
Abstract
In order to investigate the prevalence of migraine with aura (MA) attacks according to the criteria set by the International Headache Society (IHS) for diagnosis down to the three-digit level of classification, and to determine the recurrence and possible variability of MA attacks over time, we conducted a 6–15-month-long prospective study on 64 MA patients (42 women and 22 men) consecutively referred for the first time to the University of Parma Headache Centre. At the end of the follow-up period, diagnosis was the same as at the first visit for 80.0% of patients, while it was changed for 20.0%. Throughout the duration of the study, the average number of attacks for each patient was 5.3 ± 6.2 (range 0–30). Attacks of migraine with typical aura were the most frequent (69.1% of patients), but migraine aura without headache (29.1%) and migraine with prolonged aura (20.0%) were also common; by contrast, basilar migraine and migraine with acute onset aura were reported only by one patient in either case. Migraine aura without headache was statistically significantly more frequent in males than in females. Our study results suggest that in most cases the frequency of recurrent MA attacks is relatively low and provide interesting indications about the prevalence of the different MA subtypes listed in the IHS classification, albeit in a headache clinic population.
Keywords
Introduction
The 1988 International Headache Society (IHS) classification (1) lists six different types of migraine with aura (MA) and, for each one of them, it sets a number of criteria to be adhered to for their diagnosis. The IHS classification in general is so structured that it allows a diagnosis of the attack rather than of the disease. This also applies to MA, a disorder that exhibits typically distinctive characteristics but may vary in its clinical features from one attack to the next—to the point that the same patient may be diagnosed with different MA subtypes down to the three-digit level of the IHS classification.
The literature reports a few prospective self-observations by people with migraine with aura (2–6). In addition, studies on the different MA subtypes listed in the IHS classification are few in number (7–10). Therefore, we thought that a prospective study was needed to investigate the recurrence of attacks over time in a group of MA patients according to the IHS criteria for diagnosis down to the three-level digit of classification. The purpose of our study was then to: (i) determine the frequency of the different types of attacks; and (ii) determine whether and how they varied over time.
Patients and methods
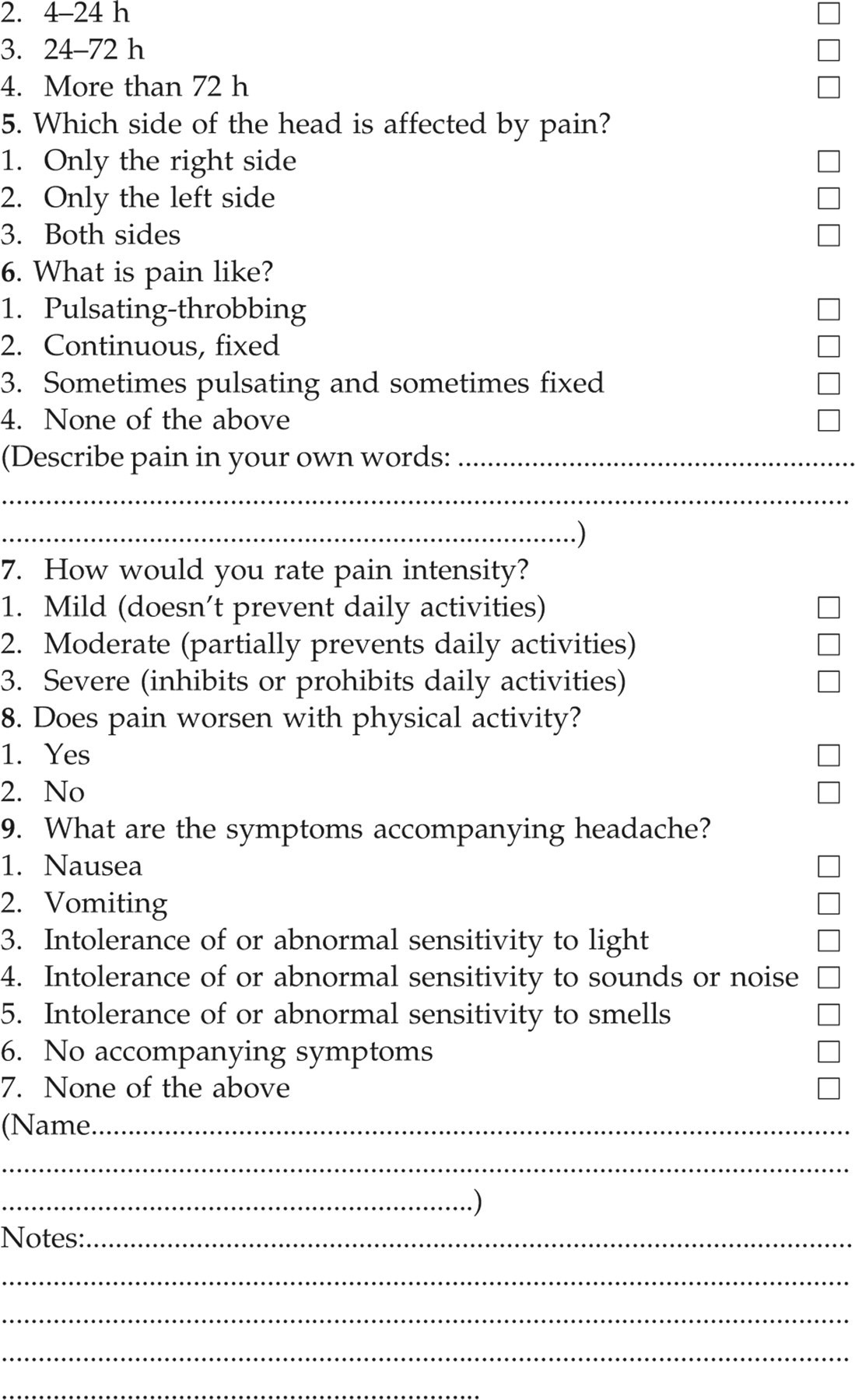
Our study population consisted of all patients consecutively referred for the first time to the University of Parma Headache Centre between 1 April 1998 and 31 December 1998 on a diagnosis of MA according to the IHS classification (1). The sample included 64 patients, i.e. 42 women and 22 men. At the time of their first visit, each patient received several copies of a questionnaire, which was to be filled in by the patients themselves at any future attack. The specially designed questionnaire was so structured as to provide all the necessary information for a diagnosis of migraine down to the three-digit level of the IHS classification and of tension-type headache down to the two-digit level of the IHS classification (1).
The patients were asked to take symptomatic drugs to relieve attacks throughout the follow-up study only if they thought they really needed them and, in any case, never before the start of the headache phase.
The patients were individually requested to call back the same physician (C.D.) who had seen them at their first visit at the Centre within 24 h of onset of an MA attack. During the phone interview, the doctor (C.D.) discussed with the patient the answers that he/she had given to the questionnaire at home and recorded them in the Centre's clinical records.
All patients were then put through a follow-up routine of visits on a 3-month basis. During each visit, they handed in their questionnaires and had them discussed with the medical staff.
We reviewed all data collected up to 30 June 1999, i.e. at 6–15 months’ follow up. Statistical analysis was done by χ2 test.
Results
Our sample included 64 patients (42 women and 22 men). Mean age at the time of their first visit was 30.5 ± 11.6 years (range 12–69 years), i.e. 29.6 ± 9.8 years (range 12–51 years) for females and 32.1 ± 14.4 years (range 14–69 years) for males. Mean age at MA onset was 20.0 ± 11.3 years (range 6–68 years), i.e. 20.7 ± 9.5 years (range 9–45 years) for females and 18.6 ± 14.4 years (range 6–68 years) for males.
An accurate review of the patients' histories showed that, up to the time of their first visit, 52 (36 women and 16 men, or 81% of the total sample) reported only one MA subtype. Nearly two-thirds of them had had only attacks of migraine with typical aura, while about 10% had had only attacks of migraine with prolonged aura. Twelve patients (six women and six men, or 19% of the total sample) reported two types of attacks in various combinations. None of the patients reported more than two different types of MA attacks. Attacks of migraine aura without headache were reported more frequently by males (eight patients out of 22) than by females (six patients out of 42) (P < 0.001) (Table 1).
Retrospective diagnosis of migraine with aura (MA) subtypes at the first observation


P = < 0.001.
1.2.1 Migraine with typical aura.
1.2.2 Migraine with prolonged aura.
1.2.3 Hemiplegic familial migraine.
1.2.4 Basilar migraine.
1.2.5 Migraine aura without headache.
1.2.6 Migraine with acute onset aura.
The average duration of the follow-up period was 9.6 months, i.e. 9.9 months for females and 9.1 months for males. The total number of MA attacks reported by our 64 patients in the follow-up period was 340, i.e. 233 for females and 107 for males. The average number of attacks in the follow-up period was 5.3 ± 6.2 (range 0–30), i.e. 5.5 ± 6.2 (range 0–30) for females and 4.8 ± 6.2 (range 0–28) for males.
Nine patients (six women and three men, or 14% of the total sample) had no attacks during the follow-up period. At the time of their first visit, all of them had reported only attacks of migraine with typical aura. Of the remaining 55 patients (36 women and 19 men), four (one woman and three men, or 6% of the total sample) had reported only one MA attack during the follow-up period, 34 (23 women and 11 men, or 53%) two to five attacks, 10 (eight women and two men, or 16%) six to 10 attacks, and seven (four women and three men, or 11%) more than 10 attacks.
Both in the retrospective and in the prospective phase of the study, 98% of patients reported visual aura symptoms (except one patient with sensory aura symptoms, consisting of left-side cheiro-oral paresthesias recurring unchanged in all attacks). Both at the first observation and in the follow-up period, visual aura was always characterized by scintillating scotomas and fortification spectra in 38% of cases, vs. 57% with either scintillating scotomas (29%) or fortificating spectra (27%), occurring only in one visual hemifield in 81% of cases (consistently the right or the left one in 66%) or in the whole visual field in the remaining cases (consistently in the whole visual field in 17%).
In at least one attack, 52% of patients reported mixed aura symptoms, i.e. both visual and sensory, with paresthesias always following the visual disturbances and affecting unilaterally one side of the face/tongue and one hand/arm in 56% of cases, i.e. localized to one upper limb in 26% and to the right or left hemiface or hemisoma in the remaining cases.
Both retrospectively and prospectively, all patients suffering from migraine with prolonged aura reported only one prolonged mixed aura (with both visual and sensory disturbances). No patients had aura including some degree of hemiparesis, either in the retrospective or the prospective stage.
The average duration of aura in our sample varied between 10 min and 30 min in 58% of cases, and was < 10 min or > 30 min in 19% of cases, respectively. Aura symptoms lasting > 60 min (1.2.2 attacks) were reported by 10 patients (five women and five men) at the time of their first observation and by 11 patients (six women and five men) in the follow-up period.
None of the patients reported in their past medical histories any factors that might account for a prolonged duration of aura.
Distribution by type of attacks at the three-digit level of the IHS classification in the 55 patients who reported MA attacks during the follow-up period is shown in Table 2.
Migraine with aura (MA) subtypes during the follow-up period (n = 55)

1.2.1 Migraine with typical aura.
1.2.2 Migraine with prolonged aura.
1.2.3 Hemiplegic familial migraine.
1.2.4 Basilar migraine.
1.2.5 Migraine aura without headache.
1.2.6 Migraine with acute onset aura.
Thirty-nine of the 51 patients with at least two MA attacks in the follow-up period reported only one type of attack, while the remaining 12 had two different types of attack.
Attacks of migraine with typical aura were the more recurrent, but episodes of migraine aura without headache and migraine with prolonged aura were also frequent (in over one-quarter and in one-fifth of patients, respectively). Attacks of basilar migraine and migraine with acute onset aura were extremely rare (Table 3). Migraine aura without headache was statistically significantly more frequent in males than in females (Table 3).
Frequency of migraine with aura (MA) subtypes in the follow-up period
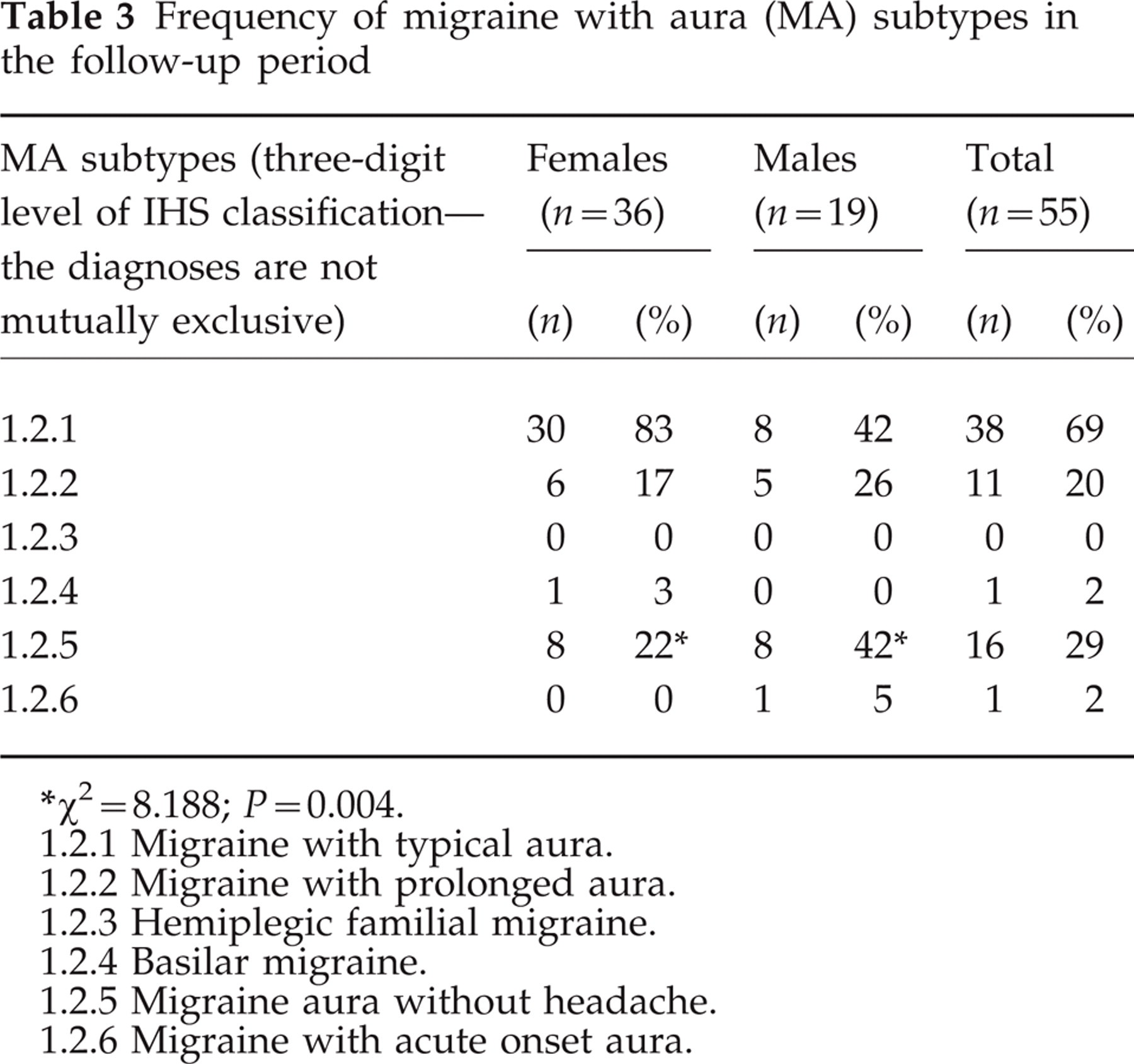
χ2 = 8.188; P = 0.004.
1.2.1 Migraine with typical aura.
1.2.2 Migraine with prolonged aura.
1.2.3 Hemiplegic familial migraine.
1.2.4 Basilar migraine.
1.2.5 Migraine aura without headache.
1.2.6 Migraine with acute onset aura.
Fourteen patients (six females and eight males) reported migraine aura without headache (1.2.5) at the time of their first observation. Age at onset for migraine aura without headache varied from patient to patient: 6 years of age in one case (a man), between 11 and 16 in five cases (three women and two men), between 20 and 27 in three cases (one woman and two men), between 30 and 39 in three cases (two women and one man), between 40 and 50 years in three cases (one woman and two men). Two more cases of migraine aura without headache were reported for the first time in the follow-up period by two women (aged 30 and 42 years, respectively).
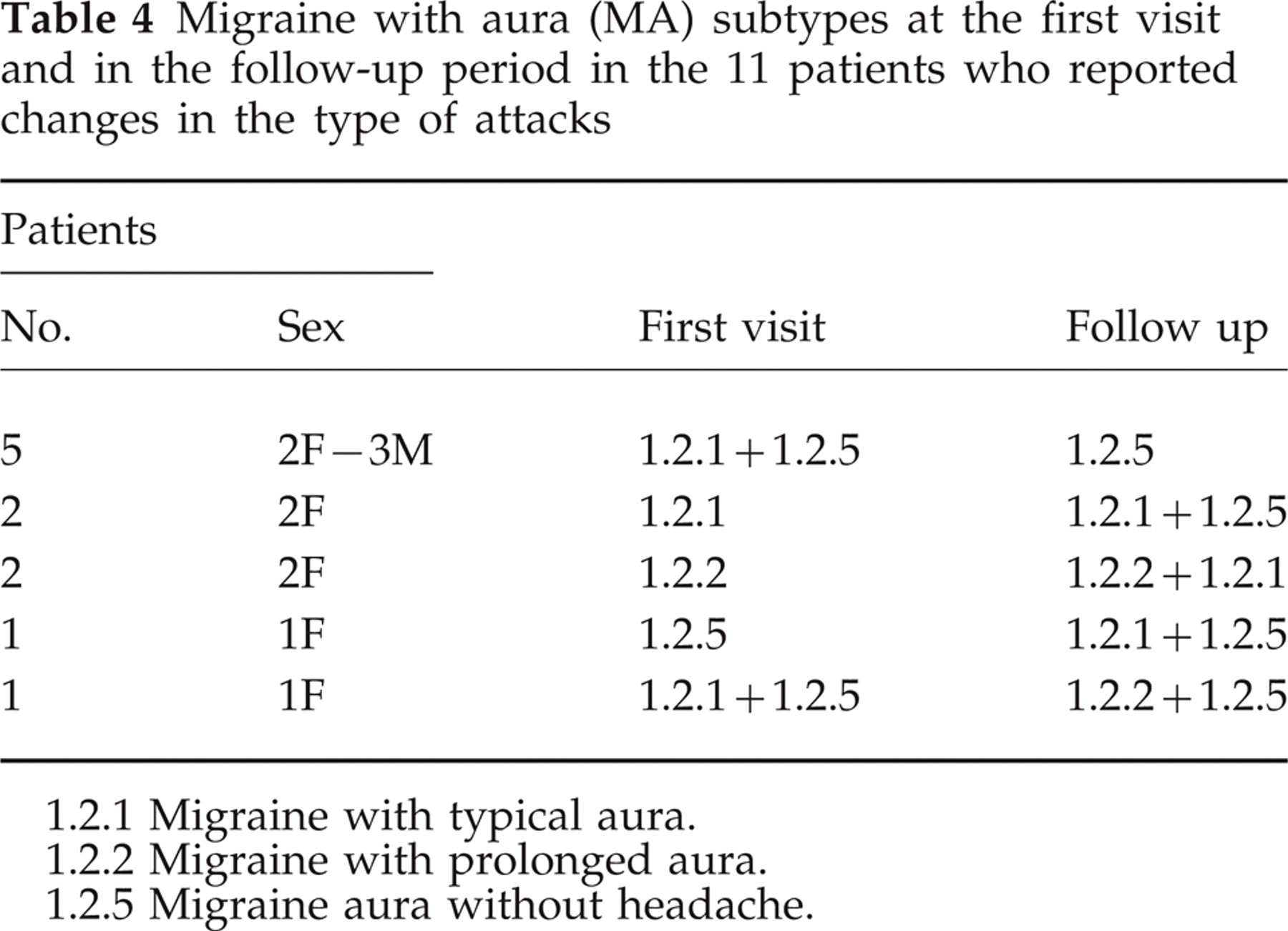
Among the 55 patients with at least one MA attack during the follow-up period, 44 (28 women and 16 men) had attacks of the same type(s) as that or those found at the first visit, five had only one of the two MA subtypes found at the first visit, five had both the MA subtype found at the first visit and another MA subtype never reported previously, and one who reported two MA subtypes at the first visit continued to suffer from one of the two and had the other replaced by a third, different MA subtype (Table 4).
Migraine with aura (MA) subtypes at the first visit and in the follow-up period in the 11 patients who reported changes in the type of attacks
1.2.1 Migraine with typical aura.
1.2.2 Migraine with prolonged aura.
1.2.5 Migraine aura without headache.
The 11 patients with changes in the type of attacks reported an average of 6.0 ± 7.5 MA attacks during the follow-up period (range 1–28).
Forty-six of the 64 patients included in the study (31 women and 15 men) did not take any preventive drugs during the follow-up period. The other 18 patients (11 women and seven men) took one or more preventive drugs, namely: flunarizine in eight cases, cinnarizine in three, lamotrigine in two, pizotifen in two, a combination of flunarizine and lamotrigine in one, a combination of flunarizine and pizotifen in one, and a combination of pizotifen and methysergide in one. Of the nine patients with no MA attacks during the follow-up period, only one (a woman) was on preventive therapy (with flunarizine). Of the 16 patients who had migraine aura without headache during the follow-up period, five were on preventive therapy—with flunarizine in two cases, cinnarizine in two and lamotrigine in one. Neither of the two women who in the follow-up period suffered from episodes of migraine aura without headache, in addition to the attacks of migraine with typical aura already reported at their first visit, was on preventive therapy; nor were any of the five patients who in the follow-up period suffered only from episodes of migraine aura without headache, while at their first visit they had also reported attacks of migraine with typical aura (Table 4).
During the follow-up period, 38 patients (59%) reported also other forms of primary headache, namely: migraine without aura (MO) in 25 cases (39%), including 19 women (45%) and six men (27%), and tension-type headache in 13 (20%), including eight women (19%) and five men (23%).
Discussion
The epidemiological investigations published so far in the literature on migraine prevalence among the general population (11–15) do not extend beyond the two-digit level of the IHS classification (1). This is mainly due to the methodological problems that are likely to be encountered in studies on migraine prevalence among the general population down to the three-digit level of the IHS classification. Obviously, any such study is bound to be hampered by procedural limitations, related both to the difficulty of having a questionnaire that is comprehensive enough to include all items required for a third-level diagnosis, and to the fact that in retrospective investigations the patients' recollection of migraine attacks may not be reliable enough to allow an accurate record of their clinical features.
On the other hand, no reports have been published so far in the literature on the frequency of the different MA subtypes among patient populations. Therefore, while the results of our study concern only a headache clinic population, they certainly provide useful indications for some interesting conclusions.
In our patients, the gender ratio (F : M = 1.9 : 1) and age at MA onset (20.0 years) were comparable to those reported by several authors (8, 11–13, 16–19).
Our prospective study enabled us to confirm the tendency of most MA patients to show a relatively low frequency of recurring attacks over time, as had previously been suggested by some retrospective investigations (7, 10, 19, 20). During the follow-up period of 6–15 months, our patients had on average an MA attack every 54 days and 20% of them even had only one attack or no attack at all throughout that period.
The accurate recording of the attacks' clinical features by the patients themselves at each occurrence enabled a diagnosis down to the three-digit level of the IHS classification and provided some interesting indications as to the type of attacks.
The first indication is the very low frequency not only of basilar migraine—whose rarity has been well known for a long time—but also migraine with acute onset aura—for which no data are available in the literature for a comparison of frequencies.
To date, the clinical entity termed ‘migraine with acute onset aura’ by the IHS classification is not a clearly defined form of headache. At first glance, the diagnostic criteria established by the IHS classification for this MA subtype do not appear restrictive enough to account for the occurrence of only one attack over a total of 340 attacks reported by our patients during the follow-up period. On closer scrutiny, however, the IHS diagnostic criteria may suggest otherwise. If, for example, during an attack with all the features typical of MO, a patient reports scintillating scotomas in the whole visual field or in parts of it which last only a few seconds, then, according to the IHS classification, he/she may be diagnosed as having migraine with acute onset aura. In all likelihood, though, this patient may be having an attack of MO. Probably, if our study had been done on patients with an initial diagnosis of MO instead of MA, the number of attacks that could be diagnosed as migraine with acute onset aura according to IHS criteria would have been far greater than it actually was during the follow-up period. The IHS classification should hopefully take this problem into account in its next revision, which should be modified accordingly.
Conversely, the results of our study point out a high frequency of migraine aura without headache, which was reported by about 30% of patients with MA attacks during the follow-up period. This percentage is higher than the about 2–20% figure reported in the literature (8, 10, 19), and does not appear to be affected by therapy. In compliance with our study protocol, patients had previously been asked to refrain from taking any drugs before the start of the headache phase, and, in any case, only a small minority of them was on preventive therapy. As suggested by previous reports, migraine aura without headache was significantly more frequent among males than among females (9, 20, 21).
Another finding of our investigation was that almost a quarter of the patients with at least two episodes of MA during the follow-up period reported different types of MA attacks. Had we chosen a longer follow-up period, the proportion of patients reporting different types of MA attacks would have very likely been much higher—which is what we intend to verify by carrying on our prospective study.
In 11 patients out of 55, the diagnosis established on the basis of the type of attacks reported during the follow-up period was at least partly different from that made at the time of their first visit. This may be due to the fact that it is obviously difficult to make a retrospective diagnosis of MA subtype(s) down to the three-digit level of the IHS classification. Another possible cause is that MA attacks may indeed vary in type in a single patient over time.
The duration of our follow-up study may have not been long enough to take in fully the different subtypes of MA that may occur in a single patient, as the frequency of MA attacks in general is relatively low. However, it was certainly long enough to establish a possible association with MO and tension-type headache, which are both well known to have a higher frequency. In our patient sample, the coexistence of MO attacks (39% of cases) was comparable to that reported by some authors (12, 20, 22), but lower than that reported by others (18, 23); the coexistence of tension-type headache attacks was found only in one-fifth of patients.
With our study we have tried to prove for the first time the reliability of the IHS classification at the three-digit level for MA, and our results, though applying to a clinical population, offer clues to the prevalence of the different MA subtypes listed in the IHS classification. They also demonstrate that a prospective approach is imperatively needed for any future study on the prevalence of MA subtypes in the general population.