
Abstract
Preliminary studies suggested that headache disorders are more common in patients with joint hypermobility syndrome (JHS). The objectives of this study were to determine if the prevalence, frequency, and disability of migraine differ between female patients with JHS and a control population. Twenty-eight patients with JHS and 232 controls participated in the case-cohort study. Participants underwent a structured verbal interview and were assigned a diagnosis of migraine based on criteria of the International Classification of Headache Disorders, 2nd Edition. The primary outcome measures were the prevalence, frequency, and headache-related disability of migraine. Logistic regression was used for the prevalence analysis and Poisson regression for the frequency and disability analyses. Results indicated that the prevalence of migraine was 75% in JHS patients and 43% in controls. The adjusted odds ratio for the prevalence of migraine was 3.19 (95% CI 1.24, 8.21] in JHS patients. The rate ratios for migraine frequency and headache-related disability were 1.67 (95% CI 1.01, 2.76) and 2.99 (95% CI 1.66, 5.38), respectively, for JHS patients. Our study suggests that JHS is a clinical disorder strongly associated with an increased prevalence, frequency, and disability of migraine in females.
Keywords
Introduction
Joint hypermobility syndrome (JHS) is an inherited connective tissue disorder, which is defined by the presence of joint hypermobility and musculoskeletal symptoms in the absence of systemic rheumatologic disease (1,2). JHS occurs in 10–15% of the general population, often demonstrating an 85–90% female predominance (3–6). An underlying disorder of collagen is thought to contribute to the systemic manifestations of JHS, which can occur at any age and are often progressive (7). Common musculoskeletal symptoms include joint pain, myalgia, joint instability and dislocations, and non-articular limb pain (8). It is becoming increasingly recognized that JHS also involves other body systems outside of the musculoskeletal realm that likely share a common pathophysiology (9). Some of these conditions found to be associated with JHS include orthostatic intolerance/postural orthostatic tachycardia syndrome (POTS), irritable bowel syndrome, fibromyalgia, anxiety/panic disorders, and depression (4,9–11).
JHS is largely caused by an undetermined genetic abnormality likely having multiple genetic aetiologies. It is inherited in an autosomal dominant fashion as a sex-influenced trait (8). Joint hypermobility is assessed clinically using the Beighton scoring system, which is a simple and quick in-office administered test (Figure 1). The diagnosis of JHS incorporates the Beighton score and is determined using the Brighton criteria, which is based on clinical evaluation and history (Table 1). The phenotype of JHS is suggested to represent a clinical continuum with the hypermobility type of the Ehlers–Danlos syndrome (hEDS) because of their indistinguishable clinical features (12). hEDS is the most common form of the Ehlers–Danlos syndromes (EDS), which have an overall prevalence of at least 1 in 5000 (13). The current clinical criteria established to diagnose and distinguish JHS and hEDS are non-specific and not mutually exclusive (12). Thus, the terms JHS and hEDS are often used interchangeably.
The Beighton Scoring System. A quick and easy-to-use scoring system for the presence of generalized joint laxity utilizing a 9-point scale. The examination entails: 1) Passive dorsiflexion of the fifth finger. If the proximal interphalangeal joint can be bent to less than 90° relative to the back of the hand, this is considered positive. 2) Passive apposition of the thumb to the forearm. If the thumb is able to touch the forearm a score of ‘1’ is also assigned for each side. 3) Elbow hyperextension is positive if the elbow can hyperextend greater than 10°. 4) Knee hyperextension is measured in the same manner as the elbow. 5) Forward flexion of the spine is considered positive if the palms can touch the floor with the knees straight. Each of the above tests are performed bilaterally with the exception of forward flexion. A value of ‘1’ is assigned for each positive test and these values are summed to obtain the Beighton score. Generalized joint laxity is diagnosed with a score of ≥5 (out of 9). However, overall joint laxity is influenced by gender, age, training, and racial background. Figure reproduced from Joint Hypermobility Handbook with permission from Left Paw Press. Joint hypermobility syndrome diagnostic criteria The hypermobility syndrome is diagnosed in the presence of two major criteria or one major and two minor or four minor criteria or two minor criteria with an independently diagnosed first-degree relative. Adapted from Grahame et al. (2000) (1).

Several studies suggest that migraine is more common in patients with JHS. Hakim and colleagues (9) found that the prevalence of migraine was 40% in patients with JHS and 20% in a control population. Similarly, Kanjwal and colleagues (11) conducted a study in a clinic for autonomic disorders and demonstrated that migraine occurred in 73% of patients with both JHS and POTS in comparison to 23% of those with POTS but without JHS (P = 0.001). Jacome and colleagues (14) reported that 11 out of 18 patients with a diagnosis of EDS referred to a subspecialty neurology clinic experienced attacks of migraine. These studies, however, represent very preliminary data as the first two studies did not use criteria from the International Classification of Headache Disorders 2nd Edition (ICHD-2) for their diagnoses of migraine and the third was a case series and thus lacked a control group for comparison.
The purpose of this study was to characterize the relationship between primary headache disorders and JHS using validated diagnostic tools in a case-cohort design. The primary objective of this study was to determine if JHS was associated with an increased prevalence, frequency, and disability of migraine as compared to a control population. A secondary objective was to determine if the prevalence and frequency of tension-type headache also differed between these two populations.
Subjects and methods
Subjects
Consecutive patients meeting diagnostic criteria for JHS/hEDS recruited from two separate practice sites of the Connective Tissue Clinic at Cincinnati Children’s Hospital Medical Center between 1 January 2010 and 1 July 2010 were screened for admission into the study as cases. The clinical diagnoses of JHS/hEDS were established by a board-certified clinical geneticist (BTT) based on the established clinical criteria (Table 1). Control patients were selected from two primary care internal medicine practices in the greater Cincinnati area from 1 June 2009 to 30 April 2010. Consecutive cases and controls that met the inclusion and exclusion criteria listed below were asked to participate in this study.
Participants aged 18–65 years who were English speaking and able to provide written informed consent were eligible to participate in the study. Subjects were excluded if they had any of the following conditions: (i) past history of secondary headache disorder due to a brain aneurysm or brain tumour; (ii) specific chronic illnesses such as malignancy, chronic renal failure, tuberculosis, lupus, rheumatoid arthritis, sarcoidosis, hypereosinophilic syndrome, Wegner’s granulomatosis, Churg–Strauss vasculitis, or polyarteritis; or (iii) currently pregnant. These conditions were excluded because these disorders and/or their treatments could potentially modulate the prevalence, frequency, and disability of headache disorders. This study was approved by the Institutional Review Boards of Cincinnati Children’s Hospital Medical Center and the University of Cincinnati.
Headache diagnosis
All participants who reported experiencing a headache in the previous year unrelated to respiratory infection, head trauma, or hangover underwent a structured verbal headache diagnostic interview. The structured interview was designed to capture the clinical characteristics of each headache type and was previously validated to diagnose migraine, tension-type, and other primary headache disorders (15). Interviews were performed by a trained research co-ordinator at the time of an office visit to the practice or by telephone at a later date. If more than one headache type was reported, then only the two headache types with the greatest pain intensity were recorded by the interviewer. The interviewer was aware of the respective clinic setting from which the participant was derived.
After reviewing information gathered during the structured interview, a board certified headache specialist (VTM) assigned headache diagnoses according to the strict criteria of ICHD-2. Migraine was defined as ICHD-2 diagnoses 1.1–1.5 and tension-type headache as 2.1–2.3. To define the frequencies of migraine and tension-type headaches, participants were queried on the number of days per month that they experienced a given headache type. Only headaches meeting diagnostic criteria for either migraine or tension-type headache were assigned a frequency. Since the headache interview was designed to identify up to two different headache types, it was possible that each could be assigned the same diagnosis (e.g. either both migraine or both tension-type). If a participant experienced two headaches of the same type, then the headache with the highest reported frequency was used as the headache frequency for that patient. The headache specialist was also aware of the respective clinic setting from which the participant was derived.
Characterization of cases
All cases underwent additional clinical characterization which was not replicated in the control population. A neurological examination was performed to screen for the presence of secondary headache disorders and a comprehensive medical history and musculoskeletal examination were performed to confirm the diagnosis of JHS.
To screen for the presence of a temporomandibular disorder (TMD), cases were asked the following questions: (i) do you have pain on chewing or upon widely opening the jaw?; (ii) has your jaw ever locked?; and (iii) do you hear noises on opening of the jaw? The presence of probable TMD was defined as a response of ‘yes’ to 2 of the 3 diagnostic questions (16). The presence of TMD was also confirmed by clinical examination.
When available, echocardiograms, cervical spine imaging, and brain MRIs from these cases were obtained by chart review to determine the presence of valvular disease, cervical disc disease, and intracranial lesions, respectively. Valvular disease was defined as mild or greater mitral, aortic, or tricuspid regurgitation or stenosis, or mild or greater mitral valve prolapse. Disc disease was defined as current or past impingement of the nerve or narrowing of the foramen noted on MRI scan.
Cases completed written questionnaires and reported the presence or absence of the following physician-diagnosed co-morbid disorders: fibromyalgia, depression, sleep apnoea, POTS, arthritis, periodic limb movement, and restless leg syndrome.
Written questionnaires
All participants were asked to complete the following validated, self-administered questionnaires: (i) the Patient Health Questionnaire-9 (PHQ-9); (ii) the Generalized Anxiety Disorder-7 (GAD-7); and (iii) the Migraine Disability Assessment (MIDAS; if headache was reported). The PHQ-9 and GAD-7 identify probable cases of depression and generalized anxiety, respectively, and rate their severity; these questionnaires assess multiple domains of functional impairment and rate severity based upon the frequency of disability days due to symptoms in the preceding 2 weeks (17,18). The MIDAS questionnaire assesses headache-related disability; it is designed to evaluate a person’s ability to function in work, home, and social situations and a disability score is determined based upon the number of days in the preceding 3 months that functioning in those areas was reduced by 50% or greater due to headache (19). The headache disability associated with migraine was defined as the mean MIDAS score in patients receiving a diagnosis of migraine. Cases were additionally asked to complete the Neck Disability Index (NDI), which is a clinically-validated tool that rates disability due to neck pain based upon reported difficulty (scale of 0–5) in performing 10 activities of daily living affected by neck pain (20).
Medications
Current medication use was either reported directly by the patient or extracted from the medical chart. Migraine abortives were defined as triptans, ergots, butalbital-containing medications, narcotics, non-steroidal anti-inflammatories, and isometheptane/acetaminophen compounds, and migraine preventatives as β-blockers, calcium channel blockers, antidepressants, anticonvulsants, angiotensin converting enzyme inhibitors, and angiotensin II receptor blockers. Tension preventatives were defined as antidepressant medications.
Statistical analysis
The study sample included 260 females, aged 18–65 years, including 28 JHS cases and 232 non-cases (controls). Males were not included due to the small number of cases (n = 3) which precluded an investigation of the effect modification by gender in the regression analyses. Prior to the regression analyses, differences between JHS cases and controls were tested with respect to percentages of subjects reporting migraine and tension-type headaches, migraine subtypes, and mean values of headache frequencies. Adjusted odds ratios measuring the effect of JHS on migraine and tension-type headache prevalence were obtained by logistic regression. Poisson analyses were performed to obtain adjusted rate ratios of JHS on the frequency of migraine and tension-type headache as well as the headache-related disability of migraine. Age was modelled as a binary variable (<45, ≥45 years) in all regression models (21,22). The cut points of age were determined by Generalized Additive Models (GAMs) of the prevalence of migraine and tension-type headache and were optimum for other models, as determined by model fit. The GAMs showed a non-linear effect of continuous age which was consistent with visual plots, showing that age slopes changed at approximately age 45 years for both headache types (Figure 2). Two separate models were performed for each of the outcome measures to determine if any of the observed associations were accounted for by the presence of co-morbid psychiatric disorders. Model 1 used JHS (yes/no), age (<45, ≥45 years), and preventative medications (yes/no) as co-variates while model 2 included JHS (yes/no), age (<45, ≥45 years), preventative medications (yes/no), and anxiety (yes/no). Co-morbid depression was not included as a co-variate in model 2 because depression and anxiety were highly correlated and it was not statistically significant in any of the models that included both anxiety and depression. Analyses were performed using SAS for Windows v9.3 (SAS Institute, Cary, NC, USA); the R statistical software package was used to produce data plots (R Design Package 2008). A P-value <0.05 determined statistical significance, unless stated otherwise.
Smooth curve of probabilities of migraine headache (A) and tension-type headache (B) versus age in JHS patients (dashed line) and controls (solid line). Note that migraine prevalence tends to peak at 45 years of age and the prevalence of tension-type headache reaches a nadir at 45 years of age.
Results
Demographics
Demographics of study population

P-value obtained using t-test.
P-value corresponding to test the difference in percentage of Caucasian and other races between case and control groups.
GAD-7, Generalized anxiety disorder; PHQ, patient health questionnaire.
GAD-7 is a 7-item questionnaire designed to assess for a generalized anxiety disorder. Multiple domains of functional impairment are rated based upon disability days. Each item is scored 0–3, and on a scale of 21, generalized anxiety is rated as: 0–5, mild; 6–10, moderate; 11–15, moderately severe; and 16–21, severe.
PHQ-9 is a 9-item questionnaire designed to assess for depression. Multiple domains of functional impairment are rated based upon disability days. Each item is scored 0–3, and on a scale of 27, depression is rated: 0–5, mild; 6–10, moderate; 11–15, moderately severe; and 16–27, severe.
Characterization of the JHS patients demonstrated a mean Beighton score of 6.54. All neurological examinations were normal in the JHS group. Furthermore, no intracranial lesions were detected by imaging in the three JHS patients with brain MRIs.
Co-morbid medical disorders were commonly encountered within the JHS patients. Those most frequently encountered included arthritis in 54% (15/28), fibromyalgia in 39% (11/28), and POTS in 18% (5/28), followed by restless leg syndrome (18%, 5/28), sleep apnoea (14%, 4/28), and periodic limb movement (11%, 3/28). A large percentage of cases displayed symptoms of TMD upon screening (74%, 20/27). Echocardiogram reports from 18 cases showed three cases with trivial-to-mild tricuspid regurgitation without other valvular diseases. Cervical disc disease was present in three cases based upon available MRI reports, but neck pain was very common as demonstrated by results of the NDI questionnaire. As indicated by the NDI questionnaire, functional disability due to neck pain in patients with JHS was found to be mild in 22% (6/27), moderate in 59% (16/27), severe in 15% (4/27), and complete in 4% (1/27).
Migraine
Headache characteristics in JHS patients and controls

MIDAS, Migraine disability assessment.
P-values were obtained by Student’s t-tests for continuous variables and chi-squared or Fisher’s Exact tests for categorical variables.
Headache status was available for 28/28 cases and 231/232 controls. The numbers of participants with headache subtypes do not add up to the total number of patients with a given headache type as some individuals may have experienced more than one subtype of headache and because other subtypes are not shown in this table.
Mean headache frequency was defined as days per month with headache and was available for 120/121 participants with migraine and for 121/122 participants with tension-type headache.
This analysis compares the mean MIDAS score (days per 3 months with headache disability) between cases and controls in participants with any type of headache and in those with migraine. MIDAS scores were available for 27/28 cases and 225/232 controls with any type of headache and for 20/21 cases and 99/100 controls with migraine.
Represents the self-reported location of migraine. Migraine location was available for 21/21 cases and 100/100 controls with a diagnosis of migraine.
Represents the total number of cases and controls receiving migraine preventative and abortive medications. Available for 28/28 cases and 232/232 controls.
The adjusted odds ratios (ORs) and rate ratios (RRs) measuring the effect of JHS on migraine prevalence, frequency and headache-related disability

Adjusted OR for age (<45, ≥45 years) and migraine preventative medications (yes, no) in 260 patients in entire population.
Adjusted RR for age (<45, ≥45 years) and migraine preventative medications (yes, no) in 121 patients with migraine. The metric for frequency was days per month and that of disability was days per 3 months.
The presence of anxiety was defined as a GAD-7 score of ≥10, which has a sensitivity and specificity of 89% and 82% for the diagnosis of generalized anxiety disorders (18).
The overall frequency of migraine was 10.5 days per month in the JHS group and 5.6 days per month in the control group (P = 0.01; Table 3). The frequency of migraine was significantly greater in cases after controlling for the influence of age and preventative medication use as the adjusted rate ratio (RR) for migraine frequency was 1.67 (95% CI 1.01, 2.76) in the JHS cases as compared to the controls (Table 4). Headache-related disability, as measured by the MIDAS questionnaire, was greater in migraineurs with JHS than in control migraineurs. The RR for headache-related disability for model 1 was 2.99 (95% CI 1.66, 5.38) for the migraineurs with JHS after controlling for age and preventative medication use. After controlling for anxiety in model 2, the RRs for the JHS group were 1.61 (95% CI 0.97, 2.65) and 2.85 (95% CI 1.55, 527), respectively, for migraine frequency and headache-related disability (Table 4).
Tension-type headache
The adjusted odds ratios (ORs) and rate ratios (RRs) measuring the effect of JHS on the prevalence and frequency of tension-type headaches
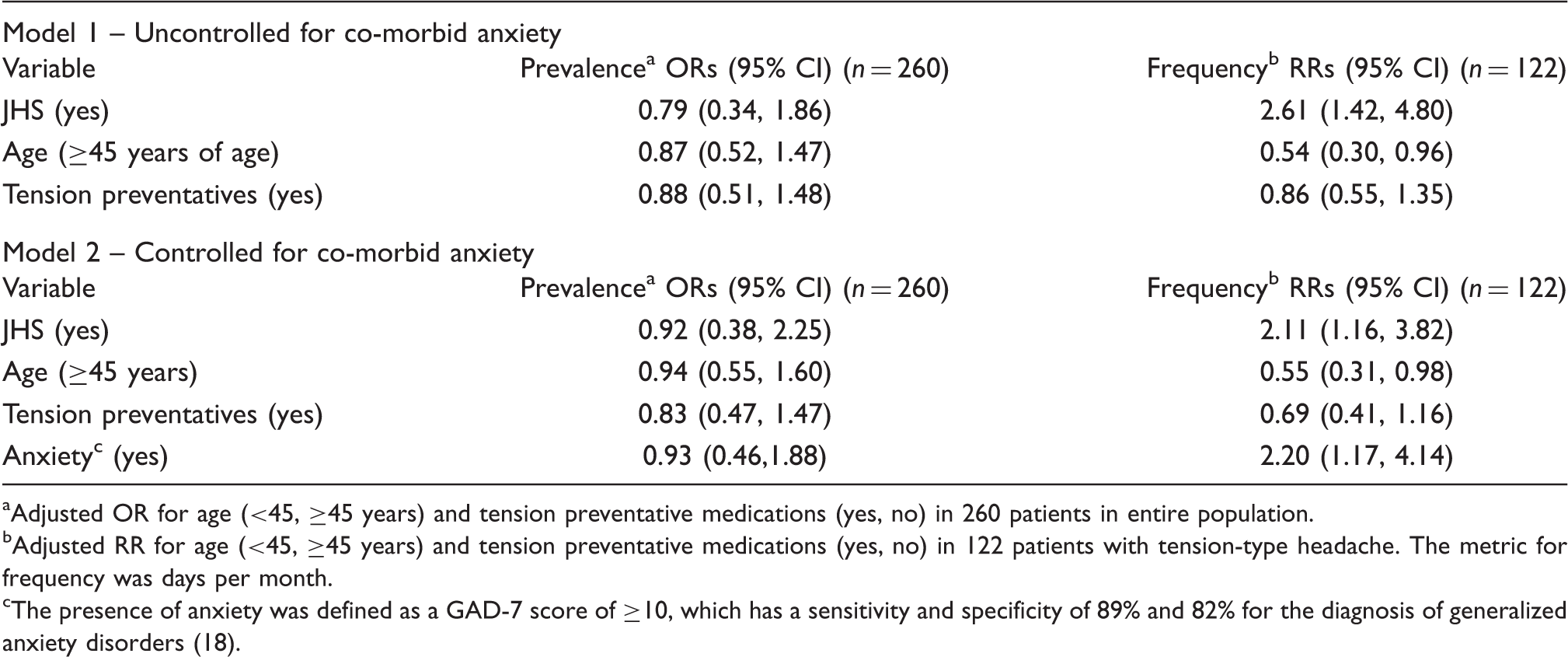
Adjusted OR for age (<45, ≥45 years) and tension preventative medications (yes, no) in 260 patients in entire population.
Adjusted RR for age (<45, ≥45 years) and tension preventative medications (yes, no) in 122 patients with tension-type headache. The metric for frequency was days per month.
The presence of anxiety was defined as a GAD-7 score of ≥10, which has a sensitivity and specificity of 89% and 82% for the diagnosis of generalized anxiety disorders (18).
The overall frequency of tension-type headache was significantly greater for JHS patients (P = 0.02; Table 3). Additionally, the adjusted RR when correcting for age and preventative medication use in model 1 was 2.61 (95% CI 1.42, 4.80). After controlling for anxiety in model 2, the frequency of tension-type headache remained statistically significant with an adjusted RR of 2.11 (95% CI 1.16, 3.82). Anxiety was also significantly associated with the frequency of tension-type headache with an adjusted RR of 2.20 (95% CI 1.17, 4.14; Table 5).
Discussion
The main finding of our study was that the prevalence of migraine was more than three times greater in female subjects with JHS than that observed in a control patient population. Tension-type headache, on the contrary, showed no increased prevalence in cases compared to controls. These results suggest that the association between JHS and the prevalence of headache disorders is specific for migraine.
JHS/hEDS, although a dominant genetic condition, shows remarkable sex-influence. Past studies have demonstrated that 85–90% of patients with JHS are women (3,5). Of the original 31 patients recruited into our study, 28 (90%) were female; therefore, the female predominance noted in this study is similar to population-based studies from the literature. This over-representation of females in JHS is thought to be due to hormonal influences on ligamentous laxity (23).
Age was found to be a predictor of prevalence in control patients with both migraine and tension-type headache. The limited number of JHS patients in our study precludes discussion of this association in that population. In controls, migraine prevalence was found to be lowest at younger ages, increasing until age 45 years where the prevalence peaked, and then decreasing again until it is lowest at older ages (Figure 2A). Conversely, the prevalence of tension-type headache was found to be greatest at younger ages, gradually decreasing until age 45 years, at which point the trend changed to increasing again in older ages (Figure 2B). Such an inverse relationship between migraines and tension-type headaches could suggest that headaches begin as tension-type headaches in women at younger ages, evolve into migraines during reproductive years, and then transition back to tension-type headaches in older age groups. An increase in the prevalence of migraine during reproductive years could occur as a result of fluctuating ovarian hormones encountered during the female reproductive cycle. Obviously, this hypothesis is interesting and will need to be confirmed in future studies.
Headache frequency and disability
The frequency and disability of migraine as well as the frequency of tension-type headache were also modulated by the presence of JHS. Female migraineurs with JHS experienced 1.7 times more days with migraine and 3 times more days with headache-related disability than the control group. Additionally, the frequency of tension-type headaches was 2.1 times greater in those with JHS than in controls. These data indicate that the effect of JHS on the frequency of headache is not specific for migraine headache, increasing this outcome measure in both headache types. It is conceivable that the co-morbid medical conditions and/or their treatments could increase the frequency of both primary headache types (see below).
Theories of migraine pathogenesis
Our findings suggest that connective tissue disorders could play a role in modulating the prevalence of migraine. Although headache pathogenesis in JHS remains uncertain, several mechanisms could explain why migraine is more common in female patients with JHS.
The underlying change in connective tissue in JHS could lead to abnormal vascular reactivity that could predispose to the development of migraine. Yazici and colleagues (24) found aortic stiffness to be lower and aortic distensibility to be higher with Doppler ultrasound in patients with mitral valve prolapse (MVP) and JHS as compared with those with MVP alone. Past studies have also reported that arteriopathies such as cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL) as well as carotid artery dissection are associated with attacks of migraine with aura (25,26). Interestingly, migraine with aura was over-represented in our patients with JHS as 43% (9/21 patients) of the migraineurs with JHS were diagnosed with typical aura with migraine as opposed to 24% (24/100 patients) within the control population. Therefore, JHS could represent a type of arteriopathy associated with an increased frequency of attacks of migraine with aura.
JHS could also be associated with a dysautonomia leading to migraine as postural orthostatic tachycardia syndrome (POTS) disease is associated with JHS. Gazit and colleagues (27) reported that orthostatic hypotension, POTS, and orthostatic intolerance occurred in 78% of patients with JHS as compared with 10% of controls. Autonomic testing revealed evidence of α- and β-adrenergic hyperactivity in patients with JHS. It has been postulated that the distensible vessels encountered in JHS may result in increased venous pooling, which then may cause a compensatory hyperadrenergic state (28). Other studies have shown an increased prevalence of migraine in those with POTS. Khurana and Eisenburg (29) found that 23 of 24 patients (96%) with POTS had a diagnosis of migraine or probable migraine. Kanjwal and colleagues (11) demonstrated that migraine occurred in 73% of patients with both JHS and POTS as compared to 23% of those with POTS but without JHS (P = 0.001). In our study, POTS was self-reported by 18% of JHS patients, which is likely an under-representation of this disorder since autonomic testing was not performed in all of our patients. Thus, the presence of POTS as part of JHS may account for the increased prevalence of migraine.
Co-morbid medical disorders
The co-morbid medical disorders that are associated with JHS are varied and include TMD, cervical disc disease, fibromyalgia, sleep disorders, and anxiety. These disorders could produce their own separate headache disorder or modulate existing primary headache disorders.
TMD is a common disorder found within patients with JHS. DeCoster and colleagues (30) reported that 71% of patients with JHS experienced symptoms of TMD, which is similar to the 74% prevalence seen in our study. The presence of TMD could produce head pain referred to the temporal regions of the head. In our study, migraine headaches were most likely to be located in the temporal region in JHS patients with 62% of patients reporting migraine in that region. This could suggest that the presence of TMD modulates the location of migraine. It is also possible that the presence of TMD could affect the frequency and disability of primary headache disorders.
Neck pain and cervical disc disorders are frequently encountered within JHS patients. Cervical disc disease was noted in 11% of our JHS patients, but neck pain was far more common as evidenced by the fact that 78% of JHS patients (21/27) experienced moderate or greater disability noted on the NDI. Neck pain can occur as a result of cervical disc disease, myofascial trigger points, or cervical spine hypermobility. Rozen and colleagues (31) postulated that cervical hypermobility was a predisposing factor for the development of new daily persistent headache in patients with JHS. Convergence of cervical nerves within the spinal trigeminal nucleus could provide a theoretical basis for a worsening of existing headache disorders in those with cervical spine pathology.
Wide-spread chronic pain, inherent to fibromyalgia and often present in JHS, may also contribute to the intensification of headache. Ofluoglu and colleagues (10) reported that 64% of patients with fibromyalgia had joint hypermobility as compared to 22% of a control population. Our cases self-reported a diagnosis of fibromyalgia in 39%. Studies have suggested up to 50% of individuals with fibromyalgia have enhanced pain perception (32). This enhanced pain perception may result from central sensitization of pain networks (33). Altered modulation of pain in patients with fibromyalgia may lower the threshold for both migraine and tension-type headache.
Sleep disorders appear to be common in patients with JHS. Sleep disturbances occur within 37% of children with JHS while periodic limb movements are found in 67% of adults with EDS (34,35). Conversely, sleep disturbances including sleep apnoea, restless leg syndrome, and snoring frequently co-occur in patients with migraine and other headache disorders (36,37). It is quite possible that alterations in sleep patterns could cause headaches to be more frequent or severe.
The prevalence of anxiety is increased in patients with JHS. Hakim and colleagues (9) reported that anxiety occurred in 32% of JHS patients as compared to 12% within a control population. We did perform separate analyses controlling for co-morbid anxiety to determine if our results might be explained by the presence of this disorder. The ORs and RRs were minimally changed by the inclusion of anxiety in these models with the exception of the migraine frequency outcome measure, which just missed significance after controlling for this co-variate. Interestingly, anxiety was found to be strongly associated with migraine prevalence (OR of 3.72) as well as the frequency of tension-type headache (RR of 2.20). This suggests that the presence of anxiety has little impact on the associations observed between JHS and migraine, but that it may have its own independent effect on migraine prevalence and the frequency of tension-type headache. We were unable to control for the other co-morbid disorders noted within the JHS population as these data were not collected within the control population. Thus, it is unknown whether the associations between JHS and migraine would remain if all of the co-morbid medical disorders had been controlled for within the analyses. This would require a much larger study population to answer such a question.
Other headache disorders
JHS may predispose to other secondary headache disorders such as Chiari malformation, intracranial hypotension, and carotid/vertebral dissections. Each of these disorders has been associated with EDS and other collagen-related disorders (38–40). We did not perform diagnostic testing to exclude these disorders in all of our patients with JHS, as there were no clinical findings to suspect these disorders.
Strengths and limitations
Our study has some important strengths compared to past studies. First, our cases with JHS/hEDS were well-characterized by a geneticist with special expertise in the diagnosis and management of these disorders. Second, this is the first study to confirm an association between JHS and migraine adhering to the ICHD-2 diagnostic criteria and to compare these patients to a control group within primary care. Third, we used a validated verbal interview that enabled us to accurately collect the characteristics of each headache type. Fourth, this is the only study of JHS patients to use the frequency and disability of migraine headache as outcome measures.
Interpretation of our results is not without limitations. First, our cases were enrolled from a subspecialty genetics clinic and we cannot exclude the possibility of selection bias in our JHS group (e.g. patients in a subspecialty clinic have more co-morbid medical illnesses than those within a primary care population). We believe that our choice of internal medicine patients as controls might have minimized differences between these groups as internists typically care for patients with multiple co-morbidities. Second, we did not exclude patients with JHS from our control population. However, even with this limitation, our conclusions would not be significantly changed as this likely would have artificially inflated the migraine prevalence in the control group, which would only serve to lessen the association between JHS and migraine. Third, the frequency of analgesic use was not ascertained in this study; therefore, we cannot exclude the possibility that medication overuse might have contributed to an increased frequency and disability of headaches within JHS patients. Fourth, we cannot exclude the possibility that some of our diagnoses of tension-type headache might have also met criteria for probable migraine. Current ICHD-2 criteria require a diagnosis of probable migraine to ‘not be attributed to another disorder’. If headaches met criteria for both tension-type headache and probable migraine, then the tension-type headache diagnosis would over-ride the probable migraine diagnosis. Fifth, some of the co-morbid medical disorders (e.g. POTS, fibromyalgia, sleep apnoea, restless leg syndrome, and periodic limb movement) were self-reported by the JHS patients and could be subject to error. Sixth, the frequency of a given headache type was self-reported by the patient during the verbal diagnostic interview and not obtained by daily diary studies, which may have led to error and recall bias for this outcome measure. However, we believe that this is a valid technique for assessing headache frequency as a recent study found a high correlation between self-reported headache frequencies and daily diary data (41).
Conclusions
Our study indicates that the prevalence of migraine approaches 75% in female patients with JHS and is 3 times greater in these patients than controls. The prevalence of tension-type headache was not increased, suggesting that the association between JHS and headache disorders is specific to migraine. The frequency and disability of migraine were also significantly increased in JHS patients. The increased risk of migraine in our JHS population supports the hypothesis of a common pathophysiology in these conditions. These preliminary findings will need to be replicated in population-based studies before firm associations can be established between migraine and JHS.
Footnotes
Notes
Acknowledgement
This study was funded, in part, by a grant from GlaxoSmithKline (grant number 109473).