
Abstract
This study was performed to document the frequency, duration and types of symptoms of postdrome in migraine patients. Eight hundred and twenty-seven consecutive headache clinic patients (IHS 1.1, 1.2 and 1.5.1) were evaluated at first visit. Postdrome frequency, duration and characteristics were analysed. Sixty-eight per cent of 827 patients reported postdrome (69.1% females; 56.8% males, P < 0.007). The average duration of the postdrome was 25.2 h. Fifty-six per cent had postdrome for ≤ 12 h, 32% for 12–24 h, 88% for ≤ 24 h, and 12% for > 24 h. The commonest symptoms were tiredness (71.8%), head pain (33.1%), cognitive difficulties (11.7%), ‘hangover’ (10.7%), gastrointestinal symptoms (8.4%), mood change (6.8%), and weakness (6.2%). Patients with postdrome compared with patients without postdrome have more characteristic and more frequent migraine features. This study demonstrated postdrome in 68% of patients, duration ≤ 24 h in most patients, more often associated with a full-blown migraine attack, more common in females, and with commonest symptoms being tiredness and low-grade headache.
Introduction
While the aura of migraine is well described, other components of the acute migraine attack are less well defined. The postdrome exemplifies this deficit. This period of symptoms occurring after the acute headache, while rarely disabling, can prolong the suffering of the acute headache and sometimes limit activity. The onset is often poorly defined, the symptoms vague, and the duration very variable. The biological substrate for the postdrome is unknown. The postdrome receives no mention in The International Classification of Headache Disorders, 2nd Edition (1). Postdrome, as an entity, is rarely specifically addressed in the literature, the notable exceptions being by Selby (2) and Blau (3, 4).
This study provides a profile of the frequency, duration and character of postdrome symptoms, and highlights differences between migraine patients with and without postdrome, using a large, detailed clinical database in a headache clinic.
Patients and methods
Study population
The study population consisted of consecutive patients treated by the author in his clinical practice. A structured interview was conducted by the author or by headache and neurologically trained nurse practitioners. Data were recorded in a custom-designed database program.
Patients were excluded from the study if they had: (i) no headache, (ii) headaches thought to be related to trauma or injuries, (iii) complicated neurological problems, i.e. underlying brain or systemic illness related to their headaches, (iv) recent onset headaches, i.e. less than 1 month prior to study, (v) significant legal issues related to their headaches, (vi) been seen prior to the initiation of the database, (vii) declined to, or were cognitively not able to participate in the database interview, or (viii) had language or intellectual barriers.
Study design
All patients received a headache evaluation, based on their past month's typical headache characteristics, as well as a physical and neurological examination. A thorough medical history of these patients was also recorded. All current and past medications used by the patients were noted. All patients were evaluated by the author. The headache diagnoses were made according to International Headache Society (IHS) criteria (3) using a computer algorithm written by the author, and each patient's diagnosis was verified by the author. Approval was obtained from an institutional review board for the use of the patient's information. The personal identities of patients were discarded when the data were downloaded to a statistical package.
Patient symptom rating
At the initial visit, the phases of migraine were explained to patients, including the concept of postdrome. They were asked whether they experienced postdrome (yes/no). If yes, they were asked to define the duration of the postdrome, and specifically whether they experienced gastrointestinal symptoms, mood changes, or tiredness (on a scale of 0–3: 0 = none, 1 = mild, 2 = moderate, and 3 = severe. They were also asked to provide a listing of other prodrome symptoms. Headache-associated features (average headache scale of 0–3: 0 = none, 1 = mild, 2 = moderate, and 3 = severe), intensity (0–10), lifetime duration, frequency per month, duration, triggers, prodrome, percentage of patients with aura, percentage of headaches with aura, percentage recurrence and postdrome frequency were recorded. In addition, medication satisfaction, acute and monthly disability, grading of headache days, sleep normality, mood and habits were documented.
Statistical analysis
Statistical analysis was performed using the SSPS statistical package (version 11 for Mac; SPSS Inc., Chicago, IL, USA). Descriptive statistics were used. Mann–Whitney tests were used to compare women and men, migraine types regarding postdrome presence and postdrome duration, and differences between patients having and not having postdrome. P-values < 0.05 were considered to be statistically significant.
Results
Demographic characteristics
Eight hundred and twenty-seven patients were diagnosed as ICHD-2 1.1, 1.2, and 1.5.1 (migraine); 85.2% were females and 14.8% were males. The mean (± SD) age of patients was 38.2 ± 12.0 years, the youngest being 13.0 years and the oldest 81.7 years. Three hundred and thirty-nine patients were diagnosed as ICHD-2 1.6 (probable migraine).
Postdrome frequency
Of the 827 patients, 68.0% reported postdrome (69.1% females, 56.8% males; P < 0.007). The frequencies of the other migraine types are listed in Table 1. Postdrome occurred 1–33% of time in 29.1% of patients, 34–66% of time in 31.5%, and 67–100% of time in 39.4% of the patients with postdrome.
Postdrome frequency and duration in headache types
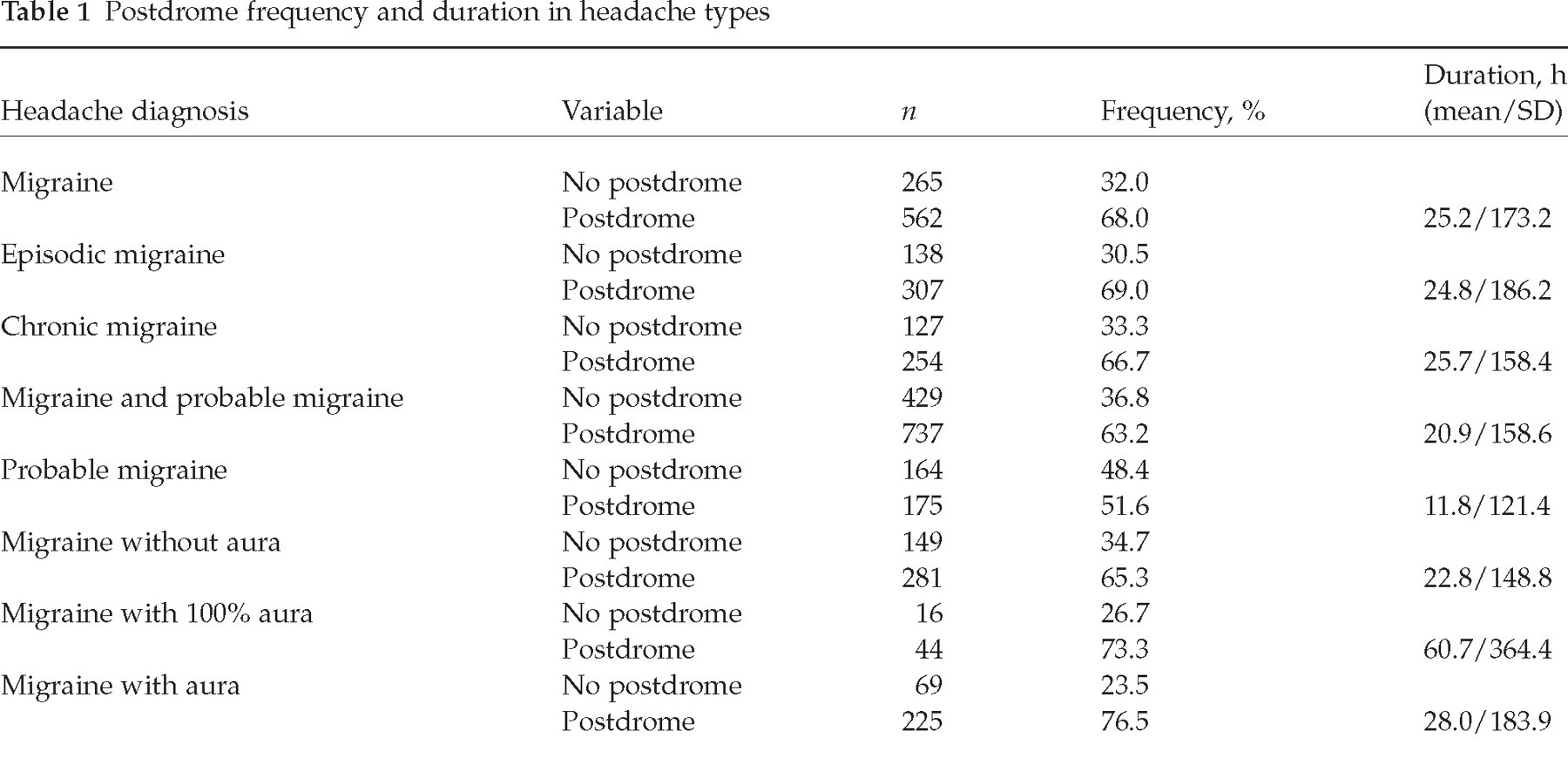
Postdrome duration
The average duration of the postdrome was 25.2 h. Fifty-six percent had postdrome for ≤12 h, 32% for 12–24 h, 88% for ≤24 h, and 12% for >24 h. The duration of the other migraine types is listed in Table 1. See Fig. 1 for the postdrome duration segmented into 12 h, 12–24 h and >24 h. Migraine with aura occurring 100% of time shows a trend towards longer duration of postdrome, the other migraine types being very similar to one another.

Postdrome duration by headache type
Postdrome symptoms
The commonest postdrome symptoms expressed by the patients were tiredness, head pain, cognitive difficulties, ‘hungover/hangover’, gastrointestinal symptoms, mood change, weakness and dizziness (see Table 2). This table shows the reported symptoms, the number of patients with the symptoms, the percentage occurrence of symptoms in patients having postdrome, and the percentage of each symptom or symptom group expressed as a percentage of the total symptoms.
Frequency of postdrome symptoms

Differences between patients with and without postdrome
Migraine patients with postdrome differed statistically (see Table 3) from patients without postdrome in many variables: more triggers as a whole and individually, lower headache frequency and less headache days, more prodrome and longer prodrome duration, more aura and greater percentage of headaches with aura, greater headache intensity, more headache aggravation by movement, more throbbing and stabbing, greater eye and neck location of headache, more associated symptoms, greater choice of rest or sleep with headache, more often forced to rest or sleep with headache, less able to function with headache, and greater number of family with migraine.
Postdrome vs. no postdrome in migraine; statistically significant variables


Variables not found to be statistically significant (P-value in parentheses): sleep disturbance trigger (0.418), sleeping late trigger (0.757), alcohol trigger (0.076), food trigger (0.062), neck pain trigger (0.078), sexual activity trigger (0.050), exercise trigger (0.333), smoke trigger (0.189), visual aura (0.271), aura no headache (0.872), lifetime headache duration (0.053), average headache duration (0.924), headache response to medication (0.620), time to absence of headache after treatment (0.051), time to 50% reduction of headache with treatment (0.457), percentage headache recurrence (0.158), aching character (0.376), pressure character (0.094), frontal location (0.494), temporal location (0.061), vertex location (0.263), occipital location (0.087), diffuse location (0.143), less school/work days missed (0.287), reduced housework days (0.708), severe headache days (0.656), sleep excess (0.384), sleep hours per night (0.893), trouble falling asleep (0.062), anxiety (0.239), depression (0.225), physical well-being (0.589), general aches and pains (0.058), tiredness (0.165).
Discussion
The acute migraine attack, with its prominent pain and associated symptoms, culminates, often imperceptibly, with the symptoms called the postdrome. It can be debated whether the postdrome is indeed a separate phenomenon or just a lessening of the preceding full-blown attack. Certainly some of the symptoms, such as residual head pain, expressed by patients sound as if they may be part of the more acute active phase of the migraine headache. The head pain is often head tenderness but is difficult to separate from a low-level headache. However, in practice one is impressed with how readily patients are able to separate the postdrome from the acute attack if specifically asked. ‘The calm, after the storm’ as one patient aptly summarized the author's concept of postdrome. Clearly there is no absolute marker for the end of the migraine acute attack and the beginning of the postdrome.
Postdrome frequency
This study of a large number of migraineurs shows that two-thirds of them describe a postdrome, but not necessarily with every headache. The frequency in the pre-IHS classification retrospective study of Blau (3) reported postdrome in 47 of 50 patients, while the later diary-controlled study (4) does not specifically state the frequency in the 40 patients studied. Postdrome is more frequent in females.
Postdrome duration
In slightly more than half of the patients the postdrome lasts for ≤12 h but only in 12% does it last for longer than 1 day. The average duration of postdrome was 25.2 h compared with 18 h in the study of Blau (4). In the current study in patients with migraine with aura occurring in 100% of headaches the postdrome tends to be longer. The shortest average duration of postdrome occurs in probable migraine.
Postdrome symptoms
The commonest postdrome symptoms in this study are tiredness, head pain, cognitive difficulties, ‘hungover/hangover’, gastrointestinal, mood change, weakness and dizziness. These are similar to the study of Blau (4), but direct comparisons are difficult. Notable in the current study is the infrequent complaint of specific neck symptoms in the postdrome compared with that reported by another study specifically addressing neck symptoms (5). However, within the context of ‘hungover/hangover’, tiredness, weakness, malaise, some neck symptoms may be present, although not specifically volunteered by the patient.
Comorbid depression and anxiety do not seem to play a role in the postdrome syndrome in this study. Patients routinely grade their level of anxiety and depression in the interictal state on a 0–3 scale during their evaluation. The Z scores and significance for comparing patients with and without postdrome for anxiety (−1.179, P = 0.239) and depression (−1.214, P = 0.225) show no differences. While not an accepted or formal method of evaluation of anxiety and depression, this finding is nonetheless suggestive that interictal anxiety and depression do not play a role in the postdrome syndrome. Also, interictal ‘tiredness’ (−1.387, P = 0.165) and ‘general feeling of well being’ (−0.541, P = 0.589) similarly graded in the interictal period show no apparent impact on the postdrome syndrome. These findings suggest that the postdrome state relates more to the migraine process than to the underlying state of the individual in the interictal period. This is certainly an unexplored area and warrants further study.
What brain processes do these symptoms reflect? Some of them are probably a lingering of the acute attack with residual pain and symptoms. Medication used to treat the migraine may contribute in some patients. There is a similarity of some of the postdrome symptoms to premonitory or prodrome symptoms (6). While this raises the issue of some pathways or mechanisms common to both syndromes, it may be more of a reflection of non-specific neural pathway activation or disinhibition. Conceptually, the author considers the two processes to be very different but this has not been proven. It is conceivable that the prodrome and the postdrome are part of one process, interrupted or perhaps camouflaged by the headache and associated symptoms. An answer to this question may lie in an ongoing study being conducted by the author comparing patients with migraine headaches having prodrome but not postdrome with those with postdrome but not prodrome.
The clinical impact of central sensitization (7) on brain function, apart from allodynia, has yet to be determined. Possibly the postdrome reflects this sensitization or, more likely, the aftermath of brain sensitization. Persistent, but decreasing, electrophysiological dysfunction has been documented after the acute migraine attack (8). These symptoms may represent the expression of a brain drained of its normal metabolic milieu, perhaps similar to a postictal state after a seizure. A possible alcohol hangover analogy does not shed light on the mechanism (9).
Postdrome and other migraine features
Reference to Table 3 shows an interesting and striking finding. The presence of postdrome is reflected in migraine attacks with more triggers, prodrome, aura and associated symptoms, higher intensity, more throbbing, stabbing, pain with head movement
Study limitations
This study suffers from some imperfections. It is a study of tertiary care patients and not a population cross-sectional study. The patients are from a single clinic. This is not a prospective study and no diary documentation was available, although some patients had documented headache profiles for prior provider evaluations. Also lacking in this study is the temporal evolution of the postdrome profile. The large number of correlations performed in this study almost guarantees that some will be statistically significant by chance. It also remains an unresolved issue whether data are better collected by direct questioning (‘do you have neck stiffness?’) or by eliciting responses without any hint of suggestion (‘what other symptoms do you have?’).
Postdrome relevance
Postdrome currently has no place in the diagnostic criteria of migraine. Should it? It appears to be unique to migraine but this has never been evaluated. Some disability due to postdrome is well documented (4). In the quest for improved quality of life for migraineurs and improving treatment for individual patients, more attention should be focused on the postdrome in routine clinical management of patients.
Conclusion
This study provides a portrait of postdrome in a large group of patients. It shows the high frequency of postdrome in migraine, documents the duration and the range of symptoms, and highlights the association of postdrome with more typical and intense migraine attacks.