
Abstract
This study evaluates osmophobia and taste abnormalities in relationship to sensitivity and specificity in the classification of migraine. Consecutive International Headache Society (IHS) classified patients (n = 1237) were evaluated. Symptoms were graded from 0 to 3. Osmophobia and taste abnormalities were tested for sensitivity and specificity in migraine diagnosis. The patients were 85.4% female and their mean age was 38.1 years. Of 673 patients 24.7% complained of osmophobia, and 24.6% of 505 complained of taste abnormalities. In the absence of nausea and vomiting the combinations of two symptoms gave the following sensitivity and specificity percentages, respectively: photophobia and phonophobia, 10.6 and 84.9; photophobia and osmophobia, 1.1 and 99.0; phonophobia and osmophobia, 1.1 and 98.6; photophobia and taste abnormality, 9.6 and 99.0; phono-phobia and taste abnormality, 9.6 and 98.8; and osmophobia and taste abnormality, 4.2 and 99.4. Osmophobia and taste abnormalities were demonstrated to be very specific in diagnosing migraine IHS 1.1-1.6, but very insensitive.
Introduction
The International Headache Society (IHS) Classification of Headaches in 1988 provided a monumental advance (1). It provided a firm basis for comparing patient groups in research and clinical practice. The system continues to be refined. One area of interest has been in the fine-tuning of the associated symptoms category (category D) of the operational criteria for the diagnosis of migraine. In the absence of nausea and vomiting, light and sound intolerance are required for the diagnosis of migraine. The issue has arisen whether osmophobia may play a useful role in defining migraine in this category. (Appendix to proposed International Headache Classification, 2nd Edn). Also neglected has been associated taste abnormality in migraine. The current study was performed for the purpose of defining the sensitivity and specificity of osmophobia and taste abnormalities in a large clinical sample of migraine patients in the diagnosis of migraine.
Patients and methods
Study population
The study population consisted of men, women, and children suffering from the full range of the IHS-defined migraine with or without aura. Patients were treated by the author in his clinical practice and the data accumulated in a database at the time of the visit.
Patients were excluded from the database if they had: (i) had no headache; (ii) headaches thought to be related to trauma or injuries; (iii) complicated neurological problems, i.e. underlying brain or systemic illness related to their headaches; (iv) recent onset headaches, i.e. less than 1 month prior to study; (v) significant legal issues related to their headaches; (vi) been seen prior to the initiation of the database; (vii) declined to, or were cognitively not able to participate in the database interview; and (viii) language or intellectual barriers. Patient data were recorded at the initial visit. Semistructured interviews were performed. This is a retrospective study and data were accumulated in the usual course of patient management. Many patients already used diaries and calendars, and some consulted the author's website for sampling the type of information required. If the patient was uncertain of the information, that variable was omitted. Institutional review board approval for use of the data without specific patient approval was obtained. Confidentiality was preserved by omitting the identification of patients when the data were downloaded to the statistical package.
Study design
Eligible headache patients at the author's clinic seen consecutively between July 2000 and May 2003 were included in a database. Patients were subjected to a headache evaluation, based on their past month typical headache characteristics, as well as a physical and neurological examination. A thorough medical history was also recorded. Osmophobia and taste abnormalities in particular, and other associated symptoms such as nausea, vomiting, photophobia, phonophobia, dizziness, diarrhoea, running of the nose or tearing of the eyes, were evaluated for sensitivity (positive finding of symptom(s) in patients with IHS migraine 1.1–1.6) and specificity (negative symptom(s) in patients who were not diagnosed with IHS migraine 1.1–1.6). Also included were other migraine features (not necessarily related to classification) such as headache waking patient from sleep, worsening of headache with activity, headache intensity (>3/10 and > 6/10), degree of unilateral headache, throbbing quality, and family members with headache, to provide a broader perspective of the associated symptoms findings.
Patient symptom rating
At the initial visit, patients were asked to rate their response to questions on a scale of 0 = never; 1 = occasional (1–33%); 2 = frequent (34–66%); 3 = very frequent (67–100%) in their typical headache.
Statistical analysis
Sensitivity was obtained by dividing the positive symptom(s) frequency in patients with a definitive diagnosis of IHS migraine 1.1–1.6 by the total number of patients with that diagnosis and expressed for patients with grades 1 through 3, grades 2 and 3, and grade 3. Specificity was obtained by dividing the negative symptom(s) frequency in patients who did not have a diagnosis of IHS migraine 1.1–1.6 by the total number of patients who did not have that diagnosis and expressed for patients with grades 1 through 3, grades 2 and 3, and grade 3. This analysis was performed in patients with no nausea or vomiting and also in patients without the restriction of no nausea or vomiting.
Results
Demographic characteristics
Of the 1237 patients seen by the author at the initial visit, 85.4% were females. The mean (± SD) age of patients was 38.1 (11.84) years (range 12.9–80.5).
Headache diagnosis (Fig. 1)
Based on headache characteristics on initial evaluation, 727 patients were diagnosed with IHS 1.1–1.6 migraine (99% IHS 1.1–1.2), 330 as migraine 1.7, 93 as tension-type headache 2.1–2.2, and 87 as ‘other’ which were patients not diagnosed in one of the former groups (31% cluster IHS 3.1–3.3; 16% trigeminal neuralgia IHS 12.2; 53% headache not classifiable IHS 13). Of the IHS 1.1–1.6 patients, 36% reported aura varying from 1% to 100% of migraine attacks.
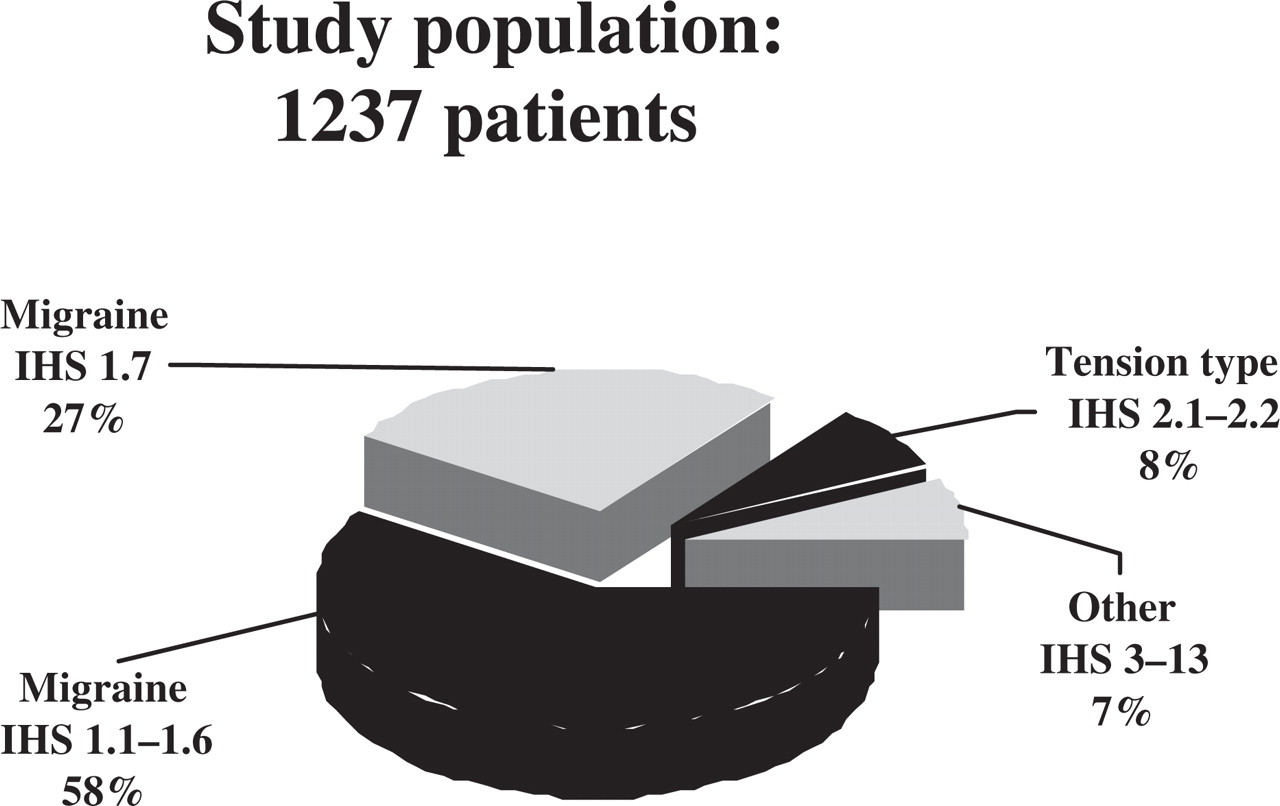
Population studied.
Osmophobia and taste frequencies
Of the data available, 166 of 673 patients (24.7%) complained of osmophobia during migraine headaches (12.5% mild, 7% moderate, and 5.2% severe). One hundred and twenty-four of 505 (24.6%) complained of taste abnormalities (13.5% mild, 6.1% moderate, and 5.0% severe).
Associated symptoms, sensitivity and specificity in the diagnosis of migraine IHS 1.1–1.6 (Table 1)
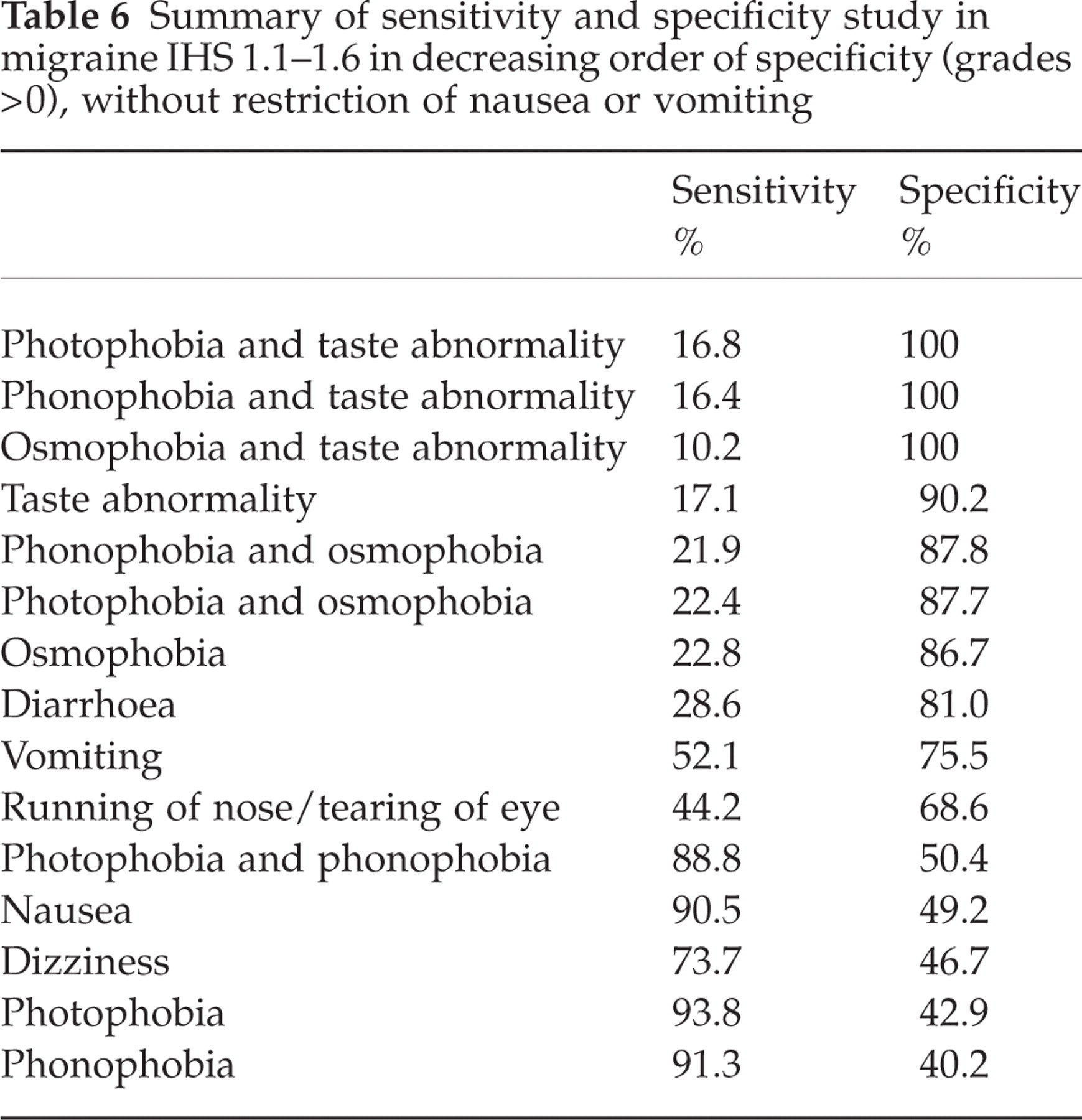
In diagnosing migraine in the absence of nausea and vomiting the combination of two of the associated symptoms gave the following sensitivity and specificity percentages, respectively: photophobia and phonophobia, 10.6 and 84.9; photophobia and osmophobia, 1.1 and 99.0; phonophobia and osmophobia, 1.1 and 100; photophobia and taste abnormality, 9.6 and 99.0; phonophobia and taste abnormality, 9.6 and 98.8; osmophobia and taste abnormality, 4.2 and 99.4. Surprisingly, in the absence of nausea and vomiting either osmophobia or taste abnormality alone gave a specificity of 98.4%. Vomiting alone (grade 3) gave a specificity of 97.5% and any running of the nose/tearing of the eyes, without nausea or vomiting, 92.2%. Increasing grades of symptom severity decreased sensitivity and increased specificity across all associated symptoms. In patients when nausea and vomiting were not excluded, sensitivity increased markedly but specificity decreased. In all situations, increasing the grade of symptom impacted significantly on the findings. (See Tables 2–6.)
Sensitivity and specificity of two of photophobia, phonophobia, osmophobia, or taste abnormality in migraine IHS 1.1–1.6 – no nausea or vomiting

∗Sensitivity = number of patients with symptom/total IHS 1.1–1.6.
†Specificity = 100 minus (number of patients with symptom/total not IHS 1.1–1.6).
Summary of sensitivity and specificity study in migraine IHS 1.1–1.6 in decreasing order of specificity (grades > 0), without restriction of nausea or vomiting
Sensitivity and specificity of single associated symptoms in migraine IHS 1.1–1.6 in patients with no nausea or vomiting

∗Sensitivity = number of patients with symptom/total IHS 1.1–1.6.
†Specificity = 100 minus (number of patients with symptom/total not IHS 1.1–1.6).
Sensitivity and specificity of single associated symptoms in migraine IHS 1.1–1.6 in patients without restriction of nausea or vomiting
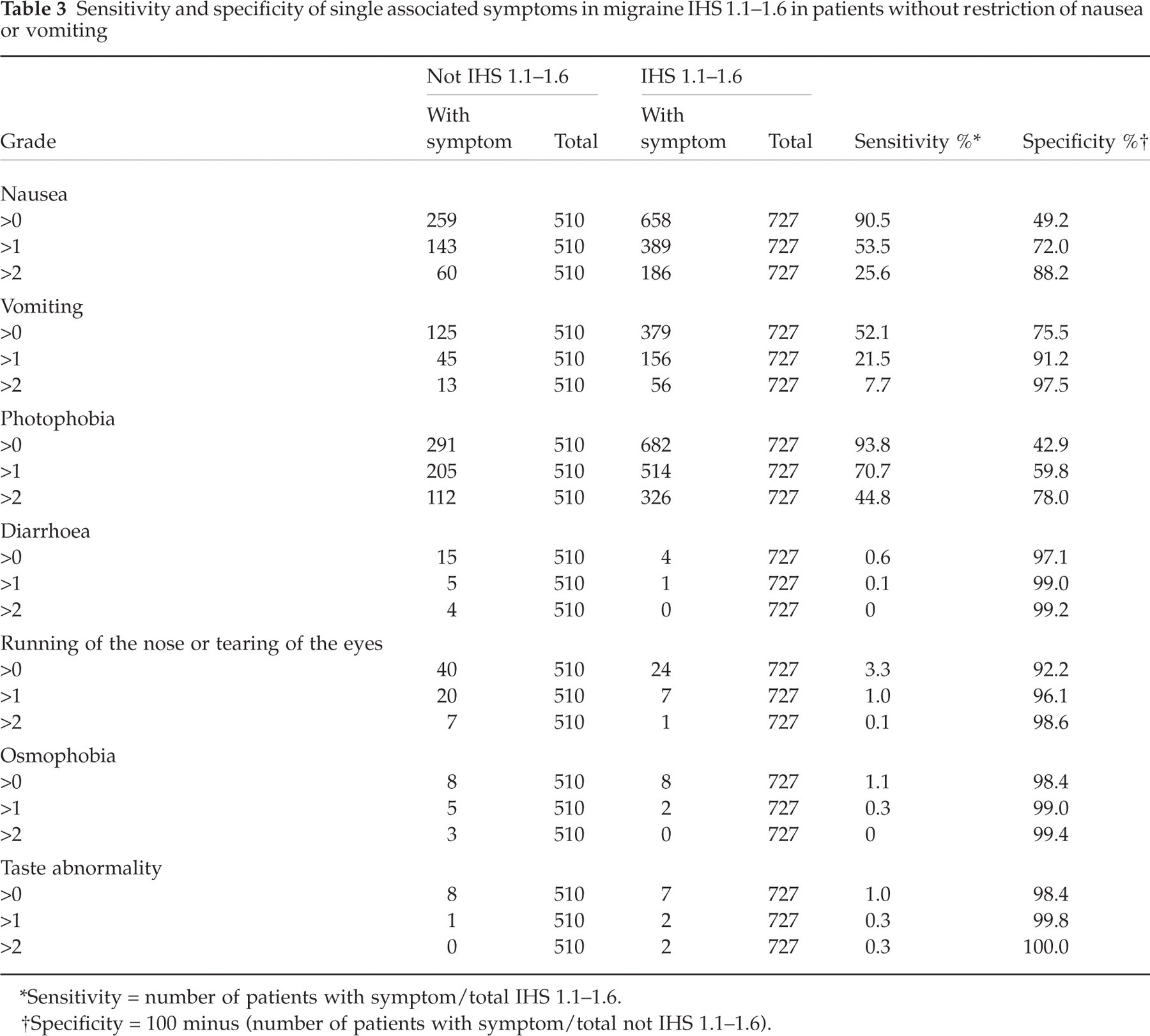
∗Sensitivity = number of patients with symptom/total IHS 1.1–1.6.
†Specificity = 100 minus (number of patients with symptom/total not IHS 1.1–1.6).
Sensitivity and specificity of single features in migraine IHS 1.1–1.6 in patients without restriction of nausea or vomiting

∗Sensitivity = number of patients with symptom/total IHS 1.1–1.6.
†Specificity = 100 minus (number of patients with symptom/total not IHS 1.1–1.6).
Summary of sensitivity and specificity study in migraine IHS 1.1–1.6 in decreasing order of specificity (grades > 0), no nausea or vomiting

Discussion
This study evaluates osmophobia and taste abnormalities during migraine attacks in a large sample of IHS 1.1–1.6 diagnosed patients in migraine classification.
Overall, osmophobia and taste abnormalities are sparsely mentioned in current headache texts (2, 3), and even less so is migraine mentioned in the authoritative olfaction and gustation text (4). There are limited reported studies of osmophobia and taste pertaining to migraine in the literature. Strong odours are described as a trigger of migraine (5, 6). Sensitivity to odours and olfactory hallucinations are described in migraine (7–11). Olfactory or taste symptoms during migraine were described in 13% of 64 patients) and 10.9% of 46 women reported olfactory hallucinations (12). Blau documented a frequency of osmophobia in 25 of 50 ‘migraine’ patients (13). The current study shows a lower percentage of patients having osmophobia. Taste is very similar to osmophobia in the current study. This is hardly surprising. Anosmic patients complain of abnormal taste, but it is primarily flavour that is affected. However, they may also complain of less sensitive sweet and salt taste (14). The absence of osmophobia in the current study had less effect on taste abnormalities (40% of the original numbers) than the absence of taste abnormalities had on osmophobia (28.3%).
The IHS 1988 classification is a unique document. It has provided an operational guideline for the working diagnosis of most headache types and situations, and provided standardization for comparing populations of patients in clinical and drug studies. Almost more important has been the huge outpouring of literature, thought, and research that the classification has evoked (15–33). Not all reports have been favourable but, as in any system, improvements can and will be made over the years. The ultimate classification will depend on biological data combined with clinical data.
The area of interest in this study is the classification of patients using osmophobia and/or taste abnormalities in category D of the IHS 1988 classification in the absence of nausea and vomiting. Do these symptoms have a place in the diagnosis of migraine? Clearly, this study demonstrates the remarkable specificity of both osmophobia and taste abnormalities either alone or combined with one another or with other associated symptoms (always above 98% and contrasted with other associated symptoms and also other features of migraine not necessarily related to classification). However, they do not add any extra patients that would not have been already diagnosed by the current 1988 IHS classification. This reflects on the basic strength of the current classification. This analysis needs to be replicated using a different population of patients.
This study explores the phenomena of osmophobia and taste abnormalities with particular reference to classification of migraine. Osmophobia and taste abnormalities were demonstrated in this study to be very specific in diagnosing migraine IHS 1.1–1.6, but very insensitive. Few, if any, additional patients would be diagnosed as having migraine who would not normally be diagnosed under the current 1988 IHS classification.