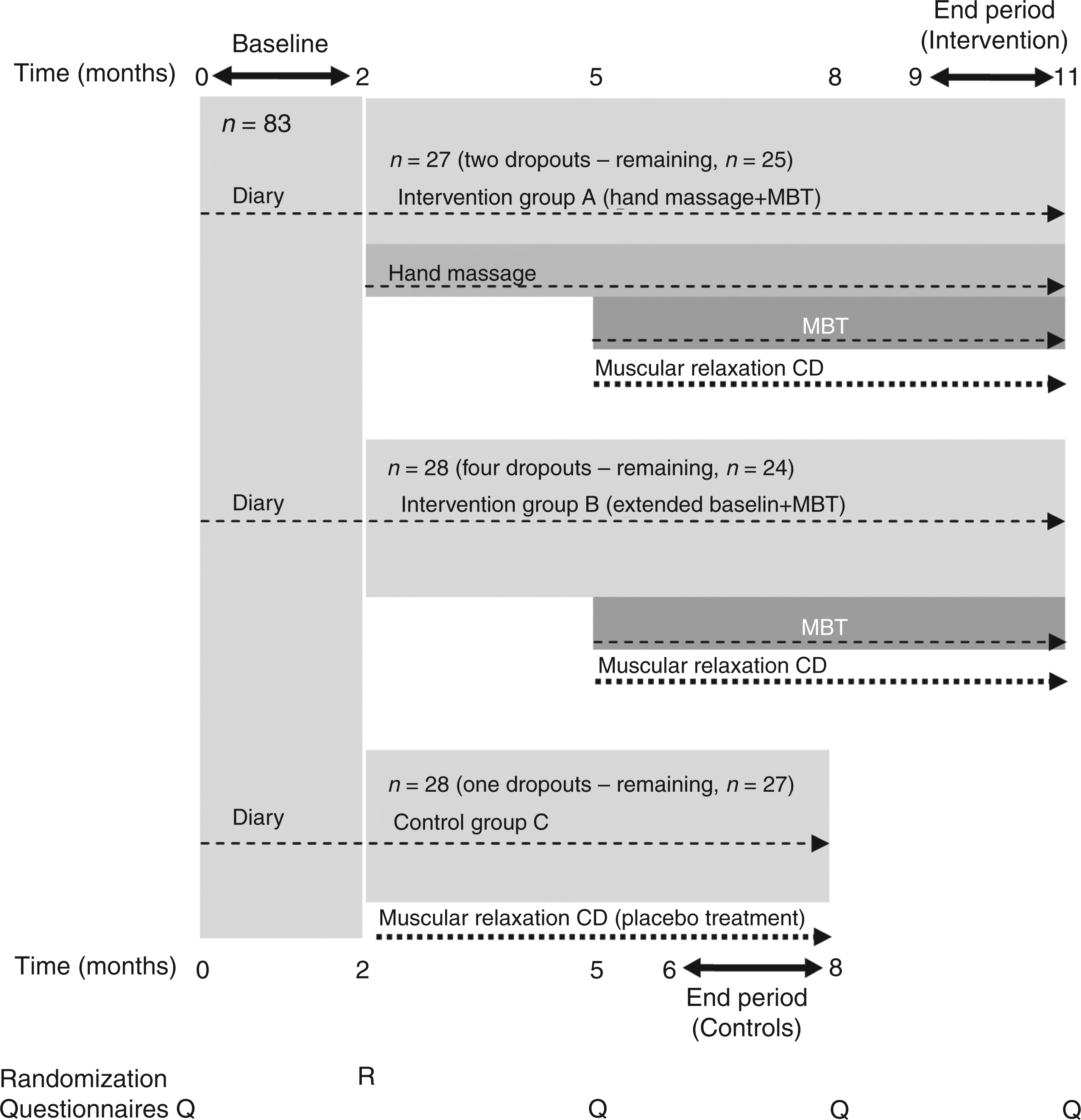
The MBT consisted of a 53-page training program administered via the Internet. The program was aimed at improving stress coping skills and was divided into the following topics: stress physiology, physical activity, diet, thought patterns, handling of emotions, and attitudes. A detailed description of the program and its effects are given by Hedborg and Muhr (7). Both intervention groups showed significantly decreased average migraine frequency compared to the control group (7) but with no statistical difference between them and were therefore merged in the present study (n = 55). The inclusion criteria for the study were two or more migraine attacks a month. To verify the migraine diagnosis according to the International Classification of Headache Disorders, 2nd edition (25), all participants were examined by one of the authors (CM), a specialist in neurology, prior to inclusion.
An Internet-based diary was used for migraine recording, which also included recordings of all migraine drug doses. The diary had a compulsory design. As a minimum, work attendance and stress level were registered each day – otherwise it was impossible to continue the study. The participants were asked to record the time points for: start of migraine headache, waking up with migraine, each migraine drug dose, and for becoming pain-free. The definition of a multiple-day attack was sustained headache at waking up one day or several days in a row. For each attack, a 4-point self-report scale was used for determining the level of headache pain (0 = no pain, 1 = mild pain, 2 = moderate pain, 3 = severe pain). As recommended by the Clinical Trials Subcommittee of the International Headache Society (IHS) (26), we used complete freedom from pain within 2 h after the first drug dose for each attack as the criterion for drug efficacy, thus including all types of drugs taken within 2 h of the first dose in our estimation of drug efficacy.
Besides virtual communication, participants also had scheduled face-to-face contacts with the study leaders: at inclusion (approximately 2 h), for learning how to practice massage (approximately 1 h; massage subgroup only), and for the collection of blood samples on three to four occasions (approximately 5–10 minutes per occasion). Participants were also offered the opportunity to make unscheduled contacts via email or phone if felt necessary, though this was rarely practiced.
The MBT program only dealt with non-pharmacological interventions. Hence, participants had been instructed to continue their usual migraine medication as they wished, and could also undertake changes if they needed. An 8-week registration period, made before randomization and the start of MBT, was used as a baseline and the effects of MBT were evaluated during an end period comprising diary data from weeks 17–24 of the program or the same period for the control group.
The main outcome measures in the present study were: number of drug doses and drug efficacy measured as the ratio of migraine attacks in which the participant was pain-free within 2 h after the first drug dose. Other measures were: days with migraine headache, number of migraine attacks as defined by the IHS criteria (25), and change of drug intake after intervention. Differences in drug use and drug efficacy between women and men were also measured.
Ethical approval
The study was approved by the Regional Ethical Review Board, Uppsala, Sweden and all participants gave their informed consent to participate.
Drug use
The migraine drugs recorded in the diary were grouped into the following categories: triptans, analgesics, ergotamines, and ‘other’. Analgesics included acetylsalicylic acid and acetaminophen with or without caffeine or codeine, and non-steroidal anti-inflammatory drugs. The ergotamine group comprised ergotamine with or without chlorcyclizine. ‘Other’ migraine medication was represented by: chlorzoxazone with or without dextropropoxyphene, diazepam, oxazepam, and metoclopramide. The number of doses was recorded, but not the exact amount or routes of administration. If multiple doses were taken on the same day, including repeated doses of the same drug, the exact number of doses of the respective drugs was listed. Information about preventive medication was recorded at inclusion and subsequently any changes in preventive medication were registered. None of the participants fitted into the medication overuse headache category (headache on more than 15 days/month for more than 3 months or use of analgesics >15 days/month for >3 months or use of other migraine drugs >10 days/month for >3 months).
Statistics
For discrete parameters (gender, education, employment, presence of tension-type headache and aura, previous medical consultation, patterns of drug use and drug efficacy) differences in proportions between groups were analyzed using the chi-square test. For continuous parameters [body mass index (BMI), migraine frequency and time since migraine onset, drug doses], differences in the means between groups were examined using the Mann–Whitney U test and differences in age using the t-test. Differences in the number of drug doses over time within groups were compared using the Wilcoxon signed-rank test. All analyses were performed using the IBM Statistical Package for the Social Sciences (SPSS; Chicago, IL, USA) version 18.0 software. The significance level was uniformly set at p = 0.05.
Results
Demographics
Demographic profile and migraine characteristics at inclusion to the multimodal behavioral treatment (MBT) study (intervention group versus control group)
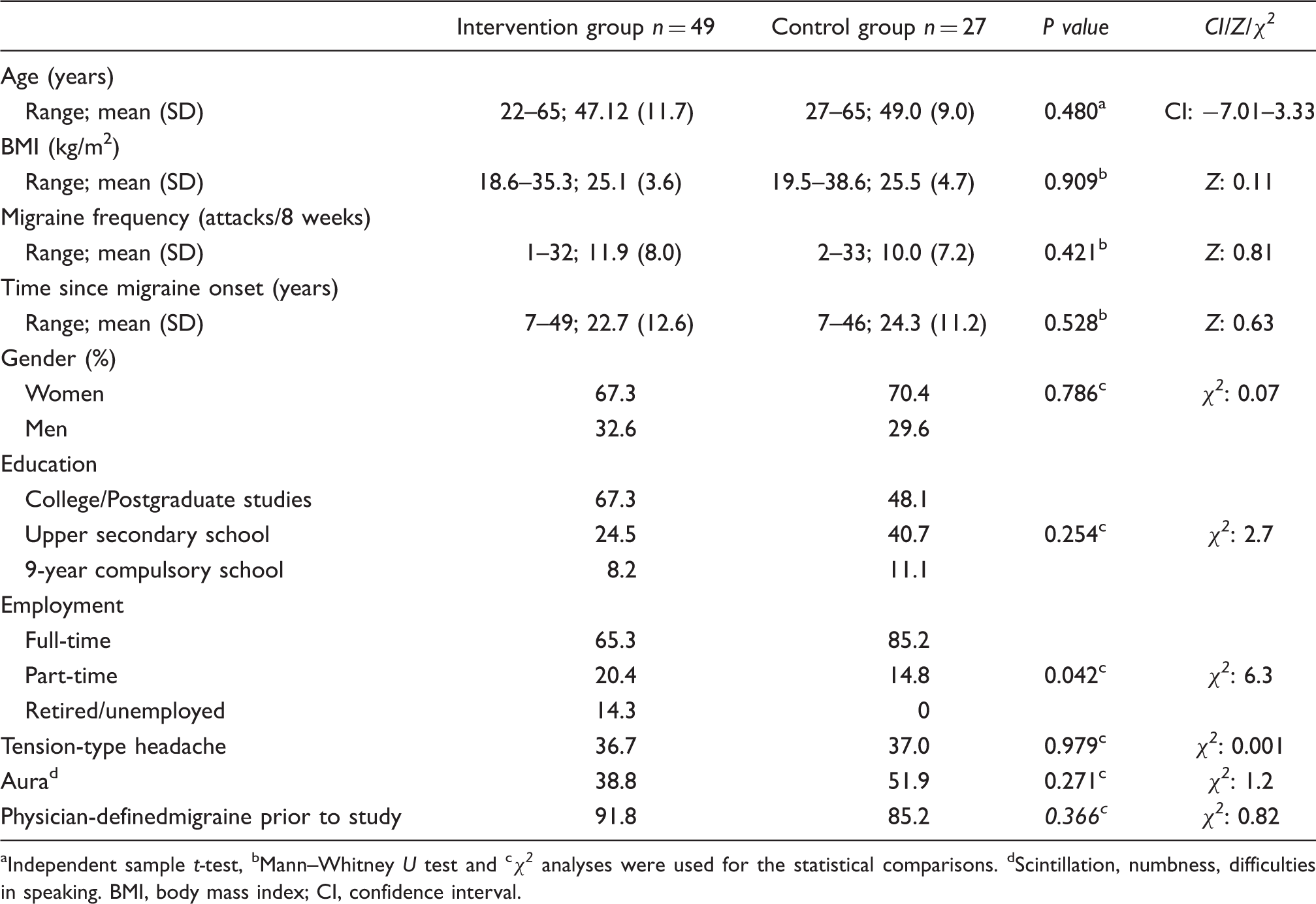
Independent sample t-test, bMann–Whitney U test and cχ2 analyses were used for the statistical comparisons. dScintillation, numbness, difficulties in speaking. BMI, body mass index; CI, confidence interval.
Migraine drug use during baseline registration
Migraine drug use in women and men before randomization to the multimodal behavioral treatment (56 days of baseline registration; women/men: n = 52/24)

Difference in the ‘average number of doses/migraine day’.
Chlorzoxazone with or without dextropropoxyphene, diazepam, oxazepam, and metoclopramide.
These numbers cannot be inferred from previous figures in the same column due to days of multiple drug use.
Days with migraine headache during which no acute migraine drugs were taken.
Proportion of participants which refrained from migraine drugs on at least one day with migraine headache.
CI, confidence interval.
Use of acute migraine drugs during all days with migraine headache at baseline and at the end of the multimodal behavioral treatment (MBT), separated by drug type or combinations thereof

T = triptan, A = analgesic, E = ergotamine, O = other (chlorzoxazone with or without dextropropoxyphene, diazepam, oxazepam, and metoclopramide).
Percentage of all migraine headache days with drug treatment, for the respective period.
Migraine medication during MBT
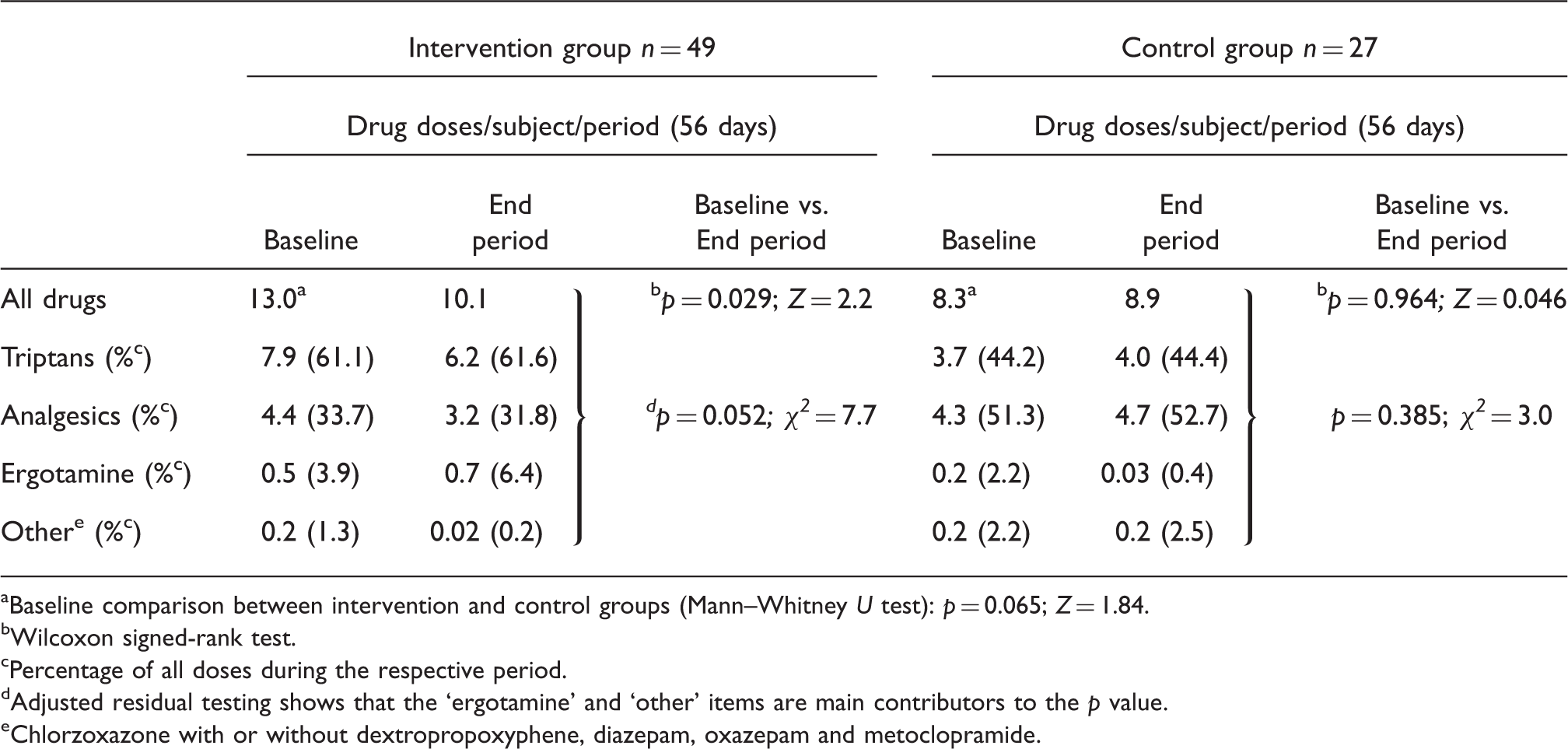
Changes in the amount and patterns of migraine drug use during the multimodal behavioral treatment (MBT) study
Drug type use during MBT
Use of preventive migraine drugs throughout the multimodal behavioral treatment study

Drug efficacy
Impact of multimodal behavioral treatment (MBT) on drug efficacy
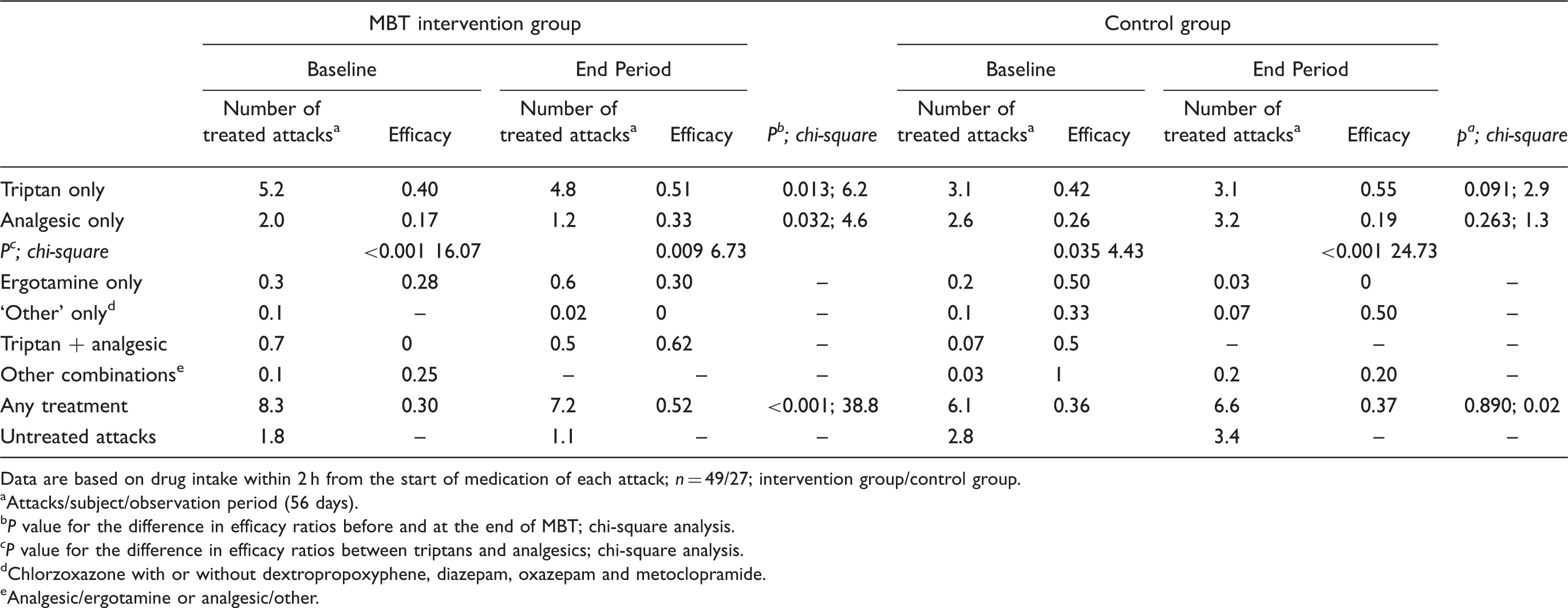
Data are based on drug intake within 2 h from the start of medication of each attack; n = 49/27; intervention group/control group.
Attacks/subject/observation period (56 days).
P value for the difference in efficacy ratios before and at the end of MBT; chi-square analysis.
P value for the difference in efficacy ratios between triptans and analgesics; chi-square analysis.
Chlorzoxazone with or without dextropropoxyphene, diazepam, oxazepam and metoclopramide.
Analgesic/ergotamine or analgesic/other.
When analyzing improvement in drug efficacy in relation to headache intensity, such improvement in the MBT intervention group was most pronounced for attacks registered as mild (baseline: 0.37 efficacy rate vs. end period: 0.58 efficacy rate; chi-square 10.5; p = 0.001). Statistically this was also reflected by a significant change in the pattern of pharmacological efficacy according to Pearson’s chi-square when analyzing for the three levels of headache intensity (chi-square 30.7; p < 0.001). Attacks with mild headache were responsible for this changed pattern: they constituted the only category in which the number of attacks was increased at the end of MBT. They increased from 134 to 150 attacks, while attacks with moderate headache decreased from 263 to 190 attacks and attacks with severe headache decreased from 102 to 65 attacks. Furthermore, mild attacks were the category with the largest increase in effective treatment (change in efficacy rate for attacks with mild headache: 0.37–0.58 vs. attacks with moderate or severe headache: 0.34–0.39 and 0.17–0.27, respectively). The improvement in drug efficacy for migraine attacks with mild headache was not associated with any significant change in the pattern of drug use (Pearson’s chi-square: 0.772, p = 0.680).
In the control group, no change in the pattern of pharmacological efficacy as a function of headache intensity was seen during the study (Pearson’s chi-square 4.5; p = 0.807).
Gender differences in drug efficacy
Gender differences in drug efficacy

Data are based on baseline registrations (n = 52 women/24 men) and on drug intake within 2 h from start of medication of each attack. The efficacy of ergotamine or ‘other’ migraine drugs, used singly or in combination with other drugs, are not listed because of their infrequent use but are included in the ‘All treated attacks’ item.
Attacks/individual/ study period (56 days).
Gender difference in efficacy.
Treatment effective in one attack only; p value not of interest.
Participants who refrained from drugs on at least one migraine headache attack.
Discussion
Drug use and drug efficacy
The present study describes the complete use of migraine drugs and their respective efficacy in a group of adult migraineurs with two or more migraine attacks per month as an inclusion criterion. To our knowledge, no prior published study has prospectively described drug intake in a migraine population over such an extensive time period. Triptans were the most frequently used and the most efficient drugs, with an efficacy rate of 0.41 at baseline, compared to 0.20 for analgesics, when used as single drugs.
This significant difference in efficacy between triptans and analgesics in the present study is in contrast to what Lipton et al. reported (27) in their review of double-blind studies on the efficacy of triptans versus different combinations of other drugs. Differences were ‘not dramatic’ in seven out of seven studies in which triptan efficacy was compared to that of analgesics. However, they concluded that this contradicts experience in clinical practice and may well be a result of study design – e.g. by using randomly selected migraineurs, starting medication at a higher symptom level and a 2-h end point. In contrast, a retrospective study by Malik et al. (24) showed efficacy rates similar to the present findings (triptans 0.51; analgesics 0.14–0.20) – a difference in efficacy that was also supported in a placebo-controlled study by Diener et al. (28), showing that the efficacy of sumatriptan was statistically higher than that of acetylsalicylic acid, with efficacy ratios of 0.37 and 0.27, respectively. Because our primary end point does not consider the benefit of partial effects or of later medication, it is likely that the efficacy rates obtained do not reflect the full benefits of acute medication for migraine.
Men displayed a lower efficacy of analgesics than women, which was not the case for triptans. This was paradoxical in view of the fact that, unlike women, men used more analgesics than triptans. There can be many different reasons behind men’s relatively low use of triptans which could be of interest to explore further. Our findings concerning gender-related drug use is well in accordance with the fact that women are more active in using drugs (29, 30), in particular concerning stress-related disorders such as headache (29).
Impact of MBT on drug use
We also studied to what extent effective MBT might influence migraine medication, and we believe that this is the first report in which the interaction of MBT on medication for migraine is described prospectively. One major finding was decreased overall drug consumption, which we judge to be a consequence of the positive effect of the MBT program leading to a decreased total number of migraine attacks and decreased total number of days with migraine.
It is notable that the number of migraine attacks with moderate and severe headache decreased considerably during MBT while the number of attacks with mild headache increased slightly. We also found that MBT resulted in significantly increased overall drug efficacy. When looking at drug efficacy as a function of headache intensity, the improvement was greatest for mild headache attacks. This, in combination with the increased proportion of mild attacks, provides a possible explanation for the improved overall drug efficacy at the end of MBT, as mild attacks are likely to be more susceptible to pharmacological treatment than more severe attacks. However, we were able to rule out the possibility that MBT participants switched over to more efficient migraine drugs when having mild attacks, as an explanation for the improved efficacy at end of the intervention.
Pharmacological treatment versus MBT
Although we lack precise data on the magnitude of symptom alleviation when using migraine drugs, we consider it of interest to estimate how this compares with the benefits of MBT (31): whereas drug treatment resulted in freedom from pain within 2 h in approximately one-third of the attacks, MBT resulted in a one-quarter reduction of days with migraine headache. Moreover, we describe an apparent interaction effect whereby MBT leads to greater drug efficacy. This demonstrates the need for both complementary behavioral-oriented therapies in migraine and more efficient drugs. We also believe that MBT has advantages over pharmacological treatment in that it results in greater empowerment of the individual – i.e. a greater feeling of being in control of the disease, and has fewer, if any, negative side effects.
Strengths and limitations
One major advantage of the present study is its prospective design, which made possible a detailed evaluation of the effects of a behavioral treatment program on drug use. The comprehensiveness and high quality of our diary data are also strengths. However, the validity of our findings for other migraineurs than those included in the present study may be open to debate, in view of their symptom level being above average at inclusion (two or more migraine attacks per month; 32). One weakness of the MBT intervention study is the lack of data on long-term effects. Also, despite our extra efforts to target men, the number of male MBT participants was too low to allow for analyses of gender differences with regard to the impact of such behavioral intervention on the use and efficacy of migraine drugs.
Conclusions
We conclude that, in the present settings, acute migraine drugs are used on approximately 75% of the days with migraine headache and that triptans are the most frequently used and the most efficient drugs. Furthermore, implementation of an MBT program, such as the one used in our study, leads to decreased overall drug consumption and less time with pharmacologically untreated headache. The efficacy rate of present migraine drugs is approximately one-third, but they seem to be more efficiently used after MBT, particularly in terms of migraine attacks with mild headache. Our data indicate significant gender differences, in that men used triptans less frequently and analgesics more frequently but with low efficacy.
In the future, more studies are needed to confirm and further characterize such gender differences in drug use, as well as the possibility of gender-dependent effects of the behavioral treatment of migraine. The presently shown synergy between drug treatment and MBT would also need to be independently confirmed. Extended studies are ultimately necessary to characterize the utility of an MBT program such as this with regards to the durability of its effects and its applicability on a larger scale via the Internet.
Footnotes
Acknowledgements
We are grateful for the valuable support from Dr Ulla-Maria Anderberg, Uppsala University, and the statistical assistance received from Hans Arinell, Uppsala University, and Karl-Erik Westergren, University of Gävle.
Funding
We are grateful for the financial support from the Erik, Karin, and Gösta Selander Foundation and from the Nursing Research Foundation, Faculty of Medicine and Pharmacy, Uppsala University.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.