
Abstract
Background: Migraine is considered a common but under-diagnosed and untreated condition. Treatment patterns have pointed at frequent over-the-counter medication use and low use of preventive therapies. Studies exploring migraine prescription practice among doctors are few.
Methods: A population-based study was carried out to examine the prescription practice in the use of acute and preventive migraine medications. The data covered 4864 working-age people reporting they have been diagnosed with migraine. Data on reimbursed prescription medicines from 1 January 1998 to 31 December 2006 were drawn from the registers of the Social Insurance Institute of Finland and compared with age- and sex-matched controls.
Results: Anti-inflammatory analgesics were prescribed for 71% of female and 62% of male migraine patients vs. 56% and 50% of controls. Triptans were prescribed for 21% of female and 10% of male patients. Combinations of analgesics and muscle relaxants were offered to 37% of female and 29% of male patients vs. 26% and 21% of controls, and antidepressants to 19% of women and 14% of men vs. 13% and 9% of controls.
Conclusion: Although use of preventive medication among migraineurs was high, the prescription patterns in acute treatments showed that NSAIDS were used more often than triptans. Assimilation of national guidelines to treat migraine published in 2002 in Finland was not reflected in the prescription patterns up to 2006.
Introduction
Migraine is a common (1) but under-diagnosed (2) and under-treated condition (3). Diagnostic criteria set by the International Headache Society (4) and evidence-based guidelines based on randomised clinical trials (5) instruct to optimise migraine care.
Migraine is a heterogeneous headache disorder which is more painful and of longer duration than other types of common headaches (6). Although most migraineurs report moderate or severe pain during attacks (7), treatment patterns point at high use of over-the-counter (OTC) attack medications and low use of preventive therapies (3).
The prevalence of migraine is 25% among women and 11% among men in Finland (8). As elsewhere, it constitutes a burden especially on the working age population (8,9). Acute migraine medications such as triptans, ergotamines and stronger painkillers, as well as prophylactic medications, are available on prescription only. The Finnish Social Insurance Institution (SII) reimburses part of prescribed medications (10), which allows a population-based register study on reimbursed migraine medication among working-age migraine patients. This information is assumed to reflect the current treatment policy of migraine in the working-age population.
National treatment guidelines were first published in 2002 and revised in 2008 (11,12). In this study, we focused on temporal changes in migraine medication prescription practices among doctors, which is rarely addressed (13). Our specific aim was to evaluate the association of national guidelines on physicians’ prescription practices for both abortive and preventive migraine medication.
Materials and methods
Study population
The Health and Social Support Study (HeSSup) is a prospective aetiological follow-up study on the psychosocial health of the Finnish working-age population. The HeSSup population comprised a random sample of 64,797 individuals drawn from the Finnish Population Register consisting of four age groups: 20–24, 30–34, 40–44 and 50–54 years. The survey was carried out by a postal questionnaire in 1998. Altogether 25,895 forms were returned (response rate 40%). A follow-up questionnaire (response rate 76%) was sent in 2003 to all those who responded to the first inquiry.
Using the official statistics on the Finnish population for the corresponding age groups in 1998, the sample was subjected to a thorough analysis of non-response (9) to assess whether the study cohort adequately represented the Finnish population. The conclusion was that differences in physical health between participants and the general population were small.
Method
All participants were asked whether a doctor had told them they have or had migraine (14,15). Migraine was thus self-reported. Those responding affirmatively in 1998 were regarded as migraine patients (N = 4864). Registers of SII were used to study reimbursed medications between 1998 and 2006 in the study population (10). The national guidelines for migraine treatment in the Finnish Current Care Summary were first implemented in September 2002. We therefore analysed the prescriptions of abortive and preventive migraine drugs before and after the implementation. The first study period covered the years from 1998 to 2002, and the second the years from 2003 to 2006.
ATC codes of the prescribed abortive and preventive migraine medicines and oestrogens

Analyses were carried out using the SAS System for Windows, release 8.2. The statistical significance of frequency distributions was tested by the chi-squared test.
In the logistic regression analysis, odds ratios (OR) with 95% confidence intervals (CI) were calculated for the prescriptions of medications. Because the analysed medications are also used for indications other than migraine, the regression analyses were made adjusting for specific diseases, also self-reported. With respect to mild opiates, adjustment was made for osteoarthritis and sciatic syndrome. Antidepressant prescriptions were adjusted for depression and antiepileptic prescriptions for epilepsy. Beta blocker prescriptions were adjusted for hypertension, coronary heart disease and atrial fibrillation. In order to obtain the best available comparison group, one randomly selected age- and sex-matched control was selected for every migraine patient. Those selected as controls had responded negatively to inquiries about migraine diagnosis in questionnaires in 1998 and 2003.
Results
Age distribution of migraine patients in 1998

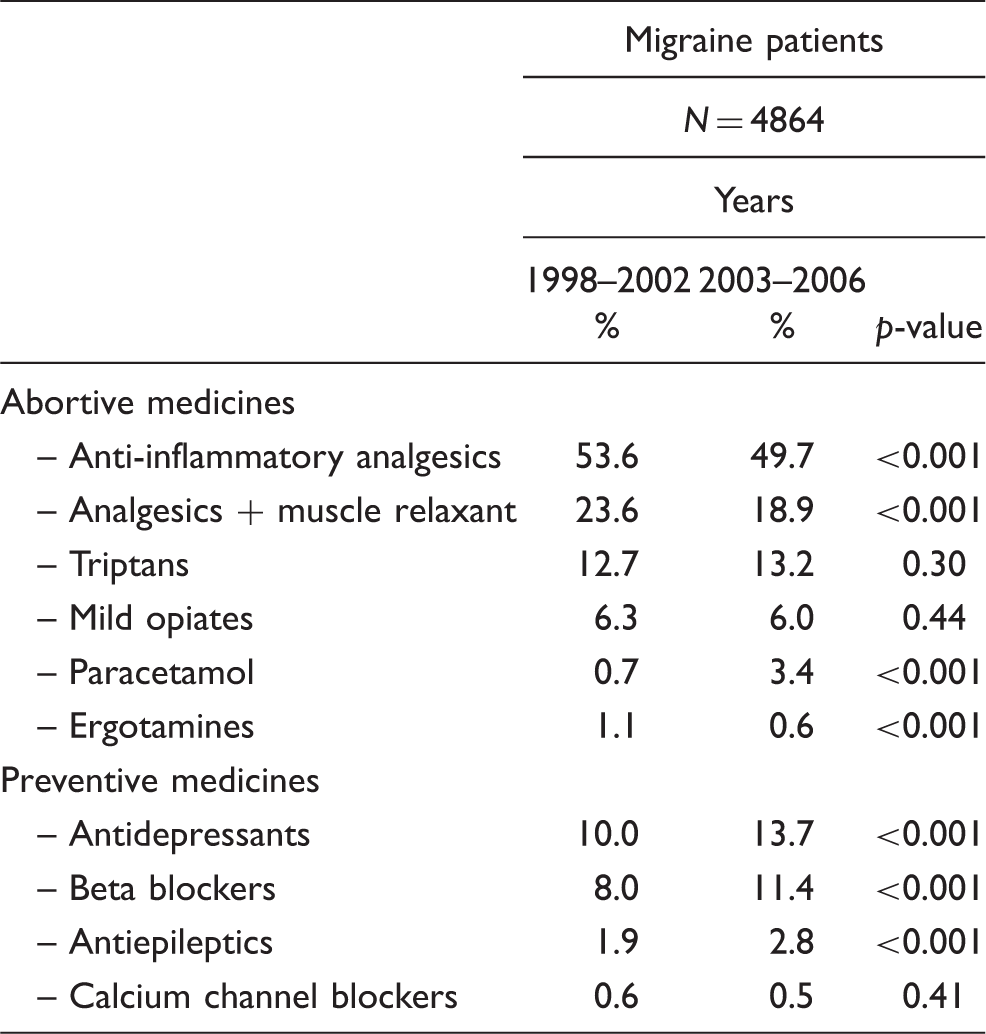
Prescription of abortive and preventive migraine drugs before and after the implementation of the Current Care Summary in 2002 [proportion (%) of migraine patients having used these drugs]
Conditional univariable logistic regression analysis (OR with 95% CI) of medicine prescription among working-age migraine patients compared with their age-matched controls

Conditional multivariable logistic regression analysis (OR with 95% CI) of medicine prescription among working-age migraine patients compared with their age- and gender-matched controls (adjusted for specific diseases)

Covariates: osteoarthritis and sciatic syndrome.
Covariates: depression (Beck > 18).
Covariates: epilepsy.
Covariates: hypertension, coronary heart disease and atrial fibrillation.
Discussion
Several guidelines aim at improving and unifying the care of migraine patients (4,5). At present we have little knowledge of their impact on treatment policies in populations (3,13). We studied the assimilation of national guidelines published in 2002 by exploring prescriptions from the Finnish Social Insurance Institution’s data, as it reimburses part of prescription medications for every Finnish citizen. Although migraine was self-reported in our material, and may thus underestimate true prevalence (16), migraine recognition among patients is generally regarded as fairly reliable (17,18). Migraine prevalence in our working-age study cohort was similar to that in the age-matched Finnish population (8).
During the 8-year follow-up from 1998 to 2006, prescriptions for preventive migraine medications showed significantly high ratios and increase during 2003–2006. The most frequently used therapies were beta blockers and antidepressants in our study also (19). Adjustment of beta blockers for cardiovascular diseases (cvd) had no further influence on the results, accounting for their shift towards older age groups (20). After adjusting for the other reported comorbid conditions, there was still a significant and almost two-fold likelihood of antidepressant, antiepileptic and hypertensive drug prescriptions among migraineurs. Results accord well with the preventive treatment recommendations and current conception of their benefit (4,5,11,12,21,22). The American Migraine Prevalence and Prevention study (AMPP) (3) showed that a substantial proportion of migraineurs who might benefit from prevention do not receive it. As we lack information on diagnostic verification for prescriptions, migraine severity, and length and efficacy of medications, we are unable to replicate the results of the AMPP study. Our results suggest physicians’ vigilance for prescribing preventive migraine medication according to the recommendations.
We observed no temporal change in triptan prescriptions and the prescription rate corresponds to results in other studies, ranging from 13 to 19% (23). Although NSAID prescription decreased significantly, they were the most commonly prescribed abortive medication. Several reports indicate that half of migraine sufferers treat their disorder exclusively with OTC drugs (24,25) and prescription medication use is lower (13). As we studied only reimbursed attack medications, there are shortcomings for drawing any solid conclusions on actual attack treatments with NSAIDs and paracetamol in Finland. Our observations show that painkillers and mild opiates are also prescribed for migraineurs, although the trend was slightly decreasing. Prescriptions may point at pain conditions other than migraine or classification of attacks to tension-type headache or combination headache. High rates of opioid use and combinations of analgesic/muscle relaxants have been observed elsewhere (26–28). Results here indicate that NSAIDs are preferred in migraine treatment by physicians, and triptan use has remained low up to 2006.
We have shown that monitoring of prescription patterns is a useful tool to evaluate changes in the practise of migraine treatment. According to our results, the association of operational guidelines for migraine treatment are more pronounced for prescribing prophylactic medications than attack treatments. Results indicate that national guidelines for migraine treatment have a significant impact on physicians’ prescription practices. We conclude that guidelines for migraine diagnosis and treatment are useful and require vigilance among doctors.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.