
Abstract
Background: The need to provide better outcomes for patients with headache, and to minimise the costs involved in doing so, has prompted the search for new modes of service delivery by exploring the service organisation and nursing role from various cultural, economic and global perspectives.
Materials and Methods: This study was based on comparisons with the UK headache service up to 2007, the point at which this study was set up. This UK service was based at the National Hospital for Neurology and Neurosurgery (NHNN, UCLH Trust). Data were obtained from US headache centres in 2008 and from centres in Copenhagen, Bangkok, Sydney and Porto Alegre in 2009.
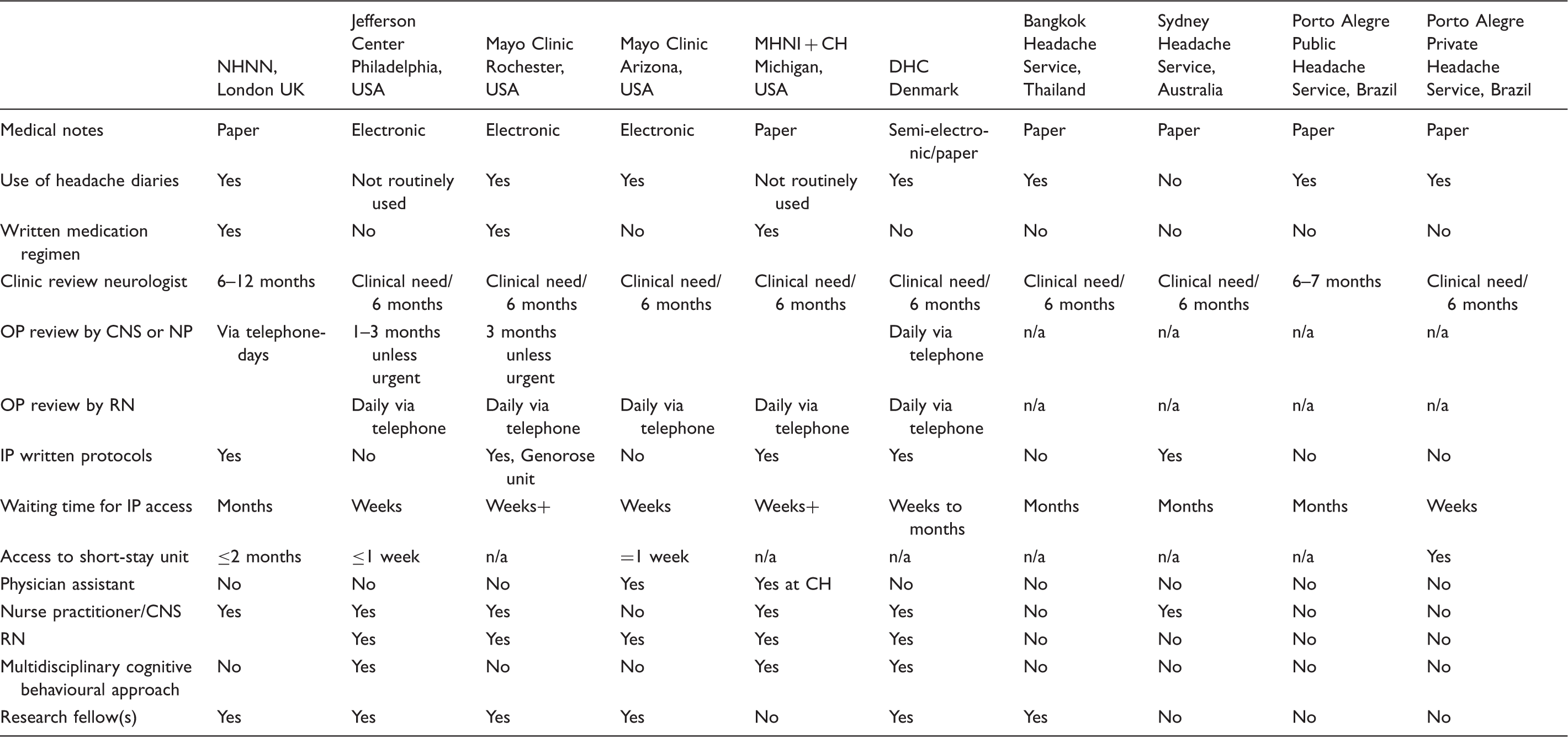
Results: A comparison shows the key components of services at all centres showing the team structure and size of service. Prominent features at the centres included: team-working, regular meetings, educational input, good access and communication among team members, headache-trained neurologists, specialist nursing at most centres, and the input of psychological and physical therapists at some centres.
Conclusions: The problems of tertiary headache care are very similar throughout the world and seem to transcend ethnic, cultural and economic considerations.
Introduction
Successful management of headache presents a real challenge to both primary care providers and neurologists. Primary headaches are among the most common disorders of the nervous system (1). They are wide-spread and, in many cases, chronic long-term conditions. A wide range of headache types have been classified in detail by the International Headache Society (IHS) as the International Classification of Headache Disorders (2). The more common primary headache conditions include migraine, cluster headache and tension-type headache, and the best estimates suggest that for Western Europe and North America about 20% of neurology referrals are for headache.
Headache syndromes cause substantial levels of disability to sufferers. Headache has been, and continues to be, underestimated in scope and scale, and remains under-recognised and under-treated throughout the world. Globally, headache affects 10–15% of the population and the World Health Organization has ranked migraine 19th among the causes of disability (3). Cluster headache is regarded as the most painful condition that exists in humans (4); as it is relatively common by neurological standards at one year prevalence of about one in one thousand (5), it offers a very substantial burden to its sufferers.
The impact of headache on society includes its effects on individuals, the direct costs of medical treatment and the indirect costs of lost productivity at work and in family life. It is estimated that headache accounts for 32% of all neurological costs in Europe (6). As an example of the impact, a large European survey of women with migraine aged 18–35 years and using headache medications, found they had on average 2 days of absence and 4 days of reduced function in work or school in the previous 6 months (7). They also felt that migraine had prevented them from achieving their career goals and limited their involvement in leisure activities. Frustration, anger, depression and fear were also commonly reported (7).
Set against this background, specialist headache care is relatively limited. In the UK, specialised headache centres that include out-patient and in-patient management strategies are a relatively new level of service for patients. It is our impression that such services are well received, indeed valued, by patients (8). Even in countries where in-patient care has been used for many years, such as Australia (9) and the US (10), there are relatively few centres given the population prevalence of headache disorders. Here, we sought to survey what is done across the world in a snapshot of headache centres to understand cultural and economic dimensions of what is certainly a global issue.
Materials and methods
The London, UK service up to 2007 is described. Some background on healthcare systems is to be found in Appendix 1.
Visits to eight international centres provided information on service components and delivery, team structure and size of service. Discussions with each team and observation in clinical practice enabled understanding of the key features of these specialist centres.
Given the training and interests of one of us (RB), there is a strong emphasis on non-medical, in particular nursing (11), roles in headache centres.
Centres visited
The centres visited were: USA: The Jefferson Headache Center, Thomas Jefferson University Hospital, Philadelphia, USA USA: The Michigan Headpain and Neurological Institute, Ann Arbor and Chelsea Hospital, Michigan, USA USA: The Mayo Clinic, Rochester, Minnesota, USA USA: The Mayo Clinic, Arizona, USA Europe: The Danish Headache Centre, Copenhagen, Denmark Asia: The Bangkok Headache Service, Thailand Australia: The Sydney Headache Service, Australia South America: two headache services in Porto Alegre, Brazil (public + private)
Analysis
Summary data are presented and tabulated. Since the basis of the study was qualitative no formal hypothesis testing has been conducted.
Results
Comparing centres by components and team structure
Comparing centres by service size

The UK Headache Service – The National Hospital for Neurology and Neurosurgery (NHNN), London, UK (service lead, PJ Goadsby)
In the UK, at the time of the survey, NHNN had the only established tertiary referral service offering out-patient, in-patient and day-care treatment options for patients with all types of headache. Patients will already have seen their general practitioner (GP) and at least one neurologist before being referred. The clinical team consisted of the lead neurologist, two additional neurologists (Kaube and Bahra), one full-time and one part-time clinical nurse specialists (CNSs).
In addition, there was a research team largely consisting of medical trainees seeking clinical experience in headache or pursuing higher degree research in headache. NHNN provide a substantial out-patient service aligned with day-case facilities, short stay (5 days) and longer stay in-patient facilities. Day-case facilities were used to develop and audit suitable procedures, such as greater occipital nerve injection (12), and for treatments, such as intravenous caffeine for low CSF volume headache (13). Five-day admissions were used for systematic characterisation of complex headache phenotypes, such as trigeminal autonomic cephalalgias (14). Attacks could be triggered by nitroglycerin to evaluate onset and phenotype, treated with high-flow oxygen, which acted as preliminary data for a subsequent randomised controlled trial (15), and the development of the placebo-controlled indomethacin test, which is pivotal in differentiating hemicrania continua from unilateral chronic migraine (16), among other uses. Dihydroergtamine was used by infusion with a modification of the Raskin protocol (10) that increased dosing (17) based on a proposed mechanism of action in the brain (18). Intravenous aspirin was used for medication withdrawal (after Kaube) and shown to be effective and well tolerated (19). It should be noted that the service has an active basic research arm (20,21).
The Jefferson Headache Center, Philadelphia, USA (service lead SD Silberstein)
The Jefferson Headache Center treats patients with all types of headache. The clinical team consisted of the director, three additional neurologists, a psychiatrist, a psychologist, biofeedback clinician, full-time and part-time registered nurses, two nurse practitioners and administrative and clerical support staff and a business manager.
They provided a large out-patient clinic service, in-patient treatment and short-stay or day-care infusion treatment. New patients would usually spend all morning or longer at the clinic. Follow-up appointments will be shorter but depend on the number of therapists they will need to see and the type of treatment they will receive. Some may have multiple sessions with a therapist(s) as part of the treatment in addition to the medical consultations. Patients generally had follow-up slots as often as they wish or are recommended, and the number of slots (not patient numbers) in a given year includes the treatment from all members of the multidisciplinary team. The centre is also involved in research and has a separate clinical research team. Some examples of the research interests include the use of topiramate in migraine (22), early descriptions of the use of dihydroergotamine in the in-patient setting (23), using the Raskin procotol (10) and work on the classification of frequent headache (24), which lead very directly to the current clinical criteria for chronic migraine (25). The service has a significant basic research component (26).
Michigan Headpain and Neurological Institute (MHNI) and Chelsea Hospital (service lead JR Saper)
MHNI-treated patients with all types of headache. The clinical team included the director and three additional neurologists, two physician assistants (at the hospital), psychologists, a part-time anaesthetist, registered nurses, physical therapists, technicians, and administrative and clerical staff. MHNI believes that its system of care and intensity of services reflect the requirements necessary to address complex headache conditions using experienced multidisciplinary, specialist staff to achieve outcomes.
New patients will spend a full day at the centre on their first visit to complete assessments. The in-patient service is located on a separate site at Chelsea Hospital on the in-patient ward for headache. The duration of an in-patient stay is approximately 2 weeks. All patients have multidisciplinary team input at the clinic and at the hospital. The number of allocated slots (not patient numbers) in a given year includes treatment from all members of the multidisciplinary team. The centre is involved in research and has a separate research team. Some examples include studies of topiramate (27), botulinum toxin (28) and occipital nerve stimulation (29) in chronic migraine.
The Mayo Clinic Rochester, Minnesota, USA (service lead FM Cutrer)
The team consisted of four neurologists, a nurse practitioner, two registered nurses and a fellow. The neurologists select the referrals they will see and new patients will generally be seen within 3 months.
This is a largely out-patient service and a minority of patients are referred to the pain rehabilitation unit if multidisciplinary team input, or medication detoxification supported by infusions, is recommended. Patients are not generally treated in the hospital for detoxification. The nurse practitioner runs nurse-led clinics and deals with some patient telephone queries. Registered nurses provide patient education, address patient queries and are also involved in research. Patients are not routinely referred to multidisciplinary therapists. The new patient appointments will range from 45 min to an hour. Follow-up consults may be shorter and will generally be at 3–6-month intervals according to clinical need. Research interests have included studies of factors affecting triptan treatment choices (30), clinical observations on rare headaches (31) and an interest in headache biomarkers (32). Important perhaps for understanding the clinical approach is that the lead has a significant background in basic research in headache (33).
The Mayo Clinic, Arizona, USA (service lead D Dodick)
The team consisted of the lead consultant neurologist, a physician assistant, a specialist nurse, a headache fellow and a resident. There is a separate research team. The consultant neurologist and physician assistant select the referrals they will see and appointments are offered with an approximate waiting time of 3 months for new patients.
Most patients are seen in out-patient clinics and some receive short infusion treatments on the short-stay infusion unit. There is minimal provision for in-patient detoxification treatment. Treatments like nerve blocks and Botulinum toxin injections are done in the clinics, and there is a substantial interest in the former in terms of clinical trials (34). The nurse co-ordinates the service, deals with patient telephone queries, renews prescriptions and arranges short-stay admissions as required. New patient visits may last up to an hour with shorter follow-up time. Follow-ups will generally be at 3–6-month intervals as dictated by clinical need. Patients are not routinely referred to other multidisciplinary therapists but, if deemed necessary, they will be referred to the general neurology service where access is good. The research interests of the clinic involve the treatment or selection of treatments for patients (35), an interest in the role of patent foramen ovale in migraine (36), the development of composite end-points for migraine studies (37), and the development of neurostimulation approaches to chronic migraine (38,39).
The Danish Headache Centre (DHC), Glostrup Hospital, Copenhagen, Denmark (service lead R Jenson)
The Danish Headache Centre treats patients with all types of headache and is the only tertiary referral centre for headache in Denmark. In addition to the lead neurologist, there are five neurologists (some work part time), three specialist nurses, physiotherapists and psychologists. With an average of 4300 consultations annually, they provide comprehensive multidisciplinary support for patients and have allocated in-patient beds that are used for analgesia withdrawal during a 2-week admission. Psychological support and education, physiotherapy and nursing support are core components of this highly organised service.
The service is also involved in research. There is a very strong culture of headache research in Denmark with seminal observations on brain blood flow in aura (40) that lead to the concept of the neural basis of the migraine aura (41). Moreover, the Danish group pioneered studying triggered migraine (42), which has made substantial contributions to understanding the disorder, including suggesting novel therapies (43). The group is perhaps better known as the incubator of the International Classification of Headache Disorders (2,44). There is a significant basic research group associated with the clinic (45,46).
The Bangkok Headache Clinic, King Chulalongkorn Memorial Hospital, Bangkok, Thailand (service lead A Srikiatkhachorn)
The Bangkok headache service treats patients with all types of headache and will accept referrals nationally via GPs or neurologists. The clinics are staffed by three neurologists and two residents. There is a cap on the total number of referrals accepted due to the limits on capacity and resources (around 500 annually). The headache neurologists must also run weekly general neurology clinics which further restrict the total number that can be accommodated in the headache clinics.
In practice, patients’ treatment and prescriptions are administered by this service and repeat prescriptions do not come from their GPs or referring doctors. Therefore, all medication monitoring and side-effect management must be done through this service. Hence, longer waiting times to follow-up and review may impact on safety and compliance. Patient education and treatment advice are given by the doctors. The use of headache diaries is actively encouraged as a tool that will optimise the consultation time and treatments. With the pressure on neurology beds, admissions for analgesia withdrawal, though desirable, have to be kept at a minimum and medication overuse headache is treated predominantly on an out-patient basis. A small number of patients may be referred to the general neurology service for input from psychologists or psychiatrists, if required. The service is also actively involved in research and the lead has a substantial background in laboratory-based research in headache (47,48).
The Sydney Headache Service, Prince Of Wales Hospital, Sydney, Australia (service lead AS Zagami)
The Sydney Headache Service accepts referrals from GPs, neurologists, pain clinics and direct private referrals: it treats all types of headache. The headache clinic is run within the neurology department on several days per week. Some patients are also seen in the general neurology clinics. Most patients are treated in out-patient clinics, annually 500 visits.
In-patient therapies frequently used include intravenous lidocaine and intravenous dihydroergotamine which are supported by established protocols. Support and administration is from the neurology ward doctors and nurses. Specialist nursing support is available for in-patient care from the clinical nurse consultant but resources are insufficient to cover clinics. As specialist nursing expands, there would be greater nursing input to other areas of the service. Admissions for analgesia withdrawal and intravenous treatments, however, may incur significant waiting times as beds are prioritised and as such admission numbers are limited. The lead clinician has a strong background in basic research in headache (49–53).
The Public Headache Service of Porto Alegre, Rio Grande de Sul, Brazil; Santa Casa Hospital, Porto Alegre (service lead LM Barea)
Porto Alegre is the capital city of the state of Rio Grande de Sul which has a population of 10 million. This is the main headache service of the public system. It provides access to all and treats all types of headache. The team consists of the lead neurologist, three residents and academic trainees. Specialist nursing roles have not yet been developed. Clinics are run on 3 days per week and are busy (15–18 patients per session plus over-bookings). New patients will generally wait between 1–3 months and follow-ups will wait 6–7 months. Referrals come mostly from GPs and the primary health system. Most patients present with chronic headache. Interestingly, patients in Brazil do not present with codeine overuse as opiates are not available over the counter. However, ergotamine and caffeine combinations and paracetamol (acetaminophen) compounds are more commonly overused. Triptan use (and hence overuse) is very limited due to high cost. In order to accommodate patients whose headache require more urgent review (e.g. cluster headache sufferers), clinics are routinely overbooked. The in-patient service is limited because of bed pressures and on average one patient per month will be admitted.
The Private Headache Service of Porto Alegre, Brazil; Moinhos de Vento Hospital, Porto Alegre (service lead Fernando Kowacs)
This service will accept and treat patients from throughout the state. The lead neurologist runs out-patient clinics on 3 days per week, does occipital nerve blocks in clinics, admits for some in-patient treatment and supervises patient treatments through follow-up consultations as clinically required. Patients must have appropriate insurance cover or may self-fund. The neurologist also works in the public service doing general neurology clinics on other days. Waiting time in the private sector is shorter, generally just weeks or less for appointments and waiting time for beds can be just days. However, with the current low staffing levels, just a limited number of in-patient admissions can be accommodated. Patients who are admitted privately will expect to see their neurologist for daily review although the junior medical team will administer and supervise their treatments. Patient compliance with medication is generally very good as patients expect and want a medication treatment when they consult. It is remarkable that the lead clinician has a solid background in basic (54,55) and clinical research (56) in headache.
Discussion
Here, we present a survey of major headache centres in Europe, North America, the Far-East (including Australia) and South America. There are certain common themes with all clinics being over-subscribed and under-resourced. There is a dominant theme of team-working to attempt to maximise resources in the constrained environments in which they operate. All the centres do research and it seems likely, given the relatively limited number of clinicians in headache world-wide, that it is no accident that the leads very often have strong backgrounds in clinical work and neuroscience. Headache is a common, disabling, global problem whose future is in the hands of academically orientated practitioners who can set and maintain standards. The greatest threat to patients with headache world-wide is under-funding the centres that manage them, and this threat is real and on-going (57).
Team-working
Team-working at all these centres was evident. Most centres had all staff based on the same unit or floor and there was overall good access, communication and support among team members. There was opportunity at each centre for regular team meetings. These may be to discuss difficult cases (e.g. at Jefferson), for staff education (e.g. at both Mayo Clinics), at a journal club (e.g. at Mayo Clinic Arizona), at weekly case meetings (e.g. at MHNI), daily nursing team meetings (e.g. at MHNI) or regular informal staff meetings (at DHC). Communication among the teams and across disciplines was evident within their very busy practices.
Headache diaries or calendars
These are routinely used at some centres. They were regarded as a useful tool for headache assessment and to monitor treatment. In general, they were used to record the date, time, duration, intensity and triggering factors for attacks, as well as the dosing and response to treatments used. This information was helpful across the service to assess headache type, severity, impact on daily life and monitor the success of treatment. There was some variation in the level of patient compliance but, overall, patients tended to complete them if encouraged by the staff. All centres, though busy and often overbooked, offered a minimum 30–45-min slots for patient consultations. A suitable simple daily diary as used at NHNN is presented (Appendix 2).
Electronic patient records
This was in use at most US centres. On the electronic system, all patient data and medical notes on previous visits, referral information, contacts with health professionals, effects of medications, doses used or changed, and all tests results and scans were readily available at all consultations for all patients. Also efficient for telephone contacts where the notes are readily accessible. At the DHC, paper notes are used at consults but most of the patient data are recorded electronically. It is envisaged that the electronic notes will develop further and enable further decrease reliance on paper notes at consultation. The Bangkok, Sydney and Porto Alegre centres continue to use paper notes in a similar way to the NHNN, in that some patient data are available electronically, but clinical consults are recorded in paper notes. In UK practice where paper notes are used and are sometimes unavailable at consultations or may be lost, late, or with a different healthcare professional and not always available where the patient is, efficiency is affected.
Telephone service
Nurses who take daily telephone queries or run telephone clinics have access to patient notes on the same day their telephone query arrived. Hence, the centres were set up to deal with patient telephone calls on the same day. Nursing time and resources are allocated for this which makes it more achievable. The centres which do not have specialist nurses to deal with telephone queries, rely on the neurologist responding to patient queries or overbooking these patients in clinics.
Written medication regimens
Some centres (Mayo Rochester and MHNI) like NHNN gave patients written medication dosing regimens at clinic visits. When preventive medications were prescribed, the patients were informed on how to take the medicines, the possible side effects and this written information provided a reminder of how to take the medication safely and possible side effects. GPs also found it useful.
Nurses
Registered nurses (RNs) and/or advanced practitioners (APs) trained in headache, worked at most centres. Their roles and numbers varied. All nurses were skilled at taking a headache history and knowledgeable on the treatments used. The nursing roles covered several areas of practice – in review clinics, doing nerve block procedures, patient education, life-style modification, medication management, telephone queries and consults and educational input in preparing patients for in-patient care. The larger centres employed higher numbers of nurses. The largest nursing teams were at MHNI and DHC and covered all aspects of care within the team.
Some centres had limited nursing input: the Bangkok and Porto Alegre services have not yet developed the specialist nursing role and junior doctors provide support to the service leads. Sydney has limited input from the nurse consultant who also covers other areas of neurology, but focuses on the in-patient service ensuring treatment protocols are reviewed and administered appropriately, with input from the neurology educator to meet staff training needs. In general, it was noted that services that had specialist nurses within the teams were highly organised whether this was in a public- or private-funded healthcare system.
Multidisciplinary team
Jefferson and MHNI had multidisciplinary team input for all in-patients and out-patients. Clinicians and therapists at these centres felt it was beneficial to improve patients’ quality of life, increased their motivation to optimise treatment, addressed psychological or behavioural issues, reduced the risks of medication overuse, reduced emergency room visits and ultimately, total healthcare use. At the DHC, most patients had input from psychologists and physical therapists. The DHC service treats many more patients with tension-type headache compared to the other centres. This may have influenced the components of service delivery, as psychologists and physiotherapists routinely treat these patients. The other centres did not feel that their patients will routinely require support or treatment from psychologists and physiotherapists.
At the Mayo Clinic Rochester less than 2% of patients are referred to the Generose pain rehabilitation unit. This centre provides intensive, focused facilities for detoxification from overused analgesics if indicated and it adopts a strong cognitive behavioural approach. At the Mayo Clinic Arizona, Bangkok, Sydney and Porto Alegre services, if input from psychological or behavioural therapists is deemed necessary, the patient will be referred to the services of the general neurology service within the hospital.
In-patient service organisation
There are limitations in comparing one treatment setting with another as there may be variations in the patient populations and expectations. Not all centres had developed an in-patient service. Jefferson, MHNI and DHC (like NHNN) accept all referrals and will admit more patients and use intravenous protocols and 24-h nursing care to treat patients who have not responded to out-patient treatments. The DHC run a ‘headache school’ that prepares groups of patients with medication overuse headache for an inpatient detoxification scheme with multidisciplinary support. Differences exist in other aspects of medical management and in the diversity of multidisciplinary services.
The two Mayo Clinic services do not have a substantial in-patient service. They are not set up to provide in-patient care as a significant component of their headache service. Mayo Rochester has access to the linked Generose pain rehabilitation unit but a very small proportion of patients are referred. The Mayo Clinic Arizona provides short-stay acute treatments that can be given on the infusion unit. Some part of this arrangement is historical, some part driven by cost and some part driven by the geography in that many patients attending the Mayo Clinics have travelled considerable distances. The Bangkok, Sydney and Porto Alegre centres are very limited by bed availability and admit smaller numbers for in-patient therapies.
Factors that influence both the need for hospitalisation and the type of care include: medical stability of the patient, presence of other medical illness, the level of medication overuse and whether patient monitoring is required. Treatments used included medication to control withdrawal symptoms, nausea, vomiting, dehydration, agitation and restlessness, sleep problems, and headache. Intravenous infusions often used included dihydroergotamine, lidocaine, valproic acid, magnesium and corticosteroids. Preventive treatments are introduced for longer term management.
Conclusions
Given the scale of the global burden of headache and the level of disability it imposes, it is imperative to have appropriate service planning and provision. Overall, all clinical leads acknowledged that headache sufferers will require a clear diagnosis, patient education, advice, treatment and monitoring and some will also require in-patient treatments. Some aspects varied: the availability of resources, specialist nursing input and the level of multi-disciplinary input. We could not summarise the situation better than to repeat the observations of Professor James Lance who founded the headache service and research unit in Sydney, and thus influenced the NHNN, Bangkok, Brazilian, and even Mayo Rochester clinic, felt: ‘What is needed is a very good, sympathetic doctor at the helm…one whose focus is clear and can decide what is needed’. He reflected that a good doctor or service lead would have appropriate: ‘training and knowledge, leadership and team skills and experience together with empathy with the patient and the perseverance to try many different treatments if necessary before the optimum is found’ (April, 2009).
In Appendix 3, we present some options for a service in the UK. It seems clear that headache centres are important and will flourish if funded with an academic culture that nurtures the headache medicine specialists of tomorrow.
Footnotes
Acknowledgements
The authors would like to thank the staff of the headache centres involved in this study. The study was funded by the Florence Nightingale Foundation, UK.