
Abstract
Objectives
The objective of this article is to characterize olfactory stimulation as a trigger of headaches attacks and differentiation between migraine and other primary headaches.
Participants and methods
The study was prospective and experimental, with comparison of groups. A total of 158 volunteers (73 men and 85 women) were diagnosed with primary headaches, according to the criteria of the International Classification of Headache Disorders, Third Edition (beta version) (ICHD-3β). The study was conducted by two examiners; one of them was assigned to diagnose the presence and type of primary headache, while the other was responsible for exposing the volunteers to odor and recording the effects of this exposure.
Results
Of the 158 volunteers with headache, there were 72 (45.6%) cases of migraine and 86 (54.4%) with other primary headaches. In both groups, there were differences in headache characteristics (χ2 = 4.132; p = 0.046). Headache attacks (25/72; 34.7%) and nausea (5/72; 6.9%) were triggered by odor only in patients with migraine, corresponding to 19.0% (30/158) of the sample, but in none with other primary headaches (χ2 = 43.78; p < 0.001). Headache occurred more often associated with nausea (p = 0.146) and bilateral location (p = 0.002) in migraineurs who had headache triggered by odor. Headache was triggered after 118 ± 24.6 min and nausea after 72.8 ± 84.7 min of exposure to odor.
Conclusions
The odor triggered headache attacks or nausea only in migraineurs. Therefore, headache triggered by odors may be considered a factor of differentiation between migraine and other primary headaches and this trigger seems very specific of migraine.
Introduction
Odors, pleasant or unpleasant, are volatile molecules and, when inhaled, they act as a stimulus to the olfactory system and trigger nerve impulses that are transmitted to the brain (1). In addition to its physiological function in olfaction, these substances are closely related to primary headaches (2–10).
Osmophobia, defined as an intolerance factor to odors, both during and between headache attacks and the triggering of headache attacks, is recognized as an action of odors in primary headaches (2,3,5,11–13). The literature is scarce regarding the role of odors in secondary headaches (14).
In low concentrations, often well tolerated by the patient (6), odors, especially perfume (4,6,7,9,10), trigger headache attacks almost exclusively in migraine patients in a frequency ranging from 28.8% to 70.0% (6,4,8,9,15,16), but there is one case report in which the odors trigger headache in patients with cluster headache (17).
Osmophobia during headache attacks occurs more frequently in migraine (2,5,10,18,19), but it has been reported in patients with tension-type headache and cluster headache in several studies (2,5,7,19,20). In the period between headache attacks, it is described only in migraines (3,5,8).
Despite the relevance of odors as a trigger of headache attacks in migraine patients, to date, no experimental study has been conducted to demonstrate that odors trigger headache attacks. All previous studies are observational and odor as a headache trigger was found in interviews with migraine patients.
Therefore, our research is important because this is the first experimental study conducted in order to characterize olfactory stimulation as a triggering factor of headache attacks and as a factor of differentiation between migraine and other primary headaches, in addition to determining the time of appearance of headache after exposure of the patient to odor.
Participants and methods
Study design and participants
This was a prospective, experimental study with comparison groups. The sample consisted of 158 participants (73 men and 85 women), who were diagnosed with primary headaches (72 with migraine and 86 with other primary headaches), according to the criteria of the International Classification of Headache Disorders, Third Edition (beta version) (ICHD-3β) (21). The sample was selected among medical students enrolled in a public university located in Teresina, Piauí, Brazil, who were invited to participate in this research.
The sample was stratified based on the definition of two classes: diagnosis of primary headache, established as migraine and other primary headaches; and headache triggered by odors, referred to as present or absent. After randomization, when a selected volunteer did not meet the inclusion criteria or did not want to participate, another one of the same sex was chosen.
Inclusion and exclusion criteria
Volunteers aged between 18 and 50 years, with a diagnosis of primary headache according to the diagnostic criteria of ICHD-3β (21), and who agreed to submit to an interview and olfactory stimulation that would integrate the research, were included in the study. The study excluded volunteers who reported daily or almost daily headache, no headache in the last 12 months, with an association between two or more primary headaches, concurrently or at different times, using migraine prophylaxis, secondary headaches, associated diseases or medications that compromised the olfaction, history of allergy to any of the perfume components inhaled, women with headache only during menstruation, and pregnant women.
All participants underwent a thorough medical history. Only primary headache, according to the diagnostic criteria of the ICHD-3β (21), were included in our research. When the participants did not meet diagnostic criteria for migraine, tension-type headache, trigeminal autonomic cephalalgias or other primary headache disorders (primary cough headache, primary exercise headache, primary headache associated with sexual activity, primary thunderclap headache, cold-stimulus headache, external-pressure headache, primary stabbing headache, nummular headache, hypnic headache and new daily persistent headache), the headaches were classified as secondary headaches and the individuals were excluded from the research.
Data collection
After the individuals fulfilled the inclusion and exclusion criteria, a structured interview was conducted by the first researcher, based on a questionnaire to diagnose the presence and type of primary headache. The second researcher was responsible for the exposure of volunteers to the odor and the recording of the effects of this exposure.
Although the study was not double-blind, there was a blinding by restricting to each examiner the information generated by them. The first researcher did not know which patients had headaches triggered by odors and the second researcher and patient did not know the diagnosis.
The olfactory stimulation was performed by inhalation of a floral scent source for 60 seconds by a volunteer who should have had no headache for at least 48 hours before the time of the olfactory stimulation. Next, he or she was monitored for 24 hours by telephone to detect the appearance of headache or other symptoms and when they appeared.
Statistical analysis
Once the information was organized in the database, the Epi Info™ 7, 7.1.5.0 version of 19 March 2015, for statistical analysis was used. The chi square test with Yates correction for differences between averages of unpaired samples was used, assuming a significance level of 0.05.
Ethical aspects
This study was approved by the Ethics in Research Involving Human Subjects Committee at the State University of Piauí, Brazil, protocol number 273.768 and the Presentation Certificate to Ethics Assessment, registry number 12743813.4.0000.5209, on May 16, 2013. All participants signed the informed consent form.
Results
The sample studied consisted of 158 volunteers, 73 men and 85 women who reported headaches and were characterized by a mean age of 22.7 ± 3.1 years, ranging between 18 and 34 years old.
Distribution of established diagnoses for 158 volunteers.

Percentage calculated on the total of the respective category.
Considering only the cases diagnosed with headache, the group with migraine had an average age of 22.5 ±3.1 years and a median of 22.0 years. In the group with other primary headaches, the average age equaled 22.9 ± 3.1 years and a median of 22.5 years. These differences were not significant (tmean = 0.666; p = 0.566).
Distribution of characteristics of established diagnoses for 158 volunteers with headache.

p values calculated using the chi-square test, comparing: a<20 episodes in the last 12 months versus ≥ 20 episodes in the last 12 months; bheadache attacks lasting < 4 hours versus ≥ 4 hours; cunilateral versus bilateral or irregular; dpulsatile versus dull/pressure or stabbing. eThree (4.2%) migraineurs could not inform about worsening headache with physical activity.
In the other primary headaches, more frequent characteristics were male (62.8%), varying from one to more than 20 headache attacks in the last year (61.6%), duration of less than 4 hours (72.1%), bilateral location (75.6%), characterized by dull/pressure or stabbing (87.2%), and photophobia or phonophobia (48.8%) as associated symptoms. Note that six (3.4%) volunteers referred to osmophobia as a symptom of migraine, isolated or associated with other symptoms (Table 2).
When considering the characteristics of headache for differentiation of volunteers with migraine from those with other primary headaches, it was found that the two groups were statistically distinct (χ2 = 4.132; p = 0.046).
Among the 158 volunteers who underwent olfactory stimulation, there were 30 (19.0%) patients who presented a triggering of headache or other symptom without headache. All 30 patients were diagnosed with migraine, thus characterizing the positivity of olfactory stimulation. This difference was significant compared with those who had other primary headaches (χ2 = 43.78; p < 0.001).
Distribution of the frequency of positivity of olfactory stimulation is observed in Figure 1, according to the established diagnosis for 158 individuals with primary headaches. In 34.7% (25/72) of migraineurs, headache with and without associated symptoms was triggered by odor and in 6.9% (5/72) only nausea without headache was triggered by it.
Distribution of the frequency of headache after olfactory stimulation, according to the diagnoses of 72 volunteers with migraine and 86 with other primary headaches.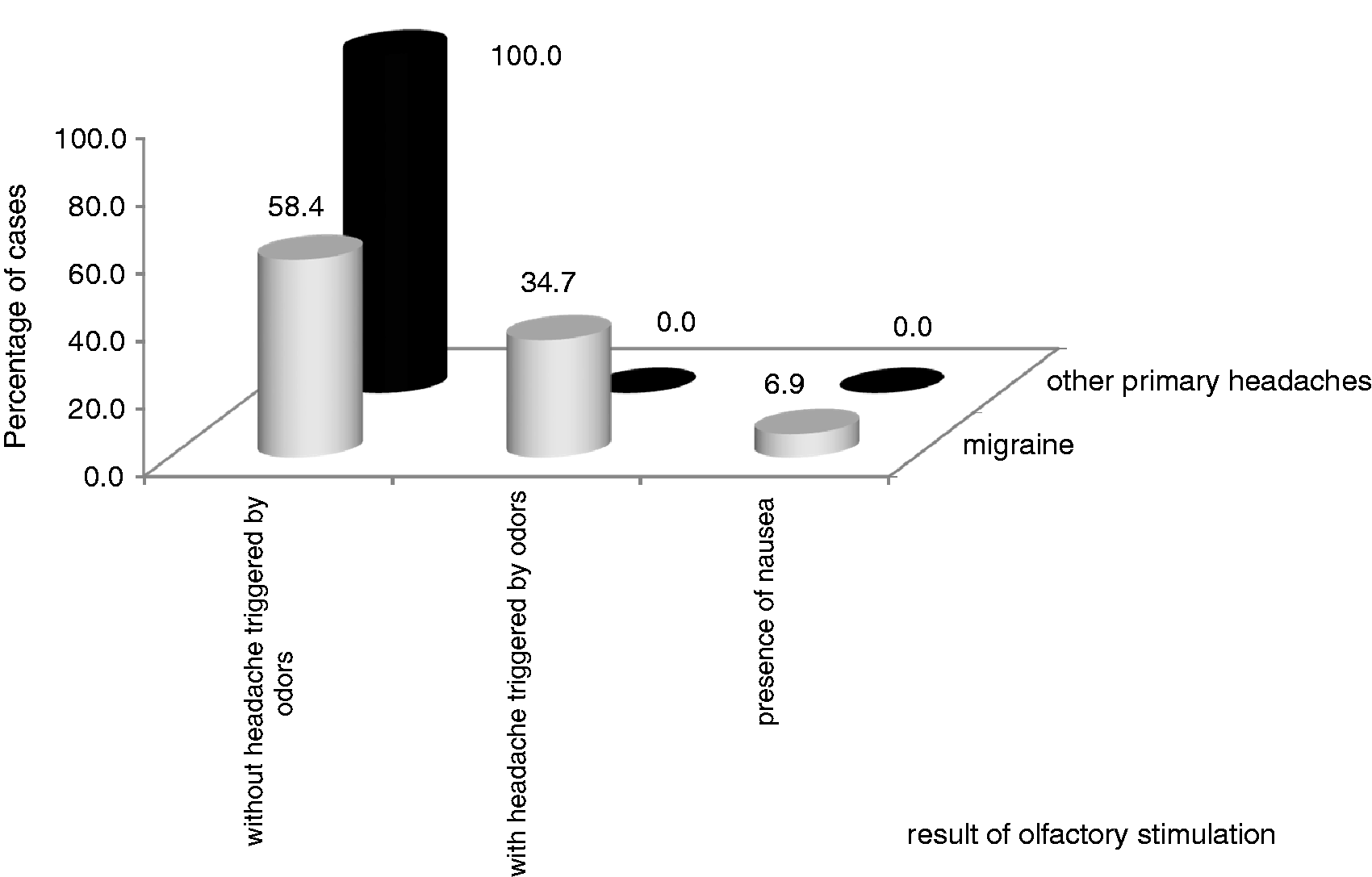
Distribution of the characteristics of migraine in 72 migraineurs according to the presence of headache triggered by odors.
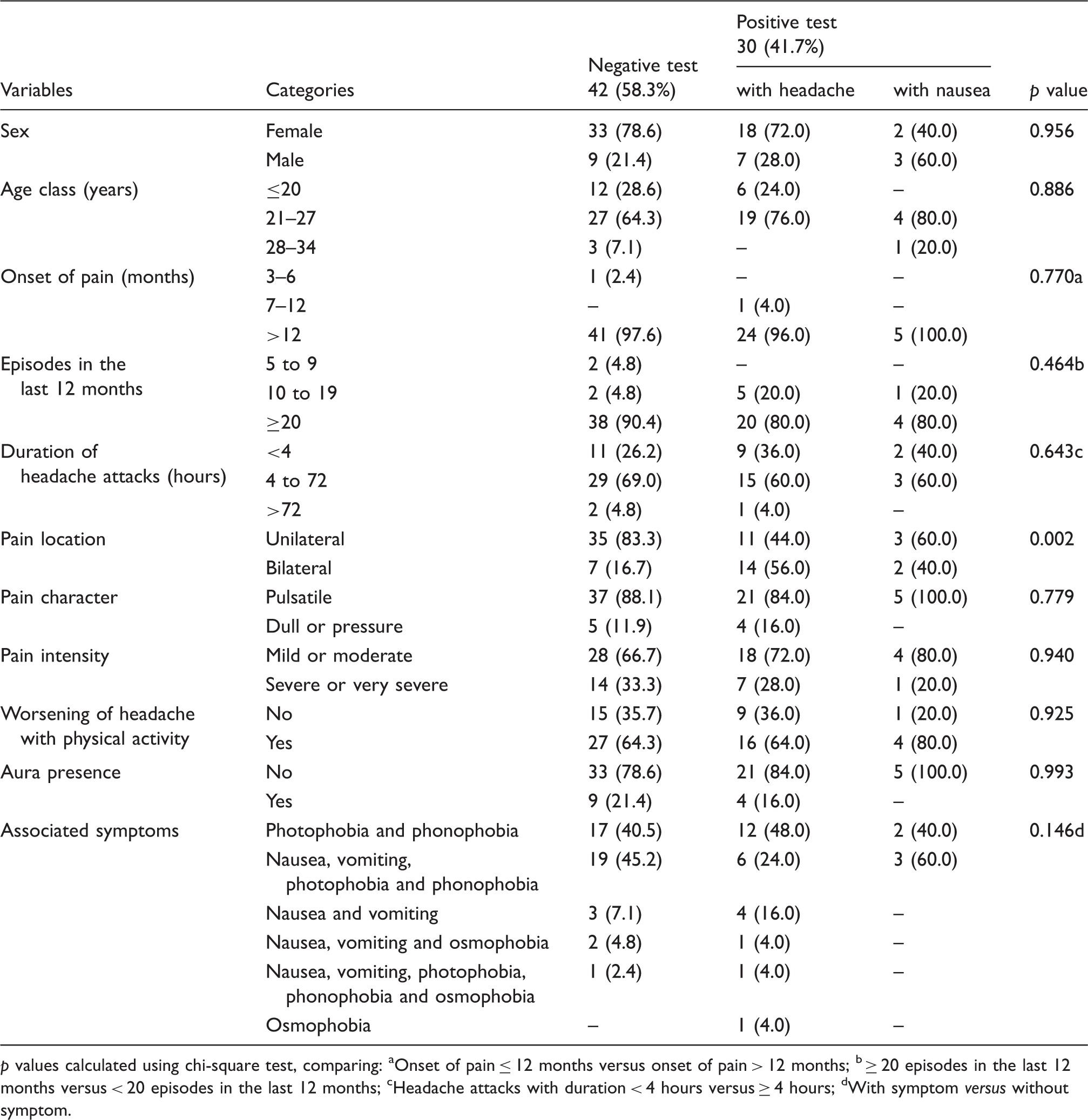
p values calculated using chi-square test, comparing: aOnset of pain ≤ 12 months versus onset of pain > 12 months; b ≥ 20 episodes in the last 12 months versus < 20 episodes in the last 12 months; cHeadache attacks with duration < 4 hours versus ≥ 4 hours; dWith symptom versus without symptom.
Nausea after the olfactory stimulation came about isolated from other complaints, differently from what was reported by migraineurs during the interview when the nausea was always associated with other manifestations of migraine.
Regarding the location of the pain, there was a significant difference between the groups with positive and negative olfactory stimulation. In the migraineurs in whom the olfactory stimulation triggered only nausea, pain was reported more frequently in a unilateral location. However, when the odor triggered headache, pain was most often bilaterally located (Table 3).
Regarding the time interval for positivity of olfactory stimulation, the mean was 118 minutes (SEM =24.6 minutes) and the median was 60 minutes (interquartile range (IQR) = 8–206 minutes) for the triggering of a headache; and an average of 72.8 minutes (SEM = 84.7 minutes) with a median of 22 min (IQR = 0–252 minutes) for the appearance of nausea. Significant differences were observed between the group with headache triggered by odor and the group with only nausea when compared to the group in which the odor did not induce headache, as shown in Figure 2.
Distribution of frequency, mean and median time of onset of headache and associated symptoms of 30 migraineurs.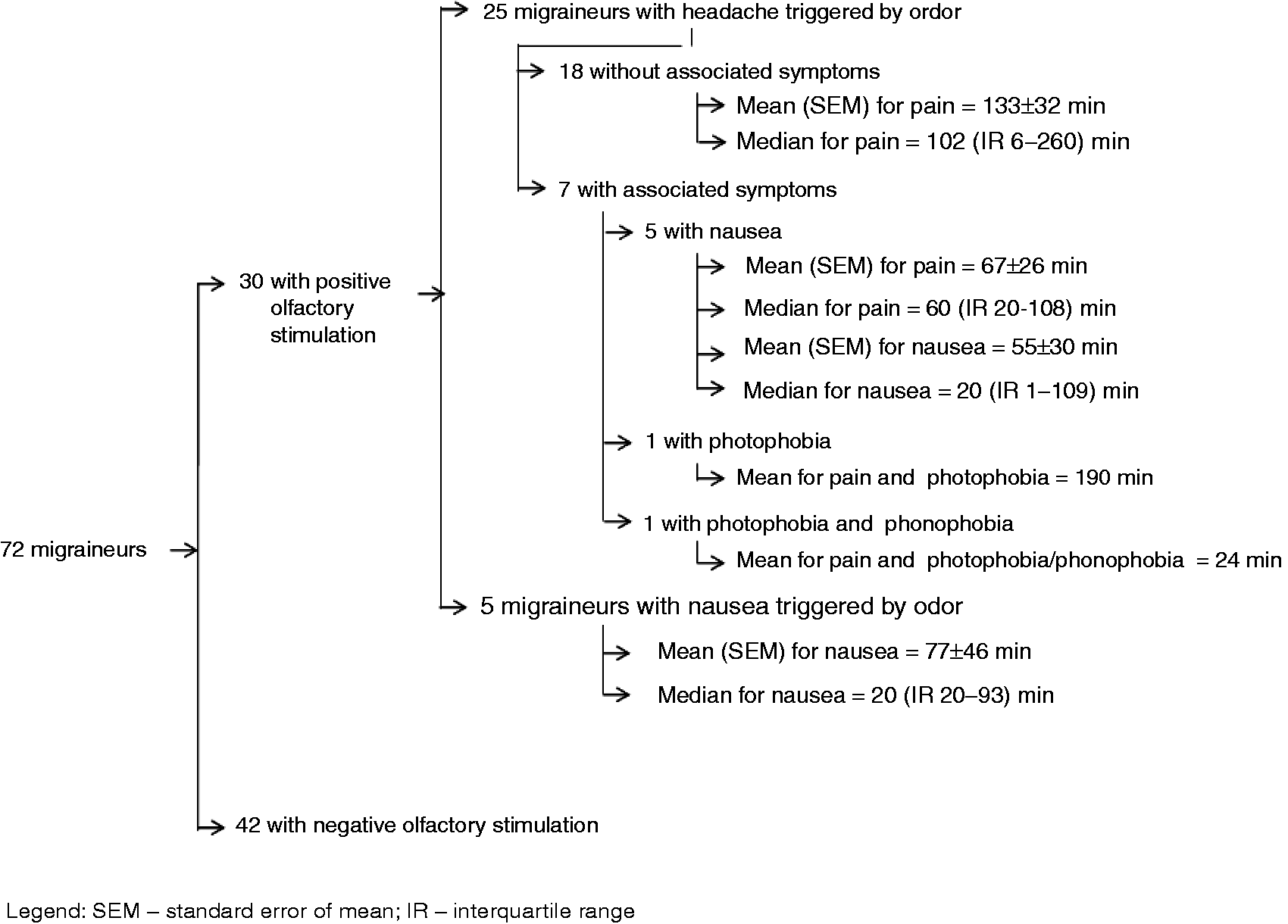
Distribution of mean and median elapsed times to onset of headache or nausea odors by 30 migraineurs with positive olfactory stimulation.
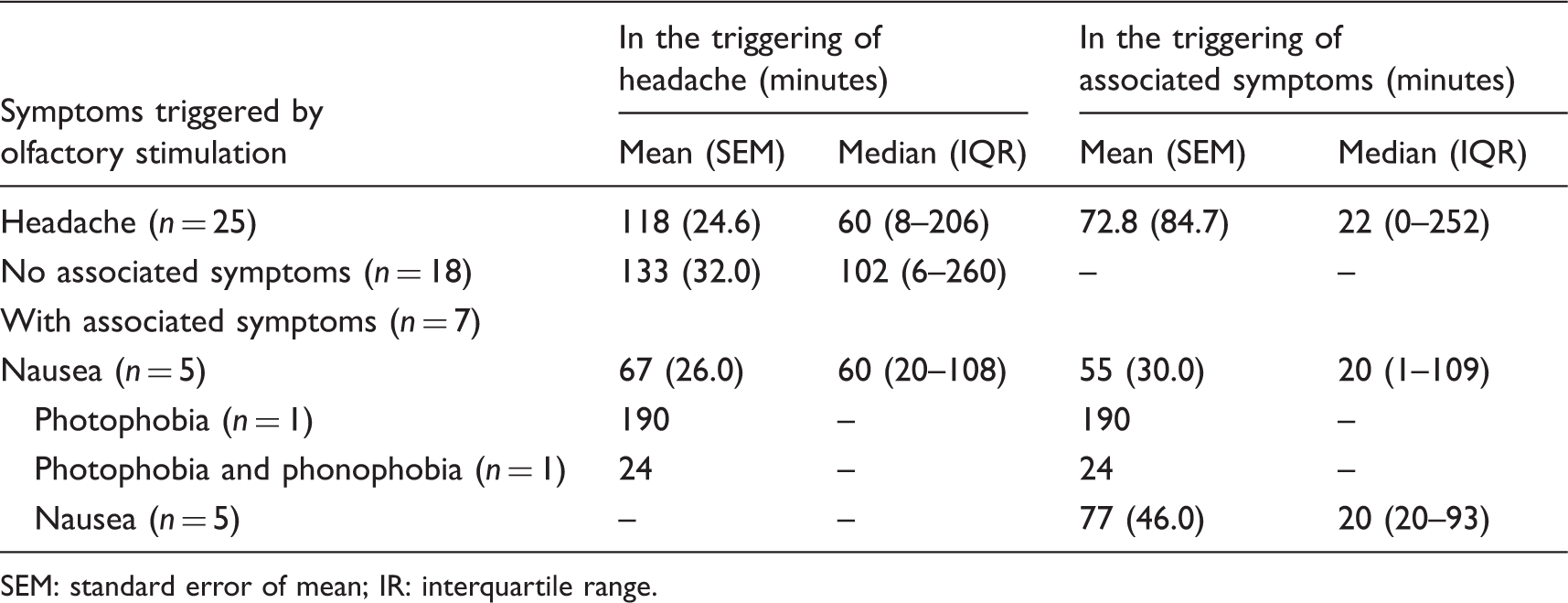
SEM: standard error of mean; IR: interquartile range.
Discussion
In this study, two groups of volunteers diagnosed with migraine or other primary headaches were compared by olfactory stimulation to evaluate odor as a trigger of headache or other symptoms. Therefore, in order to obtain consistent and valid data, a correct diagnosis was established for each headache (Table 1), according to the criteria of ICHD-3β (21).
In addition, we opted for the description of the characteristics of pain and associated manifestations, as these variables are specific to each headache, especially migraines, which may be used to differentiate between groups, as demonstrated in this study (Table 2).
The average age of the volunteers was low when we compare to other studies. Most authors found ages ranging between 38 and 44 years old (2–5) because the sample was from the general population. In our study, the volunteers were young medical students, whose ages ranged from 18 to 27 years old. Only one of them was 34 years old.
The perfume was selected for the olfactory stimulation because numerous studies have shown that it is the main odorant substance capable of triggering headache attacks in migraine patients (4,6,7,9,10). Other odorants also trigger headache when inhaled, but some should not be used in researches because of ethical implications, carcinogenic action and stimulation of nociceptive endings of the trigeminal nerve (22).
When migraine patients who have headache attacks triggered by odors are asked about the type of fragrance, half of them identify the scents with a floral source (10). Therefore, we have chosen a floral scent for olfactory stimulation of the participants of this research.
When there is increased olfactory acuity, odors in low concentrations are able to trigger headache attacks (23). Furthermore, olfactory sensitivity may be influenced by hormonal changes. Thus, more often, pregnant women and women with headaches only during menstruation present with, respectively, hyperosmia (24,25) and osmophobia (26,27). This explains why these women were not exposed to the odor in our study.
It was found that the odor triggered headache or nausea exclusively in volunteers diagnosed with migraine (Figure 1). The olfactory stimulation causing nausea without headaches indicates that this is also a characteristic of migraine and may differentiate it from other primary headaches. These findings were similar to previous studies that also showed odors as triggers of migraine. In these studies, odors only triggered headache (4,6,8,9).
In our study, 34.7% of migraineurs had headaches triggered by odor, according to several previous observational studies, in which the odor triggered headaches in 28.8% to 70.0% of these patients. Moreover, none of these studies reported headache triggered by odors in other primary headaches either (4,6,8,9,15,16).
In view of the positive and negative results (41.7% versus 58.5%) of the olfactory stimulation in migraineurs, we compared them since they appeared to be different groups. For this, we have analyzed the variables that integrate the diagnostic criteria of the ICHD-3β and that are used to define each group (Table 3). In these diagnostic criteria, migraine is characterized by unilateral location of the pain and the presence of nausea and/or vomiting associated with headaches (21).
We found that migraine characteristics are different when the headache attacks are triggered by odors. In most migraineurs headache was located bilaterally and nausea was the only concomitant symptom.
In the migraineurs who presented with positive olfactory stimulation, we have determined the time of onset of headache or nausea (Table 4 and Figure 2). We found that the mean time to the onset of headache was longer than that described in a previous study (25 minutes versus 133 minutes). This prior study was observational and it did not report the time of onset of nausea (4).
We do not know how long it takes to trigger headache attacks in migraine patients. So we may not say that the time of onset of headache attacks was long in this study because we have no comparative studies, and to the best of our knowledge, this is the first experimental study on triggering headache by odor.
There is another characteristic that appears to be specific for migraine when the olfactory stimulation is positive. In this case, nausea is a symptom that occurs prior to headache and remains present after the olfactory stimulation. Furthermore, the odor may trigger nausea only.
There is much evidence of the association between odor and primary headaches, especially migraine, but despite this knowledge, the exact mechanism of action of the odors as migraine triggers is not known. However, one study showed increased activity of the limbic and brainstem during migraine attacks following olfactory stimulation, only for migraine patients. This finding shows the strong relationship between smell and the trigeminal nociceptive pathway in the pathophysiology of migraine (1,22,28).
There is also a hypothesis that the olfactory stimulus excites the locus coeruleus in migraine patients and causes noradrenaline release. Consequently, substance P and calcitonin gene-related peptide (CGRP) are released. These two potent and inflammatory vasodilatory substances trigger the painful phenomenon (4).
Recent studies have shown that inhalation of certain odors may cause severe attacks of headache by stimulation of the transient receptor potential ankyrin 1 (TRPA1), a nonselective cation channel expressed in sensory neurons, and also by activation of the trigeminovascular system. Consequently, there are nociceptive responses and release of CGRP from trigeminal nerve terminals in the dura mater. Furthermore, TRPA1 activation may activate dural nociceptors and lead to central sensitization and cutaneous allodynia (1,29,30).
The knowledge that odors are triggers of migraine and time to onset of headache after exposure to the odor is based on observational studies, in which patients expressed their opinions in response to the researcher’s questions. Unlike this study, migraineurs underwent olfactory stimulation and the effects of the odors and were observed.
Conclusions
Odor triggered headache attacks or nausea only in migraineurs. Therefore, headaches triggered by odors may be considered a factor of differentiation between migraine and other primary headaches, and this trigger seems very specific of migraine.
Clinical implications
Odors trigger headache attacks in migraine patients. Olfactory stimulation is a factor of differentiation between migraine and other primary headaches.
Footnotes
Acknowledgment
The authors thank teacher João Lívio Norberto for his help with the English language.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.