
Abstract
A fixed location unilateral headache suggests involvement of a precise nervous structure, and neuroimaging investigations are essential to seek to identify it. Nevertheless, side-locked primary headaches also occur, although they are rare. Side-locked primary headaches are more frequently found in the group of the short-lasting (≤ 4 hours) headaches but long-lasting headache forms may also present with the pain always on the same side, including migraine, tension-type headache, new daily persistent headache and cervicogenic headache. Future studies should address the issue whether patients with side-locked headache form differ from those with non-side-locked form both in terms of natural history and biological markers.
Among 63 consecutive chronic cluster headache patients seen by us from 1999 to 2007, 32 (51±) had side shift. We also found that the duration of the chronic condition was significantly longer in those with side shift than those without. The high frequency of side shift in chronic cluster headache should be considered when proposing surgical treatment for severe intractable forms of the disease.
A pain syndrome presenting always on one side immediately suggests an anatomically circumscribed pathophysiological mechanism. Similarly, a fixed location unilateral headache suggests involvement of a precise nervous structure, and neuroimaging investigations are essential to seek to identify it. Nevertheless, side-locked primary headaches also occur, although they are rare. Generally, a side-locked primary headache is one of the group of short-lasting headaches—lasting less than 4 h—but may sometimes be long lasting. Hemicrania continua is long lasting and side-locked by definition, but other long-lasting headache forms may also present with the pain always on the same side, including migraine (1), tension-type headache (1), new daily persistent headache (2) and cervicogenic headache (3). The diagnostic criteria for cervicogenic headache are still controversial (4) even though this headache form has been extensively studied by Sjaastad et al. (3). Clinical studies by Sjaastad's group have also been important in helping to delineate other side-locked primary headache forms like hemicrania continua, paroxysmal hemicrania and SUNCT.
Few data are available on the frequency of primary side-locked long-lasting headaches, in part because of the lack of a clear clinical definition of the term side-locked. Thus, migraine may manifest on the same side for many years and suddenly change sides, suggesting the need for a time element in the definition. But for how long should the headache remain on one side only before we define it as side-locked? The question also arises as to whether there might exist pathophysiological criteria for defining side-locked primary headaches. Alternatively, there is the possibility of introducing a quantitative definition: we might define a side-locked condition as one where, say, 90% of the headaches in a defined (but fairly long) period are on one side only. A similar concept is already recognized in cluster headache, where at least 10% of patients experience a change in the pain side (5) even though cluster headache is usually considered side-locked.
Future studies should clarify whether patients with a side-locked primary migraine, tension-type headache, trigeminal autonomic cephalalgia, etc., differ from those with non-side-locked forms of these conditions.
Side-locked unilaterality in long-lasting primary headaches
Selby and Lance studied 500 migraine cases and found that 21% were ‘fixed unilateral’ (6), while other studies have reported considerably higher percentages of ‘unilaterality’ in migraine (up to 92%, for a review see (7)). The discrepancy may be accounted for by differences in definition: where the proportion of unilateral cases in a series is high, ‘unilateral’ probably includes alternating side head pain as well as side-locked. Friedman et al. (8) reported that 10% of tension-type headaches occurred on one side. Celentano et al. (9) found that ‘unilateral headache’ was often associated with scotoma and visual loss. It is likely that these patients had a form of migraine with aura; however, insufficient details were given to be sure. Thomsen et al. (10) reported that headache was unilateral in 53% of 145 patients with familial hemiplegic migraine.
At our Centre, 1169 cases of long-lasting (> 4 h) primary headache were diagnosed between 1988 and 1990. The frequencies of side-locked unilaterality were 17% (127/767) for migraine, 4% (10/244) for tension-type headache, and 27% (32/120) for non-classifiable headache (1). When present, unilaterality was fairly stable over time: 13 ± 10 years for migraine and 5 ± 7 years for tension-type headache (means ±
According to Sjaastad, many cases of long-lasting side-locked headache could be cervicogenic headache, particularly when the pain regresses after block of the greater occipital nerve (GON) or nerves in the neck (3). Predictive power calculation indicates that the most likely diagnosis when side-locked unilaterality is present is migraine (1). This is as expected, because migraine was the most common headache in the series studied, and because unilaterality is characteristic of migraine according to the IHS definition of migraine pain (4).
Response to GON or C2 block is reported as important for identifying and diagnosing cervicogenic headache (3). However, disappearance of pain after this kind of anaesthesia is not specific for the headache form. Gawel and Rothbarth (12) found that GON block was effective in 54% (52/97) of migraines and 71% (62/87) of post-traumatic headaches. Caputi and Firetto (13) reported significant improvement in 85% of 23 migraines treated with GON block, sometimes in association with supraorbital nerve block. Jansen et al. (14) reported disappearance of pain after C2-C3-C4 block in all their 14 patients with various headaches (from the descriptions, probably cervicogenic headache, cluster headache and chronic paroxysmal hemicrania). Magnusson et al. (15) noted pain disappearance after C2 block in 15 patients with persistent unilateral occipital pain following whiplash injury. Bovim et al. (16) investigated the efficacy of GON block in 24 patients with cervicogenic headache, 14 with migraine, and 14 with tension-type headache; they found a significant pain reduction 30 min after administration in 54% of cervicogenic headaches, 6% of migraines and 14% of tension-type headaches. GON block is known to be particularly effective when pain is confined to the distribution of the greater occipital nerve (17), and this might explain the greater efficacy of GON block in cervicogenic headache compared with migraine in Bovim et al.'s study (16). These authors did not specify the pain site; however, in cervicogenic headache the pain generally is more prominent posteriorly (occipito-nucal region), while in migraine the pain tends to be perceived in the anterior regions of the head. Note that according to the IHS (4), the site of the pain has no diagnostic significance for migraine or tension-type headache.
That GON block has limited significance in the diagnosis of cervicogenic headache, as well as other primary headaches, is suggested by other studies. Thus D'Amico et al. (18) obtained improvement with GON block in only 40% of patients diagnosed with cervicogenic headache according to Sjaastad's criteria, while other studies found that GON infiltration improved various primary headaches. Ambrosini et al. (19) reported that a single suboccipital steroid injection completely suppressed attacks in 10 of 13 CH patients, and Afridi et al. (20) found that 26 of 57 injections to the GON area in 54 migraineurs produced a complete or partial response (lasting a median of 30 days in those with partial response) and that 13 of 22 injections produced a complete or partial response in cluster headache (lasting a median of 21 days in those with partial response).
Side-locked unilaterality in cluster headache
Although cluster headache is often considered to be a side-locked form, at least 10% of patients experience a change of attack side during their clinical course (5). Our experience is that side shift is particularly common in chronic cluster headache. Among 63 consecutive chronic cluster headache patients seen by us from 1999 to 2007, 32 (50.8%) had side shift (4). We also found that the duration of the chronic condition was significantly longer in those with side shift than those without (6.8 ± 4.91 years vs. 1.8 ± 4.91 years; P < 0.0001) and that 20 (62.5%) of the 32 who presented side shift did so in the 2 years after developing the chronic condition (Fig. 1). The high frequency of side shift in chronic cluster headache should be considered when proposing surgical treatment for severe intractable forms of the disease.
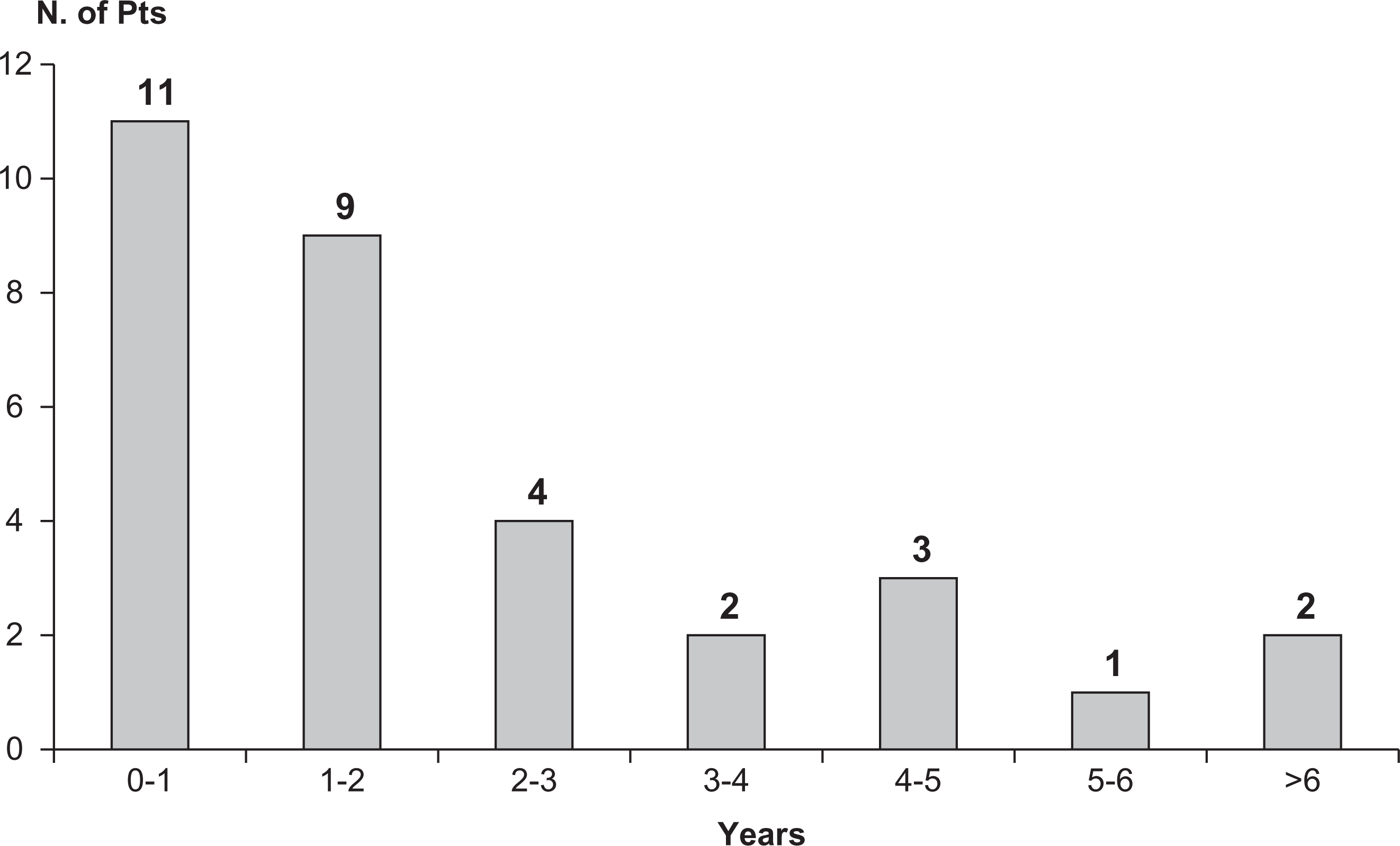
Time to occurrence of bilateral attacks after development of chronic form in 32 patients with chronic cluster headache.
The mechanisms that determine side lock in cluster headache are unknown; the reasons for side shift are similarly unclear. Various suggestions have been put forward (21). It is noteworthy that hypothalamic stimulation for chronic cluster headache is only effective against attacks occurring on the same side as the implant (22), and that peripheral stimulation (in the area of the GON) also seems to be effective only against pain attacks on the stimulation side (23, 24). The fact that deep brain stimulation is not effective against attacks on the other side suggests that the stimuli do not reach the homologous controlateral regions. The stimuli may be blocked by the intervening third ventricle and ependymal structures or perhaps by other non-hypothalamic cerebral structures involved in the pathophysiology of cluster headache (25).
Conflicts of interest
The authors have declared no conflicts of interest.