
Abstract
Introduction
People with migraine often report being osmophobic, both during and between acute migraine attacks. It is not clear, however, whether such reports are associated with changes in olfaction such as hyperosmia, as measured by psychophysical testing. In this case-control study we quantitatively assessed olfactory identification ability, which correlates with threshold tests of olfactory acuity, in patients with migraine at baseline (no headache), during migraine episodes, and after a treated attack and compared the test scores to those of matched control subjects.
Methods
Fifty episodic migraine subjects and 50 and sex- and age-matched controls without headache were tested. All completed the University of Pennsylvania Smell Identification Test (UPSIT), a standardized and well-validated olfactory test.
Results
At baseline, the UPSIT scores did not differ significantly between the migraine and control study groups (median paired score difference: −1, p = 0.18). During migraine attacks, a minority of migraine subjects (eight of 42) developed microsmia (i.e. lower test scores by at least four points), suggesting that, as compared to their matched controls, olfactory acuity was somewhat impaired during migraine attacks (p = 0.02). This difference was less pronounced and not statistically significant after a successfully treated attack (p = 0.15).
Discussion
People with episodic migraine were found to have similar olfactory function as age- and sex-matched controls, but a minority exhibit microsmia or hyposmia during acute attacks. The cause of this dysfunction is unknown, but could relate to autonomic symptoms, limbic system activation, or disorders of higher order sensory processing.
Introduction
Migraine is a complex neurologic disorder related to genetic and environmental factors consisting of headache, gastrointestinal symptoms, and multiple sensory disturbances including photophobia, phonophobia, and osmophobia in the absence of a causative secondary disorder. Hypersensitivity to sensory stimuli such as light and sound are classical diagnostic features of migraine (1), although migraineurs are also more likely than other people to be bothered by odors. In fact, osmophobia may be a more specific symptom in differentiating migraine from other headache disorders (2,3), and including it as a diagnostic criterion may increase the sensitivity for accurately diagnosing migraine in populations where photophobia is less common (4). Osmophobia is most prominent during acute migraine attacks, but discomfort may persist interictally in a subset of migraineurs (5,6).
Olfactory impairment is a common symptom found in a number of neurologic disorders, such as Parkinson's disease, schizophrenia, and myasthenia gravis (MG), possibly due to degeneration and/or dysmodulation of dopaminergic, serotonergic, and cholinergic systems (7). Multiple studies have confirmed that migraine subjects are bothered by odors, especially noxious stimuli (8,9), and that odors may precipitate attacks. One H2O-positron-emission tomography (PET) study showed abnormal cerebral activation patterns during olfactory stimulation in migraineurs with olfactory hypersensitivity (10). The ability of people with migraine to detect and discriminate odors, as determined by standardized olfactory testing, is less clear. In one study, a large number of migraine subjects had poor olfactory acuity (11), as measured by olfactory thresholds, and in another migraineurs had increased odor detection (12). A more recent study of episodic migraine subjects found that their olfactory acuity was normal (5). The effect of a migraine attack on olfactory ability during and after treated attacks is also unclear.
The objective of this study was to examine olfactory acuity in episodic migraine subjects as compared with age- and sex-matched controls, using a reliable and well-validated test of olfaction. We also evaluated the effect of acute migraine on olfactory acuity—both during and after a treated attack.
Methods
Formal approval of this study was obtained from the institutional review board at Thomas Jefferson University. Subjects ranging in age from 18 to 65 were recruited from our clinic and the surrounding community who were diagnosed with episodic migraine, as defined by the International Classification of Headache Disorders, second edition. Each subject completed a headache history to ensure the correct diagnosis and determine medications and headache frequency. We excluded subjects or controls with a history of significant headache trauma, nasal or sinus disease, or neurologic disorders such as Parkinson's disease, dementia, or multiple sclerosis. Individuals who used medications that could influence smell function, such as anticonvulsants or opioids, barbiturates or neuroleptics—drugs often used to treat attacks—were excluded from consideration. Subjects were allowed to use nonsedating simple or combination analgesics such as nonsteroidal anti-inflammatory medications, including those with caffeine, and migraine-specific medications such as triptans. To ensure that we could determine the effect of a treated migraine on olfaction, we also excluded subjects with long-lasting migraines that may not respond to medication. As ours is a tertiary headache center with many refractory patients not meeting criteria for episodic migraine, we decided to verbally recruit subjects from the community, including subjects already participating in clinical trials. Because of the effect of gender and age on olfactory function (13), each subject was paired with +a sex- and age-matched (from –two to two years) control who denied a history of disabling headache or migraine. For the purposes of this study, controls were required to have a Migraine Disability Scale (MIDAS) score of zero to verify the absence of migraine. Controls included hospital employees, partners of patients in our clinic, and friends or family of employees of our center. We did not specifically exclude people with other pain disorders or a family history of migraine.
During the first visit we administrated a focused questionnaire to all participants to obtain basic demographic and medical history information. We inquired as to whether odors caused them to develop headaches and whether any of five specific odors (perfume, paint, new carpet, gasoline, pesticides) were bothersome. The subjects and the controls completed a validated questionnaire for allodynia (14). The initial recruitment began June 2010 and final kits were received in October 2011.
To determine olfactory function, all subjects completed the University of Pennsylvania Smell Identification Test (UPSIT), a well-validated and standardized 40-item forced choice olfactory test that is useful in detecting subtle olfactory deficits (13,15). This test is more reliable than, yet highly correlated with, traditional olfactory threshold tests (16). There are a total of 40 odorants, with four booklets each containing 10 odorants. Subjects who are literate can perform the test without coaching or the need for administration. The stimuli are embedded in “scratch and sniff” microcapsules at the bottom of each page. The UPSIT score is simply a sum of the correct responses, not a threshold, with a maximum score of 40. This inexpensive test is widely used clinically and has been translated into 14 foreign languages.
All subjects took the UPSIT at the time of their first visit, when the subjects received instructions on how to perform the test at home. After the initial visit, subjects took the UPSIT again at home or in the office during an acute migraine attack (within the first hour) and completed a short clinical survey about their symptoms during the attacks, including severity, location, and aura, if present. We did not specifically ask about osmophobia. If the attack was not typical or especially severe, subjects had the freedom to choose another attack during which to take the UPSIT. They also completed the UPSIT a third time after a typical migraine with successful treatment (either mild or no pain), at least two hours after the attack, allowing for two weeks between attacks (Figure 1.) Based on previous studies using the UPSIT to determine olfaction in various neurodegenerative disorders, and assuming a true difference between the mean UPSIT scores of three units, we determined that with 50 subjects there would be a 93% probability that the study would detect a statistically significant difference at a two-sided 5% significance level. We instructed 25 subjects to take the UPSIT at home during migraine, and to complete the final UPSIT after a treated attack. The other 25 subjects took the UPSIT after a treated attack first, then the final UPSIT during migraine. Controls repeated the UPSIT after the initial visit at least two weeks after the initial visit, and again at least another two weeks later. If subjects or controls completed the UPSIT at home, it was returned to our office in person or by mail.
Study flowchart.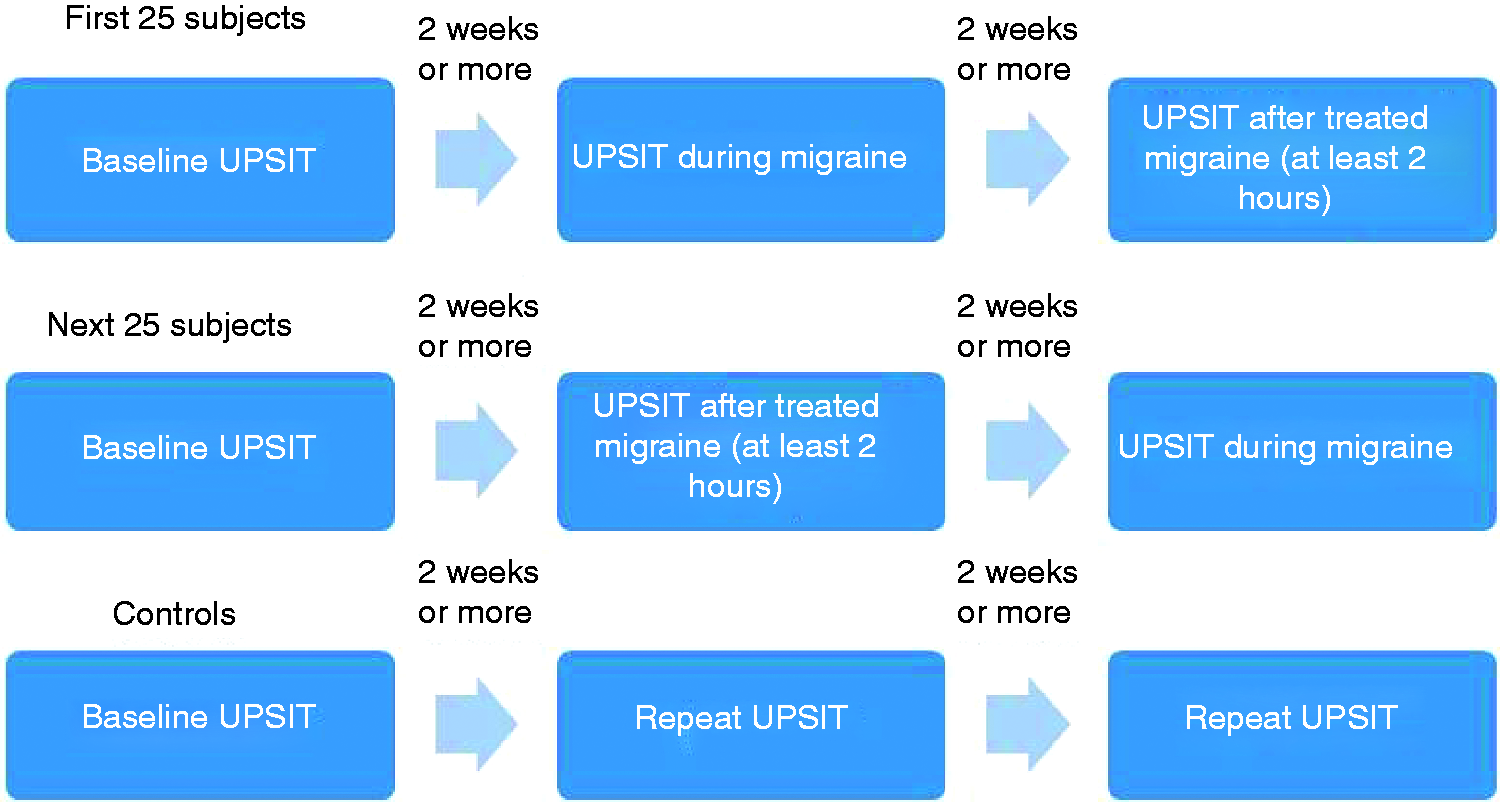
Data from the migraine patients and age- and sex-matched controls were analyzed to determine the association between migraine and olfactory acuity. The baseline characteristics and scores between matched controls and migraine patients were paired and then compared. The paired data were skewed for UPSIT scores and other variables. To address this and test for significant differences between the migraine and control groups while accounting for the correlation within matched pairs, we applied the Wilcoxon Signed-Rank test and Friedman's nonparametric longitudinal test of match-paired differences for continuous variables and McNemar's test of discordant match-paired two-level responses (or the more general Stuart-Maxwell test of discordant match-paired multi-level responses) for categorical variables. For all tests, a significance level of α = 0.05 was used. We accounted for missing data (subjects or controls who didn't return the UPSIT kits) by comparing data with their matched pairs.
Results
Descriptive summary of study group characteristics.

BMI: body mass index (kg/m2); in.: inches; lbs.: pounds.
Descriptive summary of migraine patient characteristics (n = 50).

SD: standard deviation; HA: headache. aMultiple choices are possible so percentages may not add up to 100.
Of those subjects who experience migraines, 32 (65%) indicated that they found odors to be bothersome, while only seven (15%) of the controls did, demonstrating a significant association between group (migraine or control) and sensitivity to odors (Table 1). In terms of the matched pairs, 18 of 45 (40%) had responses that agreed while 27 (60%) had differing responses. Of those 27 responses, 25 (93%) were migraine subjects who found odors bothersome and controls who did not. This discordance strongly indicated a significant association between migraine and sensitivity to odors (p < 0.01).
The two groups had similar olfactory acuity at baseline, but the distribution of the match-paired differences was skewed in the positive direction (Figure 1). At the time of the initial baseline visit, migraine subjects had a median UPSIT score of 36 (between attacks), while the controls had a median score of 37. The median match-paired difference of −1 did not differ significantly from zero (p = 0.18). Forty-two subjects completed the UPSIT during acute migraine and 40 completed the UPSIT after a treated migraine. Of the age-and sex-matched controls, three completed the UPSIT once after the initial visit and the other 47 completed both follow-up tests. The most common reasons given for not completing follow-up tests were lack of migraine headache in the months following the baseline visit or misplacing the UPSIT kits.
Although the majority of migraine subjects had similar scores during migraine as in the initial visit (± 2 points), a minority had clinically significant decreases in acuity, with eight (19%) scoring four or more points worse during acute migraine. Regardless, during their migraine attacks, the median UPSIT score for migraine subjects was still 36 as compared to 36 for controls at their second test; however, the median match-paired difference of −1 was statistically significant (p = 0.02). This suggested that olfactory acuity during migraine was significantly impaired. After being treated, the median UPSIT of the migraineurs was again 36 compared to the median score of 37 among their matched controls at their third test. The median paired difference of −1 was not significantly different from zero (p = 0.15). The histograms in Figure 2 present a visual distributional summary of changes in UPSIT test scores from baseline during attack (panel (a)) and after successful treatment of attack (panel (b)) for the migraine group. Friedman's test did not indicate a significant longitudinal association between the paired differences in scores over the three tests (p = 0.40).
Difference in baseline olfactory acuity (UPSIT scores) between migraine patient and matched control pairs.
Considering a difference of three or more points on the UPSIT to be clinically significant, 13 migraine subjects had a decrease in UPSIT scores between baseline and during attacks of three points or greater, compared with three subjects after a treated attack. One patient had an increase in UPSIT of four points after a treated migraine, and no subject had an increase of greater than three points during migraine. Of the 13 patients with clinically significantly lower scores during migraine, 12 reported allodynia during migraine, eight had migraine with aura, 10 were female, and nine reported a history of migraine greater than 10 years. Of the 23 subjects with no significant olfactory changes during acute migraine, 21/23 reported allodynia, 13/23 reported aura, 18/23 were female, and 17/23 had a migraine history greater than 10 years. There were no significant differences between groups (Table 3 and Figure 3).
Histograms of changes in migraine group UPSIT test scores from baseline during migraine attack (panel (a)) and after attack (panel (b)). Summary of UPSIT scores. UPSIT: University of Pennsylvania Smell Identification Test; Min: minimum; Max: maximum. aWilcoxon Signed‐Rank test of zero median difference (migraine minus control) in match‐paired scores.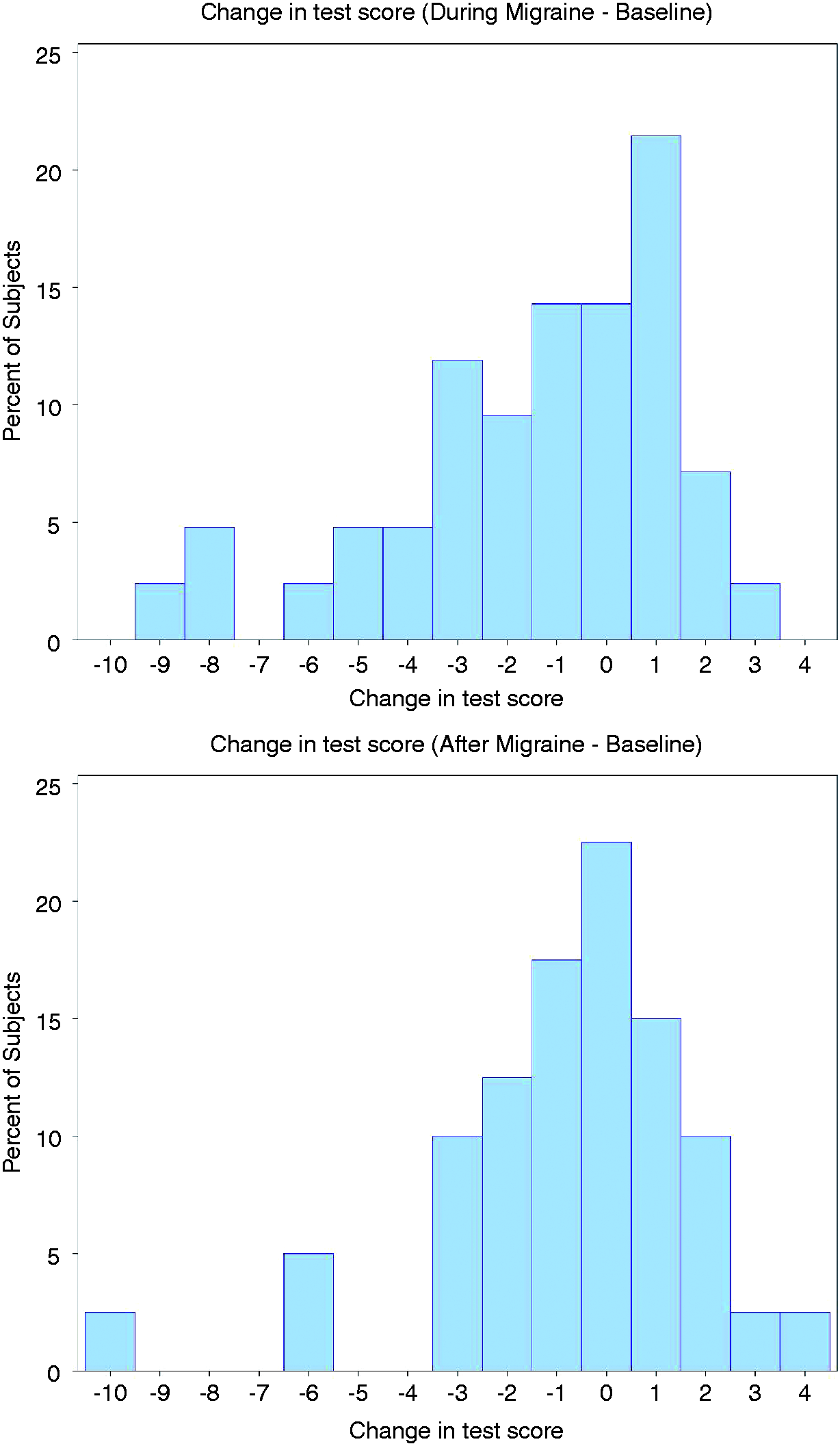

Discussion
The results of this study suggest that the majority of patients with episodic migraine have normal olfactory function. This agrees with the studies of Saisu et al. (5) and Hirsch (11) and supports the idea that migraine differs from neurodegenerative disorders such as Parkinson's disease. However, a subgroup of our migraine subjects appeared to have experienced impairment during acute migraine, especially before successful treatment. This finding is similar to the 1992 study by Hirsch of olfaction in 67 consecutive individuals with migraine. This study, which predated the classification of episodic and chronic migraine, found 18% of migraine subjects were hyposmic or anosmic based on Pyridine odor threshold testing. This study did not specify if subjects were experiencing acute migraine during attacks. The clinical and demographic characteristics of our migraine subjects who had significant olfactory impairment were not significantly different from those who did not in terms of allodynia, duration of disease, sex or presence of aura.
The effect of migraine on olfaction was relatively modest in comparison to the olfactory dysfunction of neurodegenerative disorders (17) and other neurological disorders such as MG (18). In a recent study of MG, 27 MG subjects exhibited a robust loss of olfaction relative to 27 matched controls. It is unclear if the decreased UPSIT scores in our subgroup of migraine subjects have clinical relevance as these differences were relatively small compared to neurogenerative diseases. Our suggestion would be to test olfaction in patients with clinical symptoms of olfactory difficulties, especially those with a history of previous serious viral illness, head trauma or neurodegenerative disease. It should be noted that the subjects in this study were generally fairly healthy with treatable migraine attacks lasting less than 24 hours. In a separate study, we plan to examine subjects with chronic migraine including those without significant headache-free time.
Our results confirmed several previous studies that confirm that people with migraine report experiencing hypersensitivity to bothersome odors. The UPSIT is not a measure of osmophobia, is designed to be well tolerated, and did not trigger migraine attacks in this study. However, no subject in our study exhibited UPSIT scores that would suggest increased olfactory sensitivity during migraine (with an increase of more than three points on UPSIT). Although some people with migraine may be more sensitive to odors even outside of attacks, our findings are in disaccord with those of Snyder and Drummond (12), who found migraineurs to have hyperosmia. However, their test procedures differed from ours. They studied 20 migraine subjects and 21 matched controls with no history of migraine using odor detection thresholds for acetone and vanillin. Interestingly, subjects reporting a perception that odors seemed stronger during migraine had lower threshold for acetone. Acetone is a strong trigeminal stimulant and therefore is not a good measure of olfaction, per se (19). It is unclear whether the presence of osmophobia has any influence on olfactory acuity during migraine.
Our findings are in agreement with the general notion that true hyperosmia is rare, regardless of the diseases involved (20). Taken together, olfactory hypersensitivity (the sense of some patients that olfactory abilities are heightened during migraine) is more likely a perceptual distortion as opposed to one of increased threshold sensory function both interictally and during acute attacks. People with a sense of hyperacute odor detection usually do not have superior olfactory abilities. Pregnancy, for example, is not associated with hyperosmia (21).
A more interesting potential explanation is that migraine affects areas in the brain that cause difficulty in perceiving odors when impaired. Pain-sensitive neurons from the thalamus project widely to multiple cortical regions, including the primary somatosensory cortex, the parietal association cortex, and the primary and secondary visual cortices. This suggests a mechanism for cortical dysfunction in migraine other than cortical spreading depression (22). A recent functional magnetic resonance imaging (fMRI) study found deficient habituation in the trigemino-nociceptive pathway, but not in the olfactory system, suggesting the possibility that a thalamo-cortical network may be an important aspect of migraine as opposed to a single neuronal modulator (23). Migraine is associated with activation of the amygdala and limbic system during acute attacks in a way similar to other pain disorders. The amygdala is highly involved both in odor intensity (24) and odor memory (25). Since activation of the limbic system is a hallmark of pain disorders, it is possible that these changes may not be unique to migraine and olfactory abilities in other people with episodic pain disorders remain unclear. Migraine and its associated pain may affect cognition during attacks, leading to testing errors related to concentration. A minority of individuals with migraine can experience olfactory hallucinations before or during headache, which usually involves a very specific and bothersome odor (26). It is not clear if osmophobia predicts microsmia in individuals with migraine. It is also possible that olfactory dysfunction is these patients is a response to pain, and not specific to migraine. The effect of the acute medications allowed in this study (mostly triptans and nonspecific analgesics) on olfaction cannot be ruled out. Olfactory problems in neurodegenerative diseases involve injury to dopaminergic, cholinergic, serotonergic, and noradrenergic systems, microglial activation, and inflammation (6). Although our subjects generally had normal olfaction at baseline, the development of hyposmia during attacks may indicate abnormal brain functioning, perhaps at the level of the basal ganglia or higher cortical structures (27). Many common migraine premonitory symptoms, such as hunger or yawning, are also thought to be related to dopamine and linked to the hypothalamus (28).
Clinical implications
We found subjects with migraine to have normal olfaction at baseline, similar to age- and sex-matched controls. A minority of migraine subjects in our study had decreased olfactory acuity during migraine, as measured by standardized olfactory testing. After treated attacks, there was a nonsignificant trend toward decreased olfactory abilities compared to baseline and controls. Olfactory dysfunction in migraine could relate to autonomic symptoms, limbic system activation, or disorders of higher-order sensory processing.
Footnotes
Funding
This study was sponsored by the Merck Investigator Initiated Studies Program, ID #36578.
Conflicts of interest
MJ Marmura received clinical research funding support for this project from Merck, has received an honorarium for consultation from Zogenix, and received royalties for publications from MedLink Neurology, Cambridge and Devos Medical.
RL Doty is president and major shareholder of Sensonics Inc, the manufacturer and distributor of olfactory and taste tests, including the odor identification test that was used in this study.
Drs TS Montheith, W Anjum, SE Hegarty and SW Keith have nothing to declare.
Contributions to manuscript
MJ Marmura: drafting/revising the manuscript for content; analysis or interpretation of data; patient recruitment; study concept or design; study supervision or coordination. W Anjum: drafting/revising the manuscript for content; patient recruitment; study supervision or coordination. TM Monteith: drafting/revising the manuscript for content; analysis or interpretation of data; study concept or design. RL Doty: drafting/revising the manuscript for content; analysis or interpretation of data; study concept or design. SE Hegarty, SW Keith: drafting/revising the manuscript for content; analysis or interpretation of data; statistical analysis; study concept or design.
Acknowledgments
The authors thank Kathleen Bradley and Rose Tausendfreundt for their help with patient recruitment and managing this study, and Stephen Silberstein for assisting with study design.