
Abstract
The prevalence of migraine and tension-type headache (TTH) varies considerably with respect to gender, age group and geographic regions. Methodological differences in the assessment and classification of cases are a major cause of this variability across studies, limiting the ability to perform true regional comparisons. We conducted three population-based studies in different German regions and assessed headache prevalence and headache characteristics in face-to-face interviews, applying standardized methods. We analysed the 6-month prevalence of migraine, TTH and their probable subtypes based on the new criteria of the International Headache Society (IHS). Among the 7417 participants in all three regions, the pooled 6-month prevalence of migraine, probable migraine, TTH and probable TTH was 6.75, 4.40, 19.86 and 11.61%, respectively. Despite the application of standardized classification methods, regional variations between 4.39 and 8.00% for migraine and 15.44 and 23.64% for TTH were observed, indicating differences in the local headache burden. Application of the new IHS criteria yielded headache categories that were not mutually exclusive, indicating a need for further discussion about the value of probable headache types in epidemiological studies.
Introduction
The number of published studies assessing the prevalence of headache or of major headache types such as migraine or tension-type headache (TTH) is large. The observed prevalences vary between genders, age groups, but also considerably between different geographical regions. Results have been summarized in several reviews (1–3), which also suggest that the application of different methods in the classification of cases and changing time frames in their assessment contribute to variations in the observed prevalences across studies. Variations between regions within one country or between countries in one region, however, have rarely been studied. In 2004 the International Headache Society (IHS) published the second edition of the ‘criteria for the classification of headache types’ (4). Among other changes, the introduction of ‘probable headache types’, e.g. for migraine and TTH, was important. Since the vast majority of prevalence reports were published before 2004, headache prevalences based on the new criteria are scarce.
In Germany only a few studies have investigated the frequency and impact of different headache types on an affected individual (5–9). The considerable inconsistencies in their results were probably due to differences in the applied study methods, e.g. the selection of participants or the method to classify cases. Four of these studies have collected data on the lifetime prevalence (5–7, 9), and two on the 7-day prevalence (7, 8). Even in studies with the same time frame, the ascertained prevalence varied considerably. Only one study has investigated prevalences with different time frames (7).
Although the most recent National Health Survey (8) collected data on the prevalence of various pain locations, it allowed neither a classification of headache subtypes nor an analysis of regional variability in different German regions. However, recent reports have shown that for various other illnesses, considerable East-West and/or other regional variations can be observed in Germany, e.g. for hypertension (10), stroke (11), cancer (12) and ischaemic heart disease mortality (13). Regional variations in prevalences result in differences in the respective local burden of disease, e.g. the absolute number of affected individuals, their consumption of medication, days of work absenteeism or the number of specialists necessary to treat them, to name a few.
Due to this lack of data, the German Migraine and Headache Society (DMKG) initiated a project to collect data in three different regions in Germany on the frequency of migraine and TTH. Integrated in the project was a headache survey in children and adolescents conducted in one of the three regions, which has been published separately (14). The overall aim of the German DMKG Headache Study was to determine the prevalence of migraine and TTH, including their subtypes, using the new IHS classification in three German regions and to describe variations across these regions.
Methods
Data collection in all regions took place between 2002 and 2006. Planned follow-up assessments in two existing large population studies, the Study of Health in Pomerania (SHIP) in the northeast and the Monitoring Trends and Determinants in Cardiovascular Disease (MONICA) Project Augsburg in the south of Germany, were combined with a new survey in the city of Dortmund in the west of the country. Participants in all three studies were drawn randomly from the local or regional registration offices, stratified by gender and age, resulting in equal numbers of persons across all gender-age strata present in each respective study. This adjusted for slight differences in the age structures between the three regions. The study design allowed comparing frequencies of different types of headache across three German regions and enabled East-South, South-West and East-West comparisons.
In the western region a total sample of 3820 persons aged 25–75 years was randomly selected from the Dortmund city registration office (from a total population of 591 000) and contacted by mail. Of these, 395 were not eligible, because they had moved out of the study area, died, or lacked sufficient knowledge of the German language to understand informed consent. Thus, 3425 individuals were invited to participate. If personal participation in the central study centre was not possible, a questionnaire with a shortened but otherwise identical set of questions was sent to the respective participant. In case of no response, two additional invitation letters were sent out. Subsequently, up to five attempts were made to contact an individual by phone in case of persisting non-response. Finally, all remaining addresses were again checked for movements out of the study region and home visits done to the remaining addresses. The overall response was 66.9%, yielding 2291 participants. Although headache prevalence was assessed in all participants, the classification of headache subtypes was done only in those who participated in the personal interview in the study centre (n = 1312), due to space restrictions in the mailed questionnaire.
The adult survey in the northeastern region encompassed the area of the SHIP study (15), which was started by the University of Greifswald in 1997. The baseline survey of the SHIP study included 4310 participants aged 20–79 years. Baseline response was 68.8%. The headache question module was implemented in the first follow-up of the SHIP study, which was conducted after a mean follow-up of 5 years. Follow-up response was 83.6%, yielding 3300 participants aged 25–88 years. The third study was conducted within the framework of the ongoing Cooperative Health Research in the Augsburg Region (KORA) project (16) and included the participants of the KORA-F3 study. KORA is a research platform that succeeded the former World Health Organization MONICA Augsburg project (17) in southern Germany and comprises a study area of about 600 000 inhabitants. The headache module was implemented in the 10-year follow-up (KORA-F3) of the survey, whose baseline assessment took place in 1994/1995. Participants had been randomly sampled from the city registries of Augsburg and 16 adjacent communities, stratified by age and sex. This baseline survey had a response of 73.1% and included 4856 individuals aged 25–74 years. Follow-up response among those still eligible was 76.0% and yielded 2805 individuals in age groups 35–75 years in which headache was assessed.
In all three study regions participants were interviewed face-to-face by trained interviewers who were supervised for interview quality. The standardized interview included questions on sociodemographic data, the utilization of healthcare services, the type and frequency of headache symptoms, and medication intake in the last 7 days. In addition, the frequency of cardiovascular risk factors and disorders as well as other comorbidities was recorded. The standardized headache question module used in all interviews was designed to assess the new classification (i.e. 2nd edition) of the IHS (4). It particularly differentiated between the newly introduced term ‘probable’ migraine (IHS code 1.6), ‘chronic’ migraine (IHS code 1.5) and ‘probable’ TTH (IHS code 2.4). Its basic form was used in all three regions and included 21 questions on headache characteristics and symptom frequency. This basic form allowed the classification of the 6-month prevalence of headache in general as well as of migraine and TTH including their ‘probable’ forms. In the Dortmund survey this basic form was supplemented with additional questions allowing the differentiation between migraine with and without aura, the assessment of menstrual migraine, medication overuse headache and family history of migraine and the additional assessment of 12-month prevalences. The extended headache module was assessed twice in that study, in case the assessment of an additional (second) headache type was necessary. Application of the extended headache module in the Dortmund study was restricted to those with personal interviews in the study centre.
Written informed consent was obtained from the participants in all three study regions, and the study protocol was approved by the local ethics committee of the medical faculty at the University of Münster.
Statistical analysis
Our analyses were restricted to a report of prevalences, pooled ones as well as stratified by gender and region. Pooled prevalences were directly age standardized to the German population aged 25–84 in 2006. All analyses were done with STATA 9.0 (StataCorp LP, College Station, TX, USA).
Results
A total of 7417 adults participated in the interviews of the German DMKG Headache Study, 2805 in the region of Augsburg, 1312 in Dortmund and 3300 in Pomerania. Table 1 summarizes the characteristics of the study participants in the three regions. Slight differences existed in the age ranges of the recruited participants in each region due to different lower or upper age inclusion criteria. Therefore, characteristics are shown for the age group 35–75 years in all three regions and, additionally, for all included age groups in the studies in Dortmund and Pomerania. The lower percentage of individuals with a school education of < 10 years in SHIP is due to the school system in former East Germany, where a 10-year basic school education was available for most of the population. Prevalences of cardiovascular comorbidities vary slightly between the studies, supporting evidence of regional variability in these diseases.
Characteristics of the regional study populations for the age group 35–75 years and according to all regional age groups

*Age group 35–75 years.
†Age group 25–75 years in the Dortmund Health Study.
‡Age group 25–88 years in the Study of Health in Pomerania SHIP.
§Self-reported doctor diagnosis.
The pooled, overall 6-month headache prevalence in the study was 49.49% and varied between 45.52% in the northeastern and 54.55% in the southern region. Table 2 shows the pooled 6-month prevalence of each headache type, standardized to the German population aged 25–84 years. TTH and probable TTH (19.86 and 11.61%, respectively) were about three times more prevalent than migraine and probable migraine (6.75 and 4.40%, respectively). Interestingly, the prevalence of both probable headache types was about 40% lower than the related ones with complete criteria. The prevalence of all chronic forms was < 1% and very similar for the complete and probable headache types. The age-standardized prevalences allow the calculation of the absolute number of affected individuals in the German population within the age range 25–84 years (in 2006 n = 59 591 370). A migraine prevalence of 6.75% translates into 4.02 million affected individuals with migraine, with 131 000 having a chronic course. A TTH prevalence of 19.86% results in an absolute number of 11.83 million individuals in this age range in the preceding 6-month period in Germany.
Pooled 6-month prevalence* of migraine, tension-type headache (TTH) and their probable forms and subtypes, according to the IHS criteria, 2nd edn

*Standardized to the German population aged 25–84 years in 2006 (direct age standardization).
†Migraine with completely fulfilled criteria according to IHS classification 2nd edn.
‡Migraine and probable migraine course: episodic < 15 days/month; chronic ≥ 15 days/month; undetermined missing frequency information or not classifiable.
§Probable migraine according to IHS criteria classification 2nd edn.
¶TTH, tension-type headache according to IHS classification 2nd edn.
**Tension-type headache and probable tension-type headache course: infrequent episodic < 1 day/month; frequent episodic 1–14 days/month; chronic ≥ 15 days/month; undetermined missing frequency information or not classifiable.
††Probable TTH, probable tension-type headache according to IHS classification 2nd edn.
Tables 3–5 list the overall and gender-specific 6-month prevalence of migraine and TTH, including their subtypes, in each region. In each of these tables the prevalence is shown for the age group 35–75 years and, additionally, for all included age groups in the two studies in Dortmund and Pomerania. Table 3 shows that the overall prevalence of migraine is considerably lower in East Germany compared with the southern and western region, whereas the frequency of chronic migraine is very similar. In contrast, the prevalence of probable migraine, according to the new IHS criteria, was clearly higher in East Germany and low in Southern Germany. The lower prevalence of migraine with complete criteria and the higher prevalence of probable migraine in East Germany are present in women as well as in men.
Regional standardized 6-month prevalence (%) of migraine, probable migraine and their courses for women and men in age group 35–75 years and according to all regional age groups, based on the IHS criteria 2nd edn
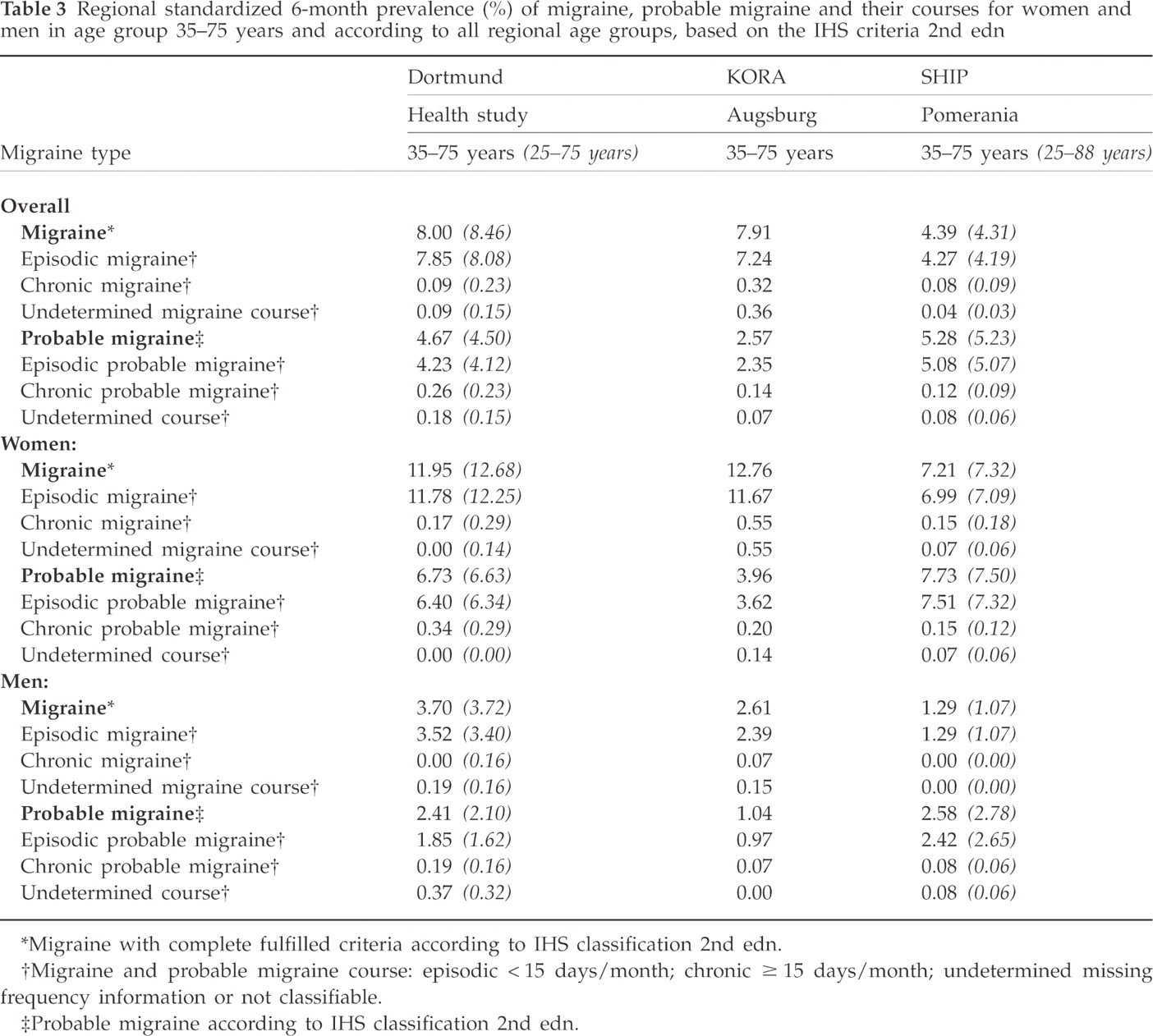
*Migraine with complete fulfilled criteria according to IHS classification 2nd edn.
†Migraine and probable migraine course: episodic < 15 days/month; chronic ≥ 15 days/month; undetermined missing frequency information or not classifiable.
‡Probable migraine according to IHS classification 2nd edn.
Table 4 describes the overall prevalence of TTH with complete criteria and the frequency of its four courses. The highest overall prevalence of this type of headache was observed in the southern region. In all three regions the subtype of frequent episodic TTH was the most prevalent one, contributing 56–79% to the overall TTH prevalence in each region. The prevalence of chronic TTH was ≤ 1% in all studies. TTH prevalence was similar in women and men in the southern and western regions, whereas in East Germany the prevalences in men were lower for all TTH subtypes. In Table 5 the prevalence of probable TTH is shown. This type of headache was less frequent in Dortmund than in the other two regions, especially in women. Within all individuals with this headache type the proportion of those with probable frequent episodic TTH was clearly lower in all three studies compared with the findings for TTH with complete criteria. Probable frequent episodic TTH contributed between 39 and 67% to the overall prevalence of probable TTH. Prevalences in Dortmund were very similar in both genders, whereas in Augsburg and East Germany overall prevalence and that for a frequent course were lower in men than in women.
Regional standardized 6-month prevalence (%) of tension-type headache (TTH) and its courses for women and men in age group 35–75 years and according to all regional age groups, based on the IHS criteria 2nd edn

*TTH, tension-type headache according to IHS classification 2nd edn.
†Tension-type headache course: infrequent episodic < 1 day/month; frequent episodic 1–14 days/month; chronic ≥ 15 days/month; undetermined missing frequency information or not classifiable.
Regional standardized 6-month prevalence (%) of probable tension-type headache (TTH) and its courses for women and men, according to the new IHS criteria

*Probable tension-type headache according to IHS classification 2nd edn.
†Probable tension-type headache course: infrequent episodic < 1 day/month; frequent episodic 1–14 days/month; chronic ≥ 15 days/month; undetermined missing frequency information or not classifiable.
We also analysed causes that contributed to a case classification as a probable headache type instead of the respective one with completely fulfilled criteria. Table 6 reports these results. It can be seen that in probable migraine cases non-fulfilment of criterion B (untreated attack duration 4–72 h) is the most important single reason why an individual was classified as a probable and not a complete migraine case. For TTH, criterion B was also the most important single cause for non-fulfilment of all criteria. However, criterion A (number of attacks) and D (accompanying symptoms) also contributed considerably to a probable TTH case classification. Restriction of the analyses to the age groups 35–75 years did not change these results in the Dortmund and Pomeranian studies.
Percentage of cases with probable headache types not fulfilling each of the four criteria for a complete migraine or tension-type headache (TTH) classification, according to study region

Criterion A, attack number (at least 5 migraine or 10 TTH attacks); criterion B, attack duration migraine 4–72 h or TTH 30 min to 7 days (untreated or unsuccessfully treated); criterion C, headache characteristics (≥ 2 out of 4); criterion D, accompanying symptoms.
The extended headache module used in the Dortmund region allowed a detailed ascertainment of additional migraine subtypes, e.g. migraine with and without aura, menstrual migraine, and of changes in the prevalence of migraine and TTH due to presence of an additional second type of headache (data not shown). The total 6-month prevalence of migraine with aura in Dortmund was 1.6% and clearly higher in women than men. Thus, in both genders migraine without aura was about four times more prevalent than with aura (women 2.3% vs. 10.4%; men 0.8% vs. 2.9%). Sixteen of the 88 women who met the complete migraine criteria in this region reported regular migraine attacks related to their menstruation [i.e. fulfilling the criteria for pure menstrual migraine or for menstrually related migraine (IHS A1.1.1 or A1.1.2)]. Another 33 women indicated that they occasionally had migraine associated with their menstrual period. Thus, the total prevalence of migraine attacks regularly related to menstruation was 2.3% among all women, 4.0% among all women with headaches during the preceding 6-month time span and 18% among all female participants with migraine. One hundred and eighty individuals (13.7%) reported two or more types of headaches, amounting to 28.2% of all participants with headache in the last 6 months. A total of 118 participants (9.0%) had two different types of headache, 60 (4.6%) indicated more than two types, and for two persons information on number was missing. Taking a second headache type into account influenced the prevalence of migraine and TTH differentially. Only one participant whose symptoms fulfilled complete migraine criteria reported these as the second type of headache. Thus, the migraine prevalence in the Dortmund Health Study changed only minimally by 0.1% if a second headache type was assessed. For TTH, however, another 70 individuals indicated it as their second headache type. Of these, 38 had reported this type of headache already as their first headache, leaving 32 individuals affected with TTH as the second headache type. This group increased the total prevalence of TTH by 2.4%, from 17.5 to 19.9%, or, relatively expressed, by 13.7% if more than one type of headache was included. These results indicate that the frequency of TTH, but not that of migraine, is underestimated if only one type of headache is assessed. A change in time frame of assessment from 6- to 12-month prevalence in the Dortmund Health Study did not materially change the reported prevalence [12-month prevalence based on the age range 25–75 years: (i) complete criteria: migraine 8.7%, TTH 18.7%; (ii) probable criteria: migraine 4.9%, TTH 11.1%].
Discussion
We assessed the prevalence of migraine and TTH, their probable subtypes and courses applying the new classification of the IHS in three large population-based studies in Germany. Standardized methods were used to ascertain and classify headache cases, and we were able to describe regional variations in the observed prevalences. Differences were found between the studies, with the highest migraine prevalence in the urban western region and the lowest in the more rural northeastern part of Germany. The TTH prevalence in east and west was similar and considerably lower than in the southern region. These regional variations were observed in both men and women. Our results indicate that headache frequency is variable even within a country such as Germany. The newly introduced categories of ‘probable headache types’ increase even further this variation of headache types in population-based studies. Our analysis has revealed that the item ‘duration of symptoms’ is the single most important one for the differentiation between migraine or TTH with complete criteria and their probable subtypes. Our results indicate the need for further discussion about the necessity and value of the newly introduced probable headache categories in epidemiological studies.
Although the significance of epidemiological studies is often emphasized as a method for quantifying the frequency and burden of headache, only few such data are available for Germany. In a study by Göbel et al. (5), 11.3% of study participants fulfilled the complete criteria of migraine and 13.3% the complete criteria for TTH. However, in that study the proportion of subjects fulfilling all but one criterion was even higher (16.2% for migraine and 25.0% for TTH). Significant correlations were found between the various headache types and sociodemographic variables. It must be noted, however, that the participants were drawn from a market research panel. It is highly doubtful that such a panel is comparable to the general population with regards to frequency and type of illness. Another study using market research methods has examined the prevalence of migraine in former West Germany (6). The authors classified headaches in accordance with the first edition of the IHS criteria. The 12-month prevalence of migraine in women was 5.3% and in men 1.7%. The large difference in migraine prevalence between these two studies illustrates the need to apply standardized methods of participant selection and case classification.
Compared with the first and with international studies, the prevalences observed in our three study regions are rather low (2, 3). In contrast to ours, most other studies either reported 12-month or life-time prevalence. The latter time frame, especially, can contribute to higher percentages. Our additional analysis of 12-month prevalences in the western region, however, revealed only very small changes in the observed prevalences if the time frame of assessment was increased from 6 to 12 months. Another reason for lower prevalences might be the method of collecting headache characteristics in each participant. We used face-to-face interviews in all three study regions, whereas many other published studies were questionnaire based. In the latter approach no clarifications can be provided in case of misunderstanding of a single question. In this situation clarifications provided by an interviewer might yield more correct answers, resulting in lower prevalences.
The IHS classification is meant for clinical applications. The objective inherent in the clinical situation is to record all types of headache, i.e. even several in one person (18). In epidemiological studies this is possible only to a limited extent (19). When classifying a first or additional headache type, the IHS classification assumes that such a grouping is clearly based on all available information, e.g. patient history, physical examination, and, occasionally, results of diagnostic work-up. Large population-based studies, in contrast, cannot apply this strategy. Their resources are usually limited to a questionnaire or a face-to-face or telephone interview.
The major problem of the new IHS classification in this situation is that the probable headache types are not mutually exclusive. A certain percentage of individuals among the participants who completely fulfil the criteria for migraine will do so for the criteria of ‘probable TTH’. Conversely, there can also be individuals among the participants who completely fulfil the criteria for TTH (IHS Code 2.1–2.3) and those for ‘probable migraine’ (IHS Code 1.6). Although prioritizing the complete headache types would offer a solution in these cases, this is not possible for the considerable group of individuals (4.75% of all participants in our study) who fulfil the criteria of ‘probable migraine’ and of ‘probable TTH’. At this point, the IHS classification requires further information for a final diagnosis, which for the above-mentioned reasons is not possible in an epidemiological study. Until now, the only solution has been to create extra categories of ‘double probable’ cases and of ‘unclassifiable’ headache cases. Further clarification of this situation is needed.
Our study has strengths and limitations. We were able to address several of the methodological aspects relevant to the application of the IHS criteria. We used a standardized case classification and face-to-face interviews for all participants. All three study populations were initially randomly drawn from regional or community registries. The inclusion of three different regions allowed analysis of large samples and subsequently rare types of migraine and TTH, and we were able to apply the new IHS criteria for headache classification. The regions included in the study, however, were not drawn at random from all of Germany. Instead, we made use of ongoing population studies in two regions (south and northeast) and selected a third one in the west for comparison. None of the three regions is representative of the total German adult population. Other study designs and sampling methods must be used to achieve this goal, and we did not aim at this. However, each of the three studies included is representative of the population living in the respective region, allowing a description of differences in the prevalence of headache types between the three included German areas. Among the limitations is also the fact that the extended headache question module allowing classification of a second headache type and more rare forms could be applied only in the Dortmund region and that in the southern study population the very young age group was lacking.
In summary, we have found considerable regional variations in the prevalence of single headache types within Germany. Causes contributing to these regional variations are speculative and cannot be assessed using a cross-sectional study design. Differences in common risk factors and comorbid conditions, and social disparities might contribute to the variation. Our results suggest that the regional burden of headache subtypes is quite different even in smaller countries such as Germany, indicating the need for detailed planning when implementing specialized treatment and care institutions.
Footnotes
Acknowledgements
The German DMKG Headache Study was supported by the German Migraine & Headache Society (DMKG) and by unrestricted grants of equal share from Astra Zeneca, Berlin Chemie, Boots Healthcare, GlaxoSmithKline, McNeil Pharma (former Woelm Pharma), MSD Sharp & Dohme, and Pfizer. The Study of Health in Pomerania (SHIP) is funded by grants from the German Federal Ministry of Education and Research (BMBF 01ZZ96030), the Ministry for Education, Research and Cultural Affairs and the Ministry for Social Affairs of the Federal State of Mecklenburg-Vorpommern. The KORA research platform and the MONICA Augsburg studies were initiated and financed by the Helmholtz Centre Munich, German Research Centre for Environmental Health (GmbH), which is funded by the German Federal Ministry of Education, Science, Research and Technology, and by the State of Bavaria.