
Abstract
Aims: Peculiar characteristics of migraine headaches include the arousal of olfaction during the attacks and osmophobia. We performed an olfactory test to evaluate the association between olfaction and migraines.
Methods: We evaluated olfactory dysfunction in 80 migraine patients (31 experienced migraines with aura (MWA), 49 migraine without aura (MWOA)) and 30 healthy controls. Participants were assessed for concurrent osmophobia. Olfaction was evaluated using an odour stick identification test (OSIT), in which participants were asked to identify various odours during a migraine-free period. The degree of offensiveness of each odour was also evaluated.
Results: Sixty-three percent of migraine patients were found to have concurrent osmophobia (MWA 71%; MWOA 57%). The percentages of migraine patients and controls who correctly identified test odours were 91% (92%, MWA; 89%, MWOA) and 92%, respectively. Perfume, rose and Japanese cypress odours were more offensive to migraine patients than to controls. All test odours were found to be more offensive to MWA than to MWOA patients.
Conclusions: The OSIT showed certain odours to be highly offensive to migraine patients even when they were not experiencing migraine headaches. More attention should be paid to odours that are perceived to be offensive by migraine patients, particularly those with MWA.
Introduction
Migraines are widely recognized as headaches accompanied by photophobia and/or phonophobia. The International Classification of Headache Disorders (ICHD)-II includes photophobia and phonophobia among its main diagnostic criteria and osmophobia as an alternative diagnostic criterion (1). Excessive sensitivity is requisite for the diagnosis of migraine, and, at the same time, provides important information for elucidating the pathogenic mechanisms underlying migraine attacks. However, despite migraine headaches being a common affliction, few studies have focused on hypersensitivity in migraine sufferers. Although there has been relatively little progress on studies of osmophobia in association with migraine, a recent report (2) has provided valuable insights. Zanchin et al. (2) documented the usefulness of osmophobia in the differential diagnosis of migraine versus episodic tension-type headache, with osmophobia being observed in approximately 40% of patients with migraine but none of the patients with episodic tension-type headaches. Detailed investigation of osmophobia is useful in the diagnosis of migraine. Herein, we present an investigation of osmophobia and the results of objective olfactory and taste tests.
Methods
Self-report questionnaire
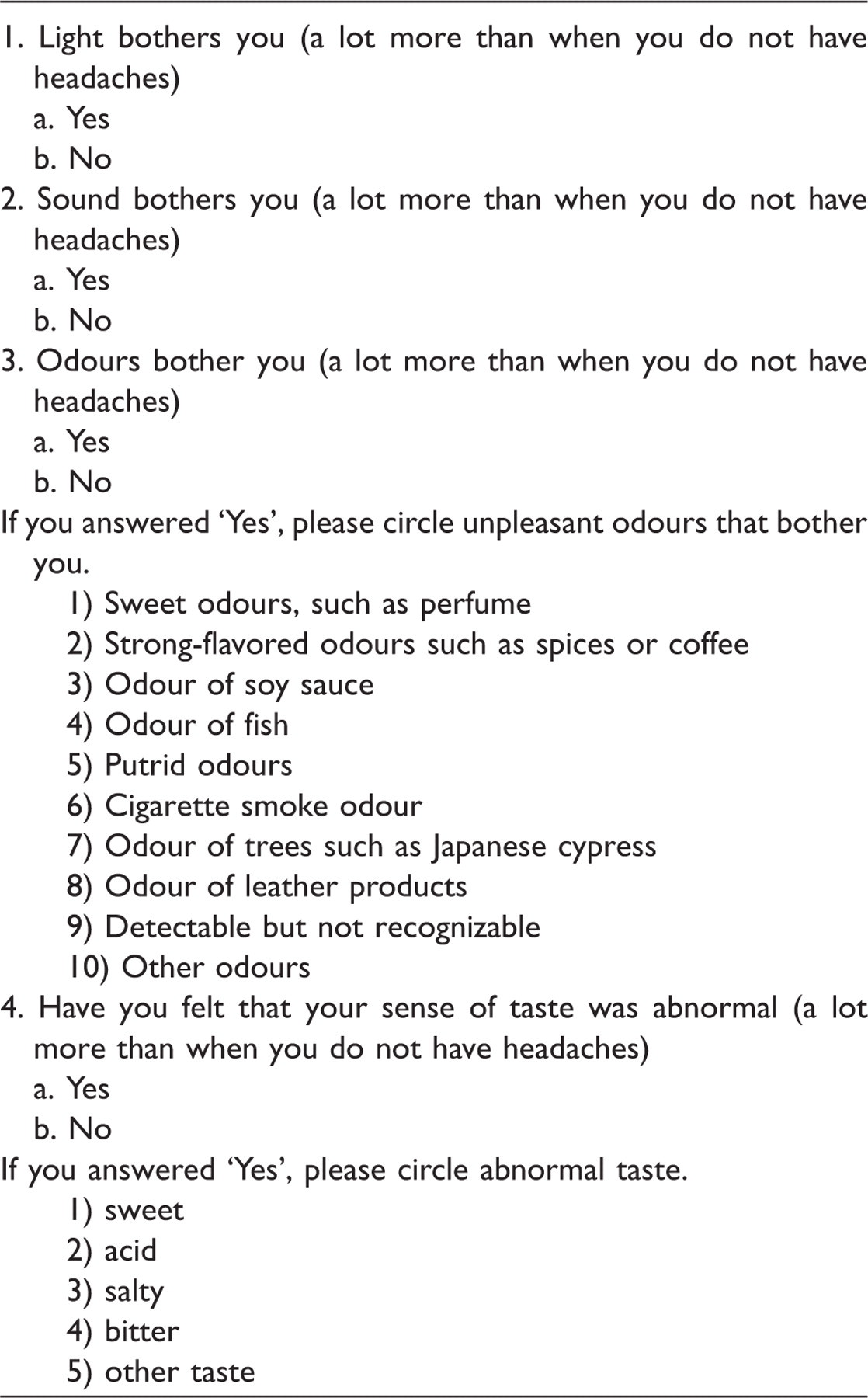
The self-report questionnaire form was designed primarily to detect indicators of photophobia, phonophobia, osmophobia and dysgeusia. If osmophobia was present, then the subjects were asked to further identify the type(s) of odour they found to be offensive among the following 10 items: a sweet odour (perfume); a strongly flavoured odour (spices or coffee); soy sauce odour; fish odour; a putrid odour; cigarette smoke odour; an odour of trees such as Japanese cypress; an odour of leather products; detectable but not recognizable; and other odours. Other questions addressed odours that tended to trigger migraines, when osmophobia initially developed, and the emergence and disappearance of osmophobia during a migraine attack. Furthermore, the subjects who exhibited dysgeusia were asked to identify the taste(s) that they found abnormal, by selecting from among the following: sweet, salty, acid and bitter.
The olfactory test was performed during migraine-free periods using an odour stick identification test (OSIT) (3) using 12 odour types. Each subject sniffed the test odours, identified each as one of the four given choices of odour type, and rated its degree of hedonic tone. Hedonic tone was rated on a 10-point score (10-point defined as absolutely unpleasant, 0-point defined as absolutely pleasant).
Taste tests were performed using the filter-paper disc method for the following taste types: sweet, salty, acid and bitter (on a concentration-based 5-point scale).
Statistical analysis was performed using the chi-squared test and analysis of variance (ANOVA). The level of statistical significance was set at p < 0.05.
Results
Demographic and clinical data of patients suffering migraine with aura (MWA) and migraine without aura (MWOA) and controls
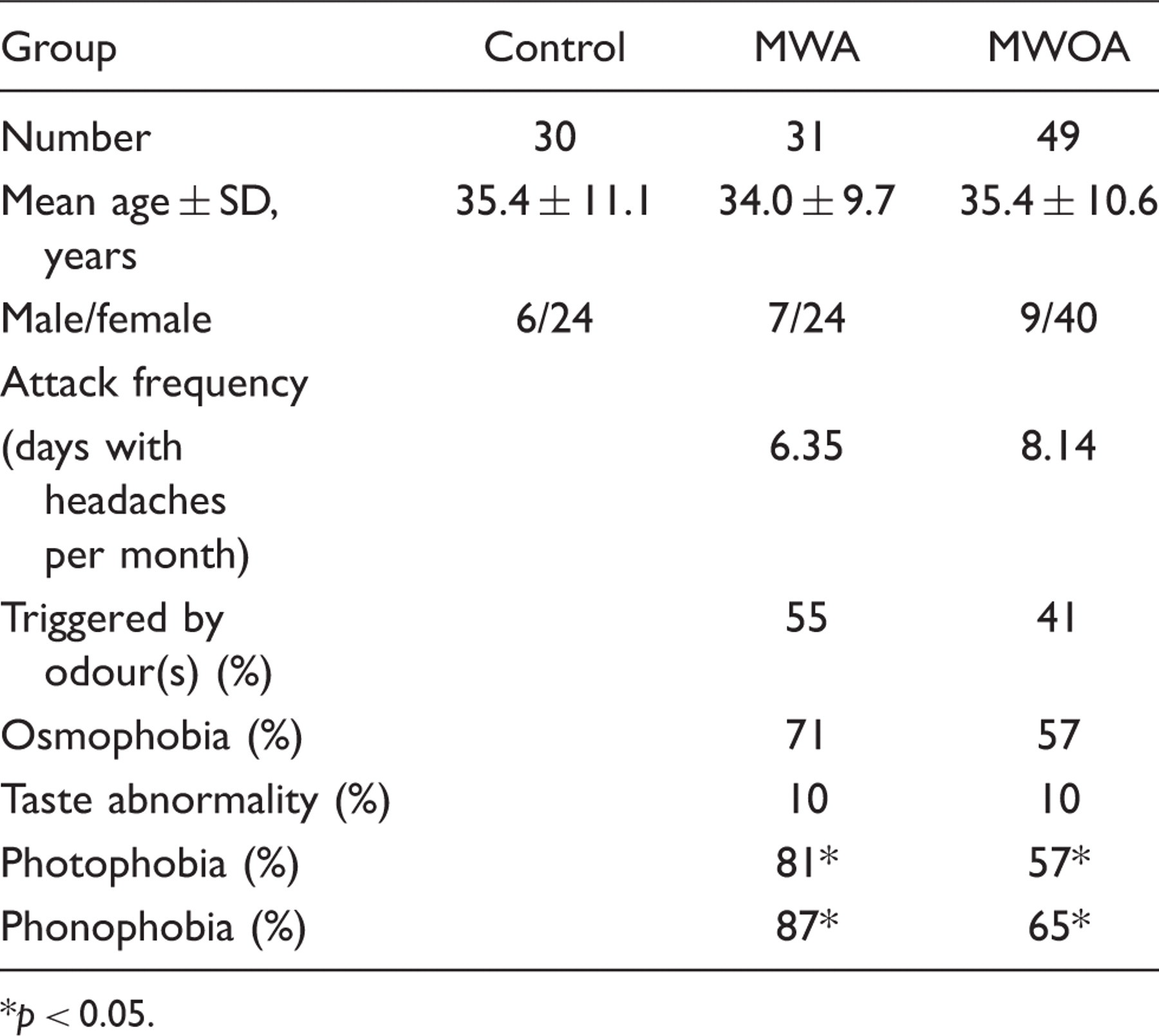
p < 0.05.
Details of odours reported to trigger headaches

Please answer all applicable questions and circle the correct response.
The onset of osmophobia occurred prior to migraine attacks in 46% of patients, within 30 min after attack onset in 52%, and ≥30 min after attack onset in very few patients (2%). Prodromal osmophobia was more frequent in MWA (57%) than in MWOA (37%) patients. The disappearance of osmophobia coincided with complete cessation of the headache in 71% of patients and persisted after the headache had subsided in 20% of patients.
Olfactory discriminative performances of patients with migraines did not differ from those of controls, with a correct answer rate of 91% (MWA, 92%; MWOA, 89%) versus 92%. The migraine patient group reported higher degrees of hedonic tone than the control group for the perfume, rose and Japanese cypress odours (Figure 1, p < 0.05). The MWA subgroup exhibited higher degrees of hedonic tone than the MWOA subgroup for clothes smelling of perspiration, rose scents, and odours of cooking gas and curry (Figure 2, p < 0.05). The degree of hedonic tone for nearly all odour types was higher for patients with ≥ 6 migraine attacks/month (37 patients) than for those with <6 attacks/month (43 patients), with this tendency being especially prominent for the perfume, rose, cooking gas and Japanese cypress odours. The perfume, curry, rose, Japanese cypress and roasted garlic odours had stronger effects on hedonic tone in the osmophobia-positive than in the osmophobia-negative patients (Figure 3, p < 0.05). The perfume, curry, rose and Japanese cypress odours had stronger effects on hedonic tone in the osmophobia-positive patients than in healthy controls (Figure 3, p < 0.05).
Average odour hedonic tone degree scores for migraine sufferers and healthy controls using the odour stick identification test. The perfume, rose and Japanese cypress odours had stronger impacts on hedonic tone in migraine patients than in healthy controls (*p < 0.05). Average of odour hedonic tone degree scores for migraine with aura (MWA) and migraine without aura (MWOA) using the odour stick identification test. The MWA subgroup exhibited higher degrees of hedonic tone than the MWOA subgroup for curry, cooking gas and rose odours and for clothes smelling of perspiration (**p < 0.05). Average of odour hedonic tone degree scores in patients with osmophobia and healthy controls by OSIT. The perfume, curry, rose, Japanese cypress and roasted garlic odours had a stronger impact on hedonic tone in the osmophobia-positive (+) than in the osmophobia-negative (–) patients (***p < 0.05). The perfume, curry, rose and Japanese cypress odours had a stronger impact on hedonic tone in the osmophobia-positive patients than in healthy controls (***p < 0.05).


The taste tests revealed no differences in gustatory sensation (hypogeusia or hypergeusia) between migraine patients and controls or between the MWA and MWOA subgroups.
Discussion
Few investigations have focused on hyperaesthesia in migraine sufferers. Furthermore, even fewer studies have been conducted on osmophobia than on photophobia or phonophobia. Thus, the relationship of osmophobia with migraines is poorly understood. Recently, the field of olfaction has become the focus of increased interest and investigation. Since the demonstration that olfactory dysfunction often develops in the early stages of degenerative brain disorders such as Parkinson’s and Alzheimer’s diseases, studies exploring dysosmia as a potential early diagnostic indicator for these disorders have been carried out (4,5). In Japan, the OSIT used herein is the most commonly used tool for such studies. The OSIT is an olfactory test developed by Saito et al. (3) primarily as a screening test for dysosmia in the Japanese population. Unlike conventional olfactory tests, it requires no special testing apparatus, entails no indoor odour pollution, and is a simple and rapid test, which can be performed in the outpatient setting. The olfactory identification tests developed and in widespread use overseas include the Pennsylvania Smell Identification Test (6) in the United States, its international version the Cross-Cultural Smell Identification Test (7), and the Sniffin’ Stick (8) in Germany. In Japan, these testing schemes have the disadvantage of including odours unfamiliar to Japanese people. Therefore, we adopted the OSIT for assessing the degree of odour offensiveness in this study.
We found that some migraine patients experience hypersensitivity to particular odours even during attack-free periods. No difference in olfactory discriminatory performance was found between patients with migraine and controls. Snyder and Drummond (9) have reported that patients with migraine show a lower threshold than controls for sensing a vanillin odour, and Hirsch (10) reported that patients with migraine exhibited a higher threshold for sensing a pyridine odour. Our study did not measure olfactory thresholds, so no conclusion has been drawn in this respect. Demarquay et al. (11), who investigated olfaction in migraine patients using 12 types of odour, described patients with osmophobia as showing higher degrees of hedonic tone to various odours and higher frequencies of headache provocation by odours, in comparison with patients experiencing migraines without osmophobia and controls. In Asian countries such as Japan, however, there are no reports on the relationships of migraine headaches with olfaction. In addition to the many factors (such as stress, menstruation and insufficient sleep) implicated in precipitating migraine attacks, odour was found to be a precipitating factor in 46% of migraine patients in this study, in 45.5% of patients reported by Kelman (12) and in 25.3% of patients reported by Zanchin et al. (2). As regards the mechanism(s) whereby odours precipitate cephalalgia in migraine patients, it was suggested by Zanchin et al. (2) that according to Moskowitz’s trigeminal neurovascular theory, headaches may be triggered by odour stimulation of the trigeminal nerve in the nose (13). Migraine is considered to be a state of exaggerated hypersensitivity affecting the entire brain, evoking pain at the stage of cerebral cognition. Therefore, it is possible that during a migraine headache the brain recognizes certain odours as dangerous sensory information that would not be identified as such by the unaffected brain, and expresses this recognized danger in the form of a headache.
The rate of hypersensitivity concurrence found in the present study was higher than those reported in Japan by Takeshima et al. (14) for both the MWA and the MWOA subgroup with respect to photophobia and phonophobia. This may be due to variable symptom severities. In our outpatient migraine clinic, we see considerable numbers of patients with chronic headaches. Zanchin et al. (2) noted that 43.0% of 807 patients with migraines had osmophobia, with unusual sensitivity to cigarette smoke, perfume and coffee odours. Kelman (15) reported osmophobia in 24.7% and dysgeusia in 24.6% of 673 patients with migraines. The present series showed a higher osmophobia concurrence rate (63%) than previously reported studies. The degree of severity may account for this trend but ethnic or racial differences may also be contributory. A study comparing olfaction between Japanese and German populations (16) found the former to be more offended by perfume odours than the latter. This was attributed to an inter-racial difference in odour sensitivity, which may also have contributed to the greater degree of olfactory hypersensitivity observed in the present study. The comparatively lower degree of environmental odour stimulation in Japan may also be related to this trend. Humans regulate air flow through the nostrils to influence olfaction, but also form smell impressions through an accommodation process, thereby actively micro-regulating the sensations induced by smells.
The present OSIT data reveal that some migraine patients experience greater degrees of offensiveness in response to particular odours (perfume and rose odours) even during attack-free periods. The greater degree of hedonic tone observed for all odour types tested in MWA as compared with MWOA patients underscores the need for patient education to optimize the living environment, particularly for patients with MWA. These patients should be counselled to avoid perfumes and cigarette smoke as these have a strong impact on hedonic tone.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.