
Abstract
Background: Dihydroergotamine (DHE), a proven migraine treatment, currently has product labeling warning against concomitant use of CYP3A4 inhibitors because of potential drug interactions. However, no reported studies of such interactions with DHE administered by any route are available.
Methods: The pharmacokinetics (PK) of MAP0004, an investigative inhaled DHE formulation, were assessed in human subjects with and without CYP3A4 inhibition by ketoconazole to evaluate the potential for drug interaction, elevation of DHE levels, and increased adverse effects.
Results: After MAP0004 alone vs. MAP0004 plus ketoconazole, the DHE maximum concentrations (Cmax) and area-under-the-curve (AUC0–48 and AUC0–∞) were not statistically significantly different nor was the Cmax of the primary metabolite, 8’-OH-DHE. A difference in 8’-OH-DHE AUCs was observed between MAP0004 with and without ketoconazole; however, the concentrations were very low. MAP0004 was well tolerated after both treatments.
Conclusions: This study demonstrated that CYP3A4 inhibition had little to no effect on DHE PK after MAP0004 administration, apparently because of its high systemic and low gastrointestinal bioavailability. CYP3A4 inhibition slowed elimination of the metabolite 8’-OH-DHE, but concentrations were too low to be pharmacologically relevant.
Introduction
Dihydroergotamine (DHE) has been used successfully to treat migraine headaches for over 60 years (1,2), but the published research on its pharmacokinetics (PK) is decades old and incomplete due to the constraints of analytical methodology at that time. In the early 1980s, researchers attributed the very low bioavailability of orally administered DHE to high first-pass metabolism (3) and conversion to the active metabolite 8’-OH-DHE (4), later clarified to occur through liver CYP3A4 metabolism (5). Concern over potential drug interactions with potent CYP3A4 inhibitors such as macrolide antibiotics and protease inhibitors (6,7) and case reports of apparent drug interactions with clinical sequelae (8,9) contributed to the establishment of labeling warning against concomitant use of those medications with DHE. Over time other routes, including intravenous (IV), subcutaneous, intramuscular and intranasal, were utilized more frequently than oral administration of DHE; however there are few studies that establish the metabolism and potential drug interactions of DHE administered through these routes. Therefore, the currently marketed products, injectable DHE and intranasal DHE, retain these precautions in the form of ‘black box’ warnings in their labels (10,11), but no published study has documented such drug interactions.
A new product under development, MAP0004 (LEVADEX™, MAP Pharmaceuticals, CA, USA), delivers orally inhaled DHE through the lungs to the systemic circulation via the TEMPO® inhaler, a breath-synchronized, plume-control inhaler designed to offer consistent, convenient and non-invasive dosing (12). Administration of MAP0004 at the 1.0 mg nominal dose level results in rapid DHE systemic availability (10 minutes to maximum plasma concentration) with a maximum plasma concentration (Cmax) of 2302 pg/mL, 25-fold lower than that observed after IV DHE 1.0 mg (13) and sufficient for potent agonist action at key anti-migraine 5-HT1B and 5-HT1D receptors (14). The systemic concentrations of 8’-OH-DHE, on the other hand, were low after MAP0004 administration (15,16), suggesting that the 1.0 mg dose undergoes minimal first-pass metabolism and that the metabolite contributes little to the pharmacologic activity of MAP0004. We conducted this study to assess the impact of CYP3A4 inhibition on DHE PK after MAP0004 dosing by administering MAP0004 before and concomitant with the potent CYP3A4 inhibitor, ketoconazole, in healthy volunteers. Additionally, we compared MAP0004 PK to that of the standard dose of IV DHE (1.0 mg) and evaluated the safety and tolerability of the three treatments. Our objective was to assess whether the PK of DHE administered by MAP0004 was significantly affected by CYP3A4 inhibition and to compare the concentrations observed to those seen after IV DHE administration.
Methods
Study design and treatments
This was an open-label, single-center study (NCT01468558, registered in clinicaltrials.gov after completion) comparing the tolerability and PK of a single dose of MAP0004, an orally inhaled formulation of dihydroergotamine mesylate (DHE, 1.0 mg nominal dose), with and without co-administration of ketoconazole, and IV DHE. The study was approved by institutional review boards and conducted according to Good Clinical Practice and International Council on Harmonization guidelines and the Declaration of Helsinki. The study was conducted from July to September 2010 at Simbec Research Limited in the UK.
One to 21 days following a screening visit to determine eligibility, subjects returned to the clinic for an 8-day inpatient visit (Figure 1). On Day 2, subjects received a single dose of MAP0004 (8:30 am) with blood sample collection over 48 hours, followed by four daily doses of 400 mg ketoconazole on Days 3 to 6 (8:30 am), followed by another single dose of MAP0004 on Day 6 (9:30 am) with blood sample collection over 48 hours. After a washout period of 7–11 days, subjects returned to the clinic to receive IV DHE (8:30 am) with blood sample collection over 48 hours, and after another 7–11 days of washout they returned for a final study visit.
Study design and treatments.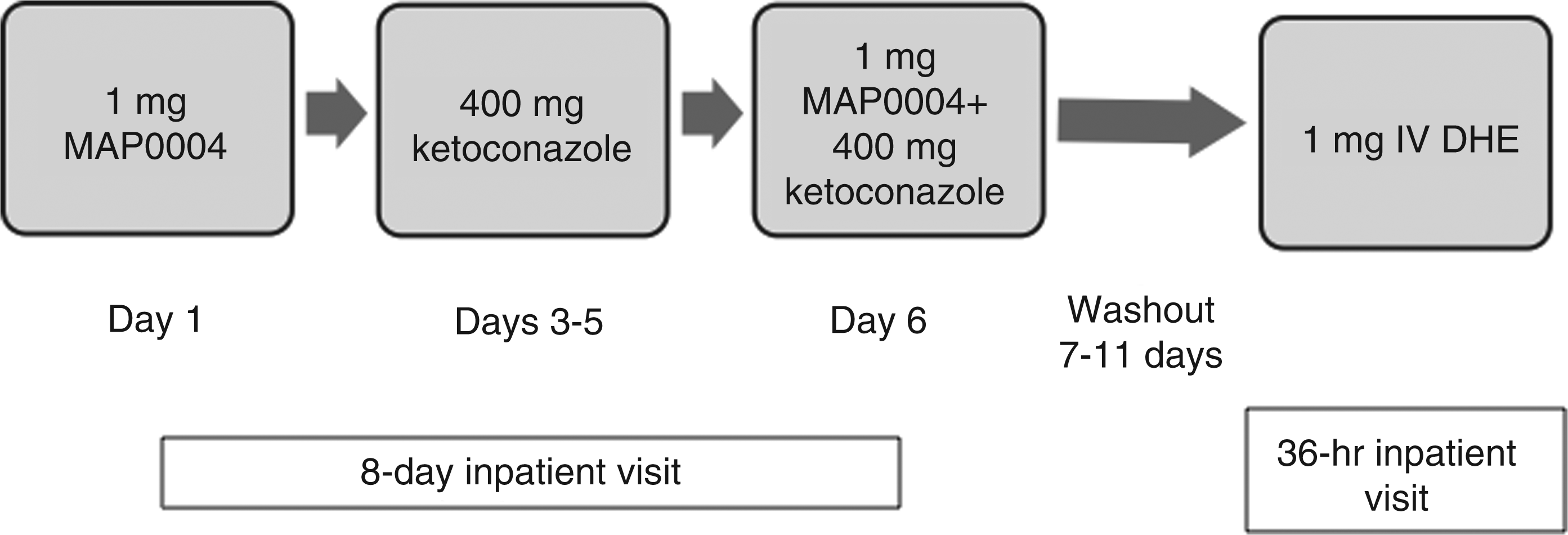
MAP0004 is a formulation of DHE suspended in a blend of hydrofluoroalkane propellants delivered with the TEMPO® Inhaler (MAP Pharmaceuticals Inc., CA, USA), two actuations of which provide a nominal dose of 1.0 mg and emitted dose of 0.63 mg DHE, a dose chosen for MAP0004 development based on a Phase 2 dose-ranging study. Ketoconazole 400 mg was administered orally as two 200 mg tablets over 4 days, a regimen known to strongly inhibit CYP3A4 metabolism (17). Intravenous DHE (IV DHE 45, Valeant Pharmaceuticals, NC, USA) 1.0 mg, the approved dose for the acute treatment of migraine, was delivered by infusion over 60 seconds.
Subjects were prohibited from using ergot-containing drugs and triptans during the study as well as CYP3A4 inhibitors, including macrolide antibiotics, protease inhibitors, quinidine, aripiprazole, glyburide, calcium channel blockers, statins, immune modulators, nefazodone, nitrates, pimozide, quinine, rifabutin, PDE-5 inhibitors and tamoxifen.
Subjects
The study was conducted in healthy non-smoking male and female volunteers 18–45 years of age recruited from the Simbec database of healthy volunteers. Participants gave written informed consent prior to entry. Female subjects were recruited in a 2:1 ratio to males because of the higher incidence of migraine among females; they were not pregnant or breastfeeding, and all were using acceptable birth control methods, were abstinent, or not of childbearing potential. Subjects had normal and stable cardiac status (heart rate ≥ 40 and ≤ 100, QTcF ≤ 450 ms, normal rhythm). Subjects did not have a diagnosis of cancer; recent major surgery; known allergies or contraindications to study drugs; clinically significant liver or kidney disease; predefined risk factors for coronary artery disease (CAD); history of hemiplegic or basilar migraine, unstable psychiatric illness, CAD, chronic obstructive pulmonary disease, bronchospasm with inhaled medications, cerebral vascular accident, transient ischemic attacks, or seizures; recent hospitalization for a concurrent illness; or recent radiation exposure. Subjects had not used excluded concomitant medications within the last 10 days.
Study assessments
At screening, subjects underwent a medical history, physical examination, clinical laboratory tests, urinalysis, screens for illicit drugs, pregnancy test, chest X-ray, 12-lead ECGs, as well as receiving inhaler training.
For each of the two inpatient treatment visits, subjects checked in the evening before initial study drug administration, at which time subjects again had a pregnancy test, drug screen, and inhaler training. Adverse events and vital signs were monitored continuously. Prior to MAP0004 or IV DHE dosing and after a 12-hour fast at either inpatient visit, subjects underwent a 12-lead ECG, inhaler training, blood sample collection for clinical laboratory tests, blood sample collection for DHE levels, and urine collection. After MAP0004 or IV DHE dosing, 6 mL blood samples for DHE PK analysis were collected with the following schedule: 0 minutes (immediately post dose), 5, 10, 15, 30, 60, 90 minutes and 2, 3, 4, 6, 12, 24 and 48 hour post dose. 12-lead ECGs were administered again at 10 and 60 minutes post dose.
On Day 2 of the first (8-day) inpatient visit, subjects received orally inhaled MAP0004. On Days 3–5, subjects received ketoconazole 400 mg daily, after which vital signs and adverse event assessments were conducted twice daily, and a 12-lead ECG was performed 1 hour post dose. On Day 6, subjects received ketoconazole 400 mg followed by inhaler training, and vital signs, 12-lead ECG, blood sample collection for clinical laboratory tests, blood sample collection for DHE levels, and urine collection were conducted. One hour after ketoconazole dosing, subjects administered MAP0004. A physical exam was performed at 24 and 48 hours post dose.
Subjects returned to the clinic after a washout period of 7–11 days for a 36-hour inpatient visit to receive IV DHE with blood sample collection over 48 hours. After discharge and another 7–11 day washout period, a follow-up visit was conducted, at which time subjects had clinical laboratory tests, physical exam, pregnancy testing, vital signs, and a final assessment of adverse events and concomitant medications.
Bioanalytical methods
Bioanalytical analysis of the plasma samples for DHE and its primary metabolite, 8’-OH-DHE, was conducted at Simbec. Plasma drug levels were measured using a validated liquid chromatographic tandem mass spectrometric (LC-MS/MS) procedure in turbo ion spray positive ionization mode. Following extraction from plasma, LC-MS/MS analysis of the extracts was performed with multiple reaction monitoring. The lower limits of quantification (LLQ) in the DHE and 8’-OH-DHE assays were 10 pg/mL and 20 pg/mL, respectively.
Statistical analysis
The primary objective was to compare the PK parameters Cmax and area under the plasma concentration versus time curve (AUC0–48 and AUC0–∞) for DHE and 8’-OH-DHE when MAP0004 was administered with and without ketoconazole. In addition, time to maximum concentration (Tmax), elimination half-life (t1/2), clearance (CL), volume of distribution (Vd), and bioavailable fraction of nominal dose (F), were evaluated. Safety was assessed based on treatment-emergent adverse events, clinical laboratory studies, vital signs, and ECGs.
A repeated-measures analysis of variance (ANOVA) model with treatment as the repeated measures factor was conducted to test for differences in Cmax, AUC0–48 and AUC0–∞ using log-transformed values with p-values reported at the 0.05 level. Geometric mean ratios and 90% confidence intervals (CI) were calculated using fixed effects for gender, and the hypothesis that the geometric mean ratio was equal to 1 was tested (18). All PK parameters were summarized descriptively.
The safety population comprised all subjects who received at least one dose of study drug. The PK population comprised all subjects who received at least one dose of study drug and who provided adequate PK samples. The sample size (18 completed subjects) was based on FDA guidance for detecting a treatment effect in drug–drug interaction studies (18) and previously published studies evaluating CYP3A4 inhibition and the potential for drug–drug interactions (19,20). A total of 24 subjects were enrolled to achieve a sample size of 18 completed subjects.
Results
Subjects
Of the 38 subjects screened for this study, 24 were enrolled who averaged 29.6 (± 8.3) years old, weighed 73.8 kg (± 12.9), and had a BMI of 25.9 (± 3.8) kg/m2. Two-thirds (18/24) were female, and the majority were Caucasian (22/24). Twenty-two subjects completed all study visits, treatments and procedures, and two were withdrawn. One subject was withdrawn for adverse events (skin irritation and pruritus) on Day 6 following ketoconazole treatment and prior to receiving the second dose of MAP0004 and IV DHE. One subject was withdrawn prior to receiving IV DHE due to a positive drug test.
Pharmacokinetics of DHE
Twenty-three subjects who received MAP0004 before or after ketoconazole and 22 subjects who received IV DHE had evaluable data and were included in the overall PK population. For all treatments, the number of samples per time point and consequently for some parameters varied due to measurements that fell below the levels of LLQ and a few missed samples.
The mean plasma semi-logarithmic concentration–time profiles for DHE after MAP0004 administration (before and after ketoconazole treatment) and for IV DHE are shown in Figure 2A (0 to 48 hours) and 2B (0 to 2 hours). The concentration–time profile after administration of MAP0004 alone was similar to that after administration of MAP0004 and ketoconazole in combination. Administration of DHE by the IV route, on the other hand, immediately resulted in dramatically higher plasma levels of DHE with a rapid reduction over time that paralleled that of MAP0004 but continued to remain higher throughout the 48-hour period. A subject-by-subject display of plasma DHE Cmax shows that no subject had a markedly increased peak plasma DHE concentration following ketoconazole co-administration (Figure 3).
Mean plasma parent DHE concentration–time profile of IV DHE and MAP0004 (alone and in combination with ketoconazole) on a semi-logarithmic scale: PK population. (A) Concentration vs. time profile over the 48-hour post-treatment period. (B) Concentration vs. time profile expanded for the first 2 hours post-treatment. Individual subject plasma DHE Cmax after MAP0004 administration alone and in combination with ketoconazole.

Summary of PK Parameters, Geometric Mean (Geometric % CV) DHE and 8’-OH-DHE

Only two metabolites were detected at concentrations above the LLQ, 8’-OH-DHE and dihydrolysergic acid amide (DHLSA). The major DHE metabolite, 8’-OH-DHE, was present in concentrations approximately two magnitudes lower than DHE, while its concentration–time profile indicated formation rate-limited kinetics. The Cmax of 8’-OH-DHE after MAP0004 alone was similar to that after MAP0004 with ketoconazole but low compared with maximum concentrations of 8’-OH-DHE after treatment with IV DHE (Table 1). Compared with levels of DHE, the levels of 8’-OH-DHE were very low, with a Cmax geometric mean ratio of 2.7% after MAP0004 alone. Following MAP0004 with ketoconazole treatment, AUC0–48 and AUC0–∞ levels of 8’-OH-DHE were significantly higher than after MAP0004 alone and similar to the levels seen after IV DHE treatment. Mean t1/2 for 8’-OH-DHE was similar to that for DHE for all treatment groups, although sample size was particularly low (n = 3) for the MAP0004 alone group due to the small number of samples above the LLQ.
Assessments of drug interactions
Geometric LS mean ratios (90% CI)

Safety
Treatment-emergent adverse events (TEAE)

Events reported by ≥ 3 subjects in a treatment group.
There were no clinically significant changes in laboratory parameters during the study; no out of range value was clinically significant. There were no clinically significant findings in physical examinations, ECGs or vital signs. Administration of MAP0004, MAP0004 with ketoconazole or IV DHE did not increase systolic or diastolic blood pressure.
Discussion
The results of this study provided evidence that CYP3A4 inhibition has little to no effect on DHE elimination following MAP0004 administration at the dose of 1.0 mg selected for product development. The systemic levels of DHE after MAP0004 co-administered with the potent CYP3A4 inhibitor, ketoconazole, were similar to those observed after the administration of MAP0004 alone, reaching a Cmax of approximately 2500 pg/mL at approximately 10 minutes with similar AUC and t1/2. Thus, there appears to be no potential to enhance or prolong DHE levels if MAP0004 were used concurrently with CYP3A4-inhibiting drugs, such as protease inhibitors or macrolide antibiotics. To our knowledge, this is the first human study to evaluate the effect of CYP3A4 inhibition on DHE administered by any route. These results, however, cannot be extrapolated to other routes of administration, including intranasal, subcutaneous, intramuscular and oral.
Levels of DHE metabolites were found to be very low after MAP0004 administration with and without ketoconazole, with only the active metabolite, 8’-OH-DHE, and DHLSA present in concentrations above the LLQ. The Cmax of 8’-OH-DHE was 80 pg/mL after MAP0004 plus ketoconazole, statistically indistinguishable from that after MAP0004 alone. The low levels of 8’-OH-DHE detected after MAP0004 alone or IV DHE treatment were similar to those observed in previous studies (15,16) and too low to be pharmacologically relevant (14). Metabolite levels represented less than 3% of plasma DHE after MAP0004 inhalation, most likely because of the limited amount of gastrointestinal and hepatic first-pass metabolism due to absorption through the lungs. In comparison, metabolite levels are reportedly 20–30% after intranasal administration (11). In the current study there was an apparent effect of CYP3A4 inhibition on elimination of 8’-OH-DHE, as indicated by elevation in AUC0–48 and AUC0–∞ and prolongation of the time to maximum concentration, presumably because of delayed metabolism of 8’-OH-DHE.
All treatments were well tolerated in the current study. There were no clinically significant changes in clinical laboratory evaluations, ECGs or physical examinations and no increases in systolic or diastolic blood pressure, a known side effect of IV DHE (10). The highest incidence of adverse events, severe adverse events, and drug-related adverse events was observed in the IV DHE group, the most frequent of which was nausea, consistent with previous reports (15,21). Using a series of receptor-based mechanistic studies, Cook et al. concluded that the maximum DHE concentrations following MAP0004 administration were insufficient to interact with receptors implicated in cardiovascular and pulmonary effects, whereas the concentration seen after IV DHE had agonist effects at those receptors (14). While there were modest effects of IV DHE on blood pressure in the current study, a recently conducted placebo-controlled study demonstrated that IV DHE raised pulmonary arterial systolic pressure significantly compared with MAP0004, which was indistinguishable from placebo, leading the authors to conclude that MAP0004 may be therapeutically preferable in terms of cardiac safety (13). The safety of inhaled MAP0004 has also been confirmed in asthmatics, in whom the PK profile of DHE was comparable to that of healthy volunteers (22).
This study had important limitations. First, the study did not include a treatment arm combining IV DHE with ketoconazole, and was not intended to assess the possible effects of CYP3A4 inhibition on the intravenously administered drug. Also, the study did not determine the route of elimination for DHE or its metabolites, nor did it explore potential sites of metabolism of DHE. Finally, these results were obtained from healthy volunteers instead of patients with migraine, wherein some differences in metabolic processes are possible.
The inhaled route administration of DHE appears to provide advantages over other routes, including the lack of significant CYP3A4 drug interactions. In addition, MAP0004 uses a unique inhaler that is convenient, non-invasive, and offers precise and consistent dosing. The low throat deposition and increased fine particle fraction (12) probably contribute to the rapid and high systemic availability.
Conclusion
The results of this study provided evidence that CYP3A4 inhibition has little to no effect on DHE PK after MAP0004 administration; the systemic levels of DHE after MAP0004 co-administered with the potent CYP3A4 inhibitor, ketoconazole, were similar to those after administration of MAP0004 alone. CYP3A4 inhibition may slow metabolism and elimination of 8’-OH-DHE, however, levels of the active metabolite remained very low and unlikely to be pharmacologically important. Thus, there appears to be minimal clinical risk of enhancing or prolonging DHE levels if MAP0004 were used concurrently with CYP3A4-inhibiting drugs, such as protease inhibitors or macrolide antibiotics, and no evidence for label warnings. Administration of DHE by other routes should be similarly evaluated for drug interactions.
Footnotes
Acknowledgements
PK and statistical analysis was performed at Simbec Research. The authors thank the study personnel at Simbec and MAP Pharmaceuticals as well as the subjects who participated in the trial. In the preparation of the manuscript, authors were assisted by a professional medical writer, Elizabeth Field, PhD, of Field Advantage Medical Communication, LLC, who was funded by MAP Pharmaceuticals.