
Abstract
Background: The association between migraine and obesity gives the clinician with an exciting possibility to alleviate migraine suffering through weight-reduction gastric-restrictive operations. We hypothesized that bariatric weight-reduction intervention (gastric banding) will be associated with reduction of migraine burden in this population.
Methods: A total of 105 women between 18 and 50 years of age, admitted for bariatric surgery between April 2006 and February 2007, were screened for migraine. Twenty-nine with diagnosis of migraine were enrolled into the prospective phase. We followed the migraine pattern of these patients for 6 months post bariatric surgery.
Results: Baseline median migraine frequency was six headache days a month. Post bariatric surgery, the migraine-suffering women reported of a lower frequency of migraine attacks (p < 0.001), shorter duration of the attacks (p = 0.02), lower medication use during the attack (p = 0.005), less non-migraine pain (44.8 vs. 33%, p = 0.05), and post-bariatric surgery reduction in headache-related disability assessed by the MIDAS and HIT-6 scores. There was a reduction in migraine frequency among both episodic (from four to one episodes a month) and chronic (from 16.8 to 8.5 episodes per month) migraine patient cohorts separately and combined.
Conclusions: Among migraine-suffering premenopausal obese women, we found a reduced frequency of migraine attacks and improvement of headache-related disability post bariatric surgery. Our findings should be interpreted cautiously. The absence of a control group and the non-blinded nature of our small study make it difficult to draw firm conclusions about the causal nature of the headache changes observed in this population. Further study is needed to evaluate the possible specific effects of surgical weight loss on migraine in obese women.
Introduction
Migraine is a common neurovascular condition, often resulting in severe impact on the suffering individual (1). Epidemiological links between migraine and obesity have emerged during the last few years and have been recently reviewed (1). There are conflicting data in large population databases regarding the association between migraine and obesity; however, all of the large population databases evaluating migraine patterns at reproductive age suggest there is an association between episodic migraine and obesity (2–5). Furthermore, obesity is associated with the transformation of episodic migraine to chronic migraine (3).
During the last years, our clinical impression was that among candidates for bariatric surgery there are a large proportion of morbidly obese female patients who suffer from migraine. Horev et al. (6) found, in a small series of patients, 48% higher incidence of migraine among morbidly obese population. This observation was supported by the report of Peres et al. (7) in which migraine was reported by 66% of obesity clinic patients as compared with 18.5% of non-obese controls. Other studies have revealed the correlation between obesity and migraine among women and men of reproductive age (6) and also among adolescents (2).
The link between migraine and obesity faces the clinician with an exciting possibility to alleviate migraine through weight reduction. As the prevalence and severity of obesity rise, so has the acceptance of increasingly aggressive remedies such as the use of bariatric surgery (8). Gastric-restrictive operations, such as gastric banding and vertical banded gastroplasty, cause weight loss by limiting the capacity of the stomach to accommodate food and by slowing the flow of ingested nutrients (9,10). Many obesity comorbidities such as diabetes and hypertension have been shown to improve or even be cured following such interventions (11).
We hypothesized that bariatric weight-reduction intervention (gastric banding) is associated with reduction of migraine burden in this population.
Methods
Study population
A total of 105 consecutive women between 18 and 50 years of age, admitted to the surgical department of the Soroka University Medical Center for bariatric surgery between April 2006 and February 2007 were screened for migraine. All participants were interviewed using a structured questionnaire which focused on headache events in the past and during the last 3 months prior to interview. The interview was conducted during the 14 days prior to the scheduled surgical procedure. Women who reported headache attack during the past 3 months were further investigated on headache characteristics and accompanying features. A diagnosis of migraine with or without aura was made according to the International Classification of Headache Disorders II (ICHD-II) (12) by a neurologist.
All the patients who were diagnosed as suffering from episodic and chronic migraine with or without aura were included. Participants who suffered from any neurological condition except headache or who had sustained a head injury during the previous year were excluded. No other comorbidities or pain syndromes were a reason for subjects’ exclusion. Since a reliable assessment of medication-overuse headache was not possible, patients with medication-overuse headache were not excluded.
The patients were informed of the study design and rationale and signed an informed consent. The study was approved by Soroka University Medical Center ethical committee.
Study conduct
The study was designed to prospectively follow the migraine pattern for 6 months post bariatric surgery among migraine-suffering morbidly obese women.
Demographic, biometric (specifically height and weight), and medical data were collected from the patients’ medical records when they were recruited. Weight and height were recorded as measured by the admitting surgery department using the same equipment (scales and stadiometer) for all the subjects. The follow-up weight at 3 and 6 months following surgery was self reported.
Migraine severity assessment
Migraine severity was assessed using three parameters, the Headache Impact Test (HIT-6), the Migraine Disability Assessment Scale (MIDAS), and headache frequency.
The HIT-6, a six-question survey, was used to measure the impact of headache on respondents’ lives. The questionnaire cover six aspects of functioning fields that most commonly being influenced by headache: pain, role of functioning (the ability to carry out usual activities), social functioning, energy or fatigue, cognition, and emotional distress (13).
The MIDAS scale is used to quantify headache-related disability (14). MIDAS is a brief and reliable headache-specific tool which captures headache-related disability. Five questions investigate the influence of headache on everyday activities over the preceding 3 months.
Additionally, the supplementary of MIDAS question on migraine severity in the past 3 months (i.e. migraine days), which is not part of the MIDAS score, was also utilized.
Follow-up
Baseline migraine severity evaluation was performed on a personal interview using a structured questionnaire, prior to the surgery. Patients were contacted by telephone 3 and 6 months following the bariatric procedure. The telephone interview included an evaluation of migraine severity (similar to the primary evaluation interview) and the patients were asked to report their current weight.
Statistical analysis
The two primary endpoints were changes in total HIT and MIDAS score. These endpoints were assessed by the Friedman test. Pair-wise post-hoc analysis using Bonferroni adjustment was performed (month 3 vs. baseline, and month 6 vs. the baseline; p < 0.025). For the missing data during the follow-up we used a conservative approach assigning pre-treatment estimations of MIDAS and HIT scores. Change in body mass index (BMI) was assessed by ANOVA repeated measures analysis. For the missing data we used a conservative approach assigning pre-treatment BMI values.
Women were further stratified by the median relative weight loss at 3 months (less than 10.5% and equal or higher than 10.5%). The frequency of headache at 3 and 6 months adjusted for the baseline frequency was compared between these two groups by general estimating equations with negative binomial distribution with log link.
Continuous variables with normal distribution were presented as mean ± SD and compared using Student’s t-test and paired t-test for the dependent variables. Non-normally distributed variables (as assessed by Kolmogorov–Smirnov test) were presented as median and interquartile range (IQR) and compared using Mann–Whitney test for independent variables and Wilxocon non-parametric test for the paired observations. Dichotomous or nominal categorical variables were compared utilizing chi-square test with normal approximation or Fisher’s exact test when appropriate. Paired dichotomous variables were compared using McNemar test. Correlation between continuous variables was examined by Spearman correlation test. p-values < 0.05 (two-sided test) were considered significant.
Results
Baseline demographic and health-related characteristics of the study population

Values are mean ± SD or n (%), unless otherwise stated.
Figure 1 presents the mean BMI at baseline and 3 and 6 months follow-up visits among the intervention study group. The BMI descent is obvious and linear. Post bariatric surgery the migraine-suffering women reported a lower total frequency of migraine attacks (p < 0.001, Table 2). They also reported shorter duration of the attacks (p = 0.02), lower medication use during the attack (p = 0.005), and less non-migraine pain (44.8 vs. 33%, p = 0.05). There were six patients with chronic migraine (20.7%). At 3 months following bariatric surgery, five of them converted to episodic migraine, while at 6 months one of the patients with episodic migraine at the baseline converted to chronic migraine.
Mean body mass index (BMI) at baseline and 3 and 6 months follow up. Bars represent standard deviation. ANOVA repeated measures used for the analysis. Characteristics of migraine at baseline and 3 and 6 months after bariatric surgery Values are mean ± SD or n (%), unless otherwise stated. Two subjects lost to follow up. Seven subjects lost to follow up. Friedman test. IQR, interquartile range.
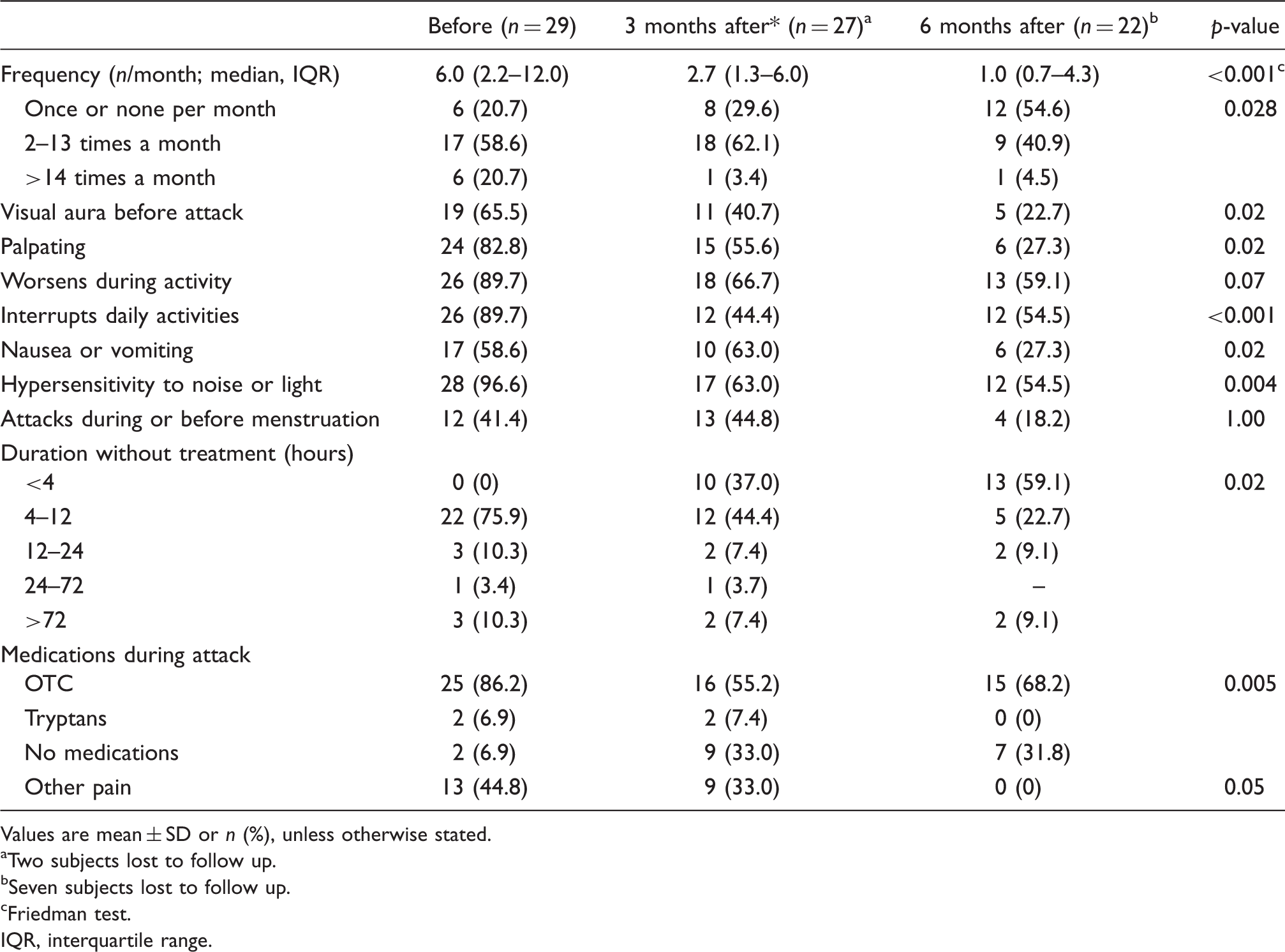
Figure 2 presents the post-bariatric surgery descent of headache-related disability assessed by the MIDAS score and the HIT-6 score, respectively. There was a significant decrease in both scores over 6 months, while in post-hoc analysis both scores were lower at 6 months and 3 months, respectively, as compared to the baseline (p < 0.005). The median headache frequency among the episodic and chronic migraine patients was reduced by greater than 50%. In 23 subjects with the episodic migraine the baseline median monthly frequency of migraine attacks was 4 (interquartile range 2–8), while at 3 and 6 months it was 2 (IQR 1–3.5) and 1 (IQR 0.7–2.8), respectively. Similarly six patients with chronic migraine demonstrated the decrease in migraine frequency from a median of 16.8 per month to 8.2 and 8.5 at 3 and 6 months, respectively.
Scores at baseline and 3 and 6 months follow up: (A) median MIDAS score; (B) median HIT-6 score. Bars represent 25 and 75 percentiles. Non-parametric Friedman test used for the analysis.
There was no significant correlation between relative BMI and MIDAS changes (p = 0.37 and p = 0.56) and relative BMI and HIT-6 changes (p = 0.27 and p = 0.31) at 3 and 6 months, respectively. Furthermore, no associations between the weight decrease at 3 months above and below the median (10.5%) and headache frequency at 3 and 6 months were found (adjusted for the baseline frequency, p = 0.81).
Discussion
In the present study, we demonstrated that migraine severity (as measured by headache days, HIT-6 and MIDAS) declines significantly following bariatric surgery and this effect last for at least 6 months. Although the association between migraine and obesity was established in epidemiological studies, this is one of the first studies describing the intervention, suggesting that treating obesity might affect migraine suffering.
Migraine is a common disorder, affecting millions worldwide. It has a tremendous impact on patients, families, and society in both direct and indirect ways. Although currently a biological marker for migraine does not exist, its diagnosis is made with relatively high precision on the basis of the criteria developed by the International Headache Society for migraine with and without aura which are now applied worldwide. Several tools have been developed to quantify the severity of migraine, which can be measured as migraine days per month, the impact of migraine on the patient’s life (HIT-6), or migraine-associated disability (MIDAS). In the present study, migraine was diagnosed using a structured questionnaire according to the ICHD-II criteria and its severity assessed using all of those measures.
Higher migraine severity among morbidly obese migraine-suffering women is consistent with previous studies, which have demonstrated not only increased migraine severity (15) but higher rates of transformation of episodic migraine to chronic migraine (16). In our cohort of obese women migraine prevalence was 27.6%, which is significantly higher than the reported migraine prevalence in the general population (12–18%) (4,6). In a large US survey, Ford et al. (4) found that BMI is associated with the increased prevalence of severe headaches or migraines in a non-linear manner (25.9% for BMI > 30 kg/m2 vs. 18.9% for BMI < 25 kg/m2). Similarly, the HUNT study found that among adolescents overweight is associated with recurrent headache [odds ratio (OR) = 1.4, 95% confidence interval (CI) 1.2–1.6, p < 0.0001] (2). The prevalence of migraine in our study (27.6%) was consistent with the reported prevalence in obese patients. Peterlin et al. (5) also demonstrated higher migraine prevalence (OR = 1.39) among obese women compared to non-obese women. Vo et al. (17) found that while obese women had a 1.48-fold increased odds of migraine vs. non obese women, severely obese women (OR = 2.07; 95% CI 1.27–3.39) and morbidly obese women (OR = 2.75; 95% CI 1.60–4.70) had the highest odds of migraines.
Recently Bond et al. (18) published a prospective observational study among 24 morbidly obese patients who had had bariatric surgery. Similarly to our study, a reduction in headache prevalence and severity was demonstrated. Number of headache days was reduced from 11.1 ± 10.3 days preoperatively to 6.7 ± 8.2 days postoperatively (p < 0.05). However, the effect of the surgery in the episodic and chronic migraine cohorts separately was not reported.
Possible mechanisms for the association between obesity and migraine have been studied [inflamation (19,20), plasma levels of calcitonin gene-related peptide (CGRP; (21), orexins (21), and adipokines (22,23)]. Regardless of the nature of the linking mechanism, the results of our study suggest that weight loss might be associated with migraine improvement. Although demonstrated only as a consequent of one method for weight reduction (bariatric surgery), it seems likely that the loss of weight by itself can act as a ‘prophylactic treatment’ for migraine, at least in the morbidly obese population. Further research should be addressed both to the assessment of the efficacy of different techniques of weight-loss interventions on migraine severity, as well as trying to define the mechanism by which weight loss affects migraine. This mechanism might even be a target for future migraine-preventing therapies.
As post-surgery diet patterns were not assessed in our study, another possible explanation for the migraine improvement might be connected to differences in food components or consumption post bariatric surgery. This issue should be focused upon in further studies.
Potential limitations of our study include the highly selected study population. The patients from the study group were all Jewish, relatively young (average age 33.4 years) premenopausal women and had chosen to treat their obesity surgically, either because of severe comorbidities or because of cosmetic reasons. Although prevalence of hypertension and diabetes in our cohort were comparable to previously published frequencies (24), the prevalence of dyslipidaemia in our cohort was higher. It is possible that psychiatric comorbidities, such as anxiety and depression, which are more common in obese people (25), are even more common among obese women who choose to undergo bariatric surgery. Depression was not evaluated in this study. Other limitations of our study include small sample size and the observational nature of this kind of studies. However, a randomized study to compare conventional migraine prophylactic drugs with bariatric surgery may not be feasible in a population of severely obese patients. The self-reported nature of the follow-up weight assessment could have introduced a recall bias. A follow-up study is required with a larger cohort group and morbidly obese non-bariatric surgery controls in order to strengthen the findings of this study. Nevertheless, the nature of the homogeneous study population possibly eliminated the possible confounding effects of race, gender, and life-cycle phase. As this was designed to assess effects at 3 and 6 months, a follow-up study should assess long-term effects of BMI reduction (12 or 24 months post surgery). Such a study might reveal that sudden change in BMI cause only a temporary reduction in migraine severity parameters.
In summary, we found that among premenopausal obese women post bariatric surgery the frequency of migraine attacks significantly reduced and headache-related disability improved. Our findings should be interpreted cautiously. The absence of a control group and the non-blinded nature of our small study make it difficult to draw firm conclusions about the causal nature of the headache changes observed in this population. Further study is needed to evaluate the possible specific effects of surgical weight loss on migraine in obese women.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.