
Abstract
We studied the interrelation of chronic tension-type headache with and without medication overuse (CTTH) and migraine in a random sample of 30 000 persons aged 30–44 years. They received a mailed questionnaire. Those with a possible chronic headache were interviewed by neurological residents. The International Classification of Headache Disorders was used. A total of 386 persons had CTTH. Compared with the general population, men had a 2.8-fold and women a 2.4-fold significantly increased risk of migraine without aura (MO). The risk of migraine with aura (MA) was not increased. The mean age at onset of CTTH was significantly higher in those with than in those without co-occurrence of MO. Bilateral MO attacks were significantly more frequent in those with age at onset of CTTH prior to age at onset of MO compared with those with age at onset in reverse order. CTTH and MO are interrelated, possibly in a complex matter. In contrast, CTTH and MA are not interrelated.
Introduction
Headache is the most common type of pain, as nearly everybody has experienced headache at least once in their life. The International Classification of Headache Disorders (ICHD) divides headaches into primary and secondary forms (1). The most common primary headaches are tension-type headache (TTH) and migraine (2–4), whereas the most common secondary headaches are induced by alcohol, fever, hunger and rhinosinusitis (5). TTH and migraine are usually paroxystic disorders, but sometimes they appear in a chronic form, i.e. the headache frequency increases to ≥ 15 days/month for at least 3 months. The prevalence of chronic tension-type headache with or without medication overuse (CTTH) is 2–3% in the general population (2, 6–10). The prevalence of TTH is similar or slightly greater in migraineurs than in non-migraineurs, whereas the frequency of TTH is significantly higher in migraineurs than in non-migraineurs (11–13). What causes this interrelationship of TTH and migraine? Can abortive attacks of migraine mimic TTH, or can aggravated attacks of TTH mimic migraine? Are other mechanisms such as medication overuse involved?
The aim of this study was to investigate the interrelation of CTTH and migraine in a chronic headache sample of 30–44-year-olds from the general population.
Materials and methods
A representative, random, age-stratified sample of 15 000 men and 15 000 women, 30–44 years old and residing in the 20 eastern municipalities in Akershus County, was drawn from the National Personal Registry by Statistics Norway. Akershus County has both rural and urban areas and is situated in close proximity to Oslo. All persons received a mailed questionnaire.
Respondents with possible chronic headache, i.e. those with ≥ 15 days with self-reported headache within the last month or with ≥ 180 days with self-reported headache within the last year were invited to a semistructured headache interview. Two neurological residents experienced in headache diagnostics conducted all interviews and the physical and neurological examinations. Specific emphasis was given to the age at onset questions by relating it to other life events in order to reduce recall bias. The explicit diagnostic criteria of the ICHD and the revised criteria for medication-overuse headache were applied (1, 14–16). The study took place at the Akershus University Hospital in 2005. The response rate of the questionnaire was 71% and the participation rate of the interview was 74%. A more detailed description of the materials and methods has been given elsewhere (9, 10).
The prevalence of migraine is derived from a Danish epidemiological survey of the general population. A sample of 3000 men and 1000 women, all 40 years old, was drawn from the Danish Central Person Registry. They received a short migraine screening questionnaire, which had a response rate of 87%. Those with possible migraine were interviewed by a physician. The participation rate of the interview was 87%. Kappa was 0.77 validating self-reported migraine in the questionnaire against the diagnosis of the clinical interview. A more detailed description has been published elsewhere (17). The calculations of relative risk (RR) of migraine are based on our data compared with the Danish epidemiological survey (for details see next section).
Data processing and statistical methods
The statistical analyses were performed using
Ethical issues
The Regional Committees for Medical Research Ethics and the Norwegian Social Science Data Services approved the project. Participation was based on informed consent.
Results
Of all 386 (83 men and 303 women) persons with CTTH, 170 (40 men and 130 women) had medication overuse and 216 (43 men and 173 women) had no medication overuse.
Prevalence of migraine
Of the 386 persons with CTTH, 162 had MO and 31 had MA. The prevalence of MO was not significantly different in those with and without medication overuse in either gender (men 14/40 vs. 7/43; P > 0.05, and women 65/130 vs. 76/173; P > 0.05). Nor did prophylactic medication influence co-occurrence of migraine. Table 1 shows the prevalence of MO and MA in those with CTTH and in the general population. Compared with the general population, the RR of MO was significantly increased 2.8-fold (95% CI 1.9, 4.0) in men with CTTH and 2.4-fold (95% CI 2.1, 2.7) in women with CTTH. The relative risk of MA was not increased in either gender with CTTH [men 1.2 (95% CI 0.6, 2.5), and women 0.9 (95% CI 0.6, 1.3)].
Adjusted prevalences of migraine without aura (MO) and migraine with aura (MA) in people with chronic tension-type headache with or without medication overuse (CTTH)

CTTH<MO is age at onset of CTTH prior to age at onset of MO.
Age at onset
Table 2 shows that the mean age at onset of CTTH and MO was not influenced by medication overuse. Men had a significantly higher mean age at onset of CTTH than women, whereas the mean age at onset of MO was equal in both genders. Men had a significantly higher mean age at onset of CTTH than MO, whereas it was equal in women.
The mean age at onset of chronic tension-type headache and migraine without aura in relation to medication overuse

Table 3 shows that the mean age at onset of CTTH in both genders was significantly lower in those with than in those without MO.
The mean age at onset of chronic tension-type headache in relation to migraine without aura
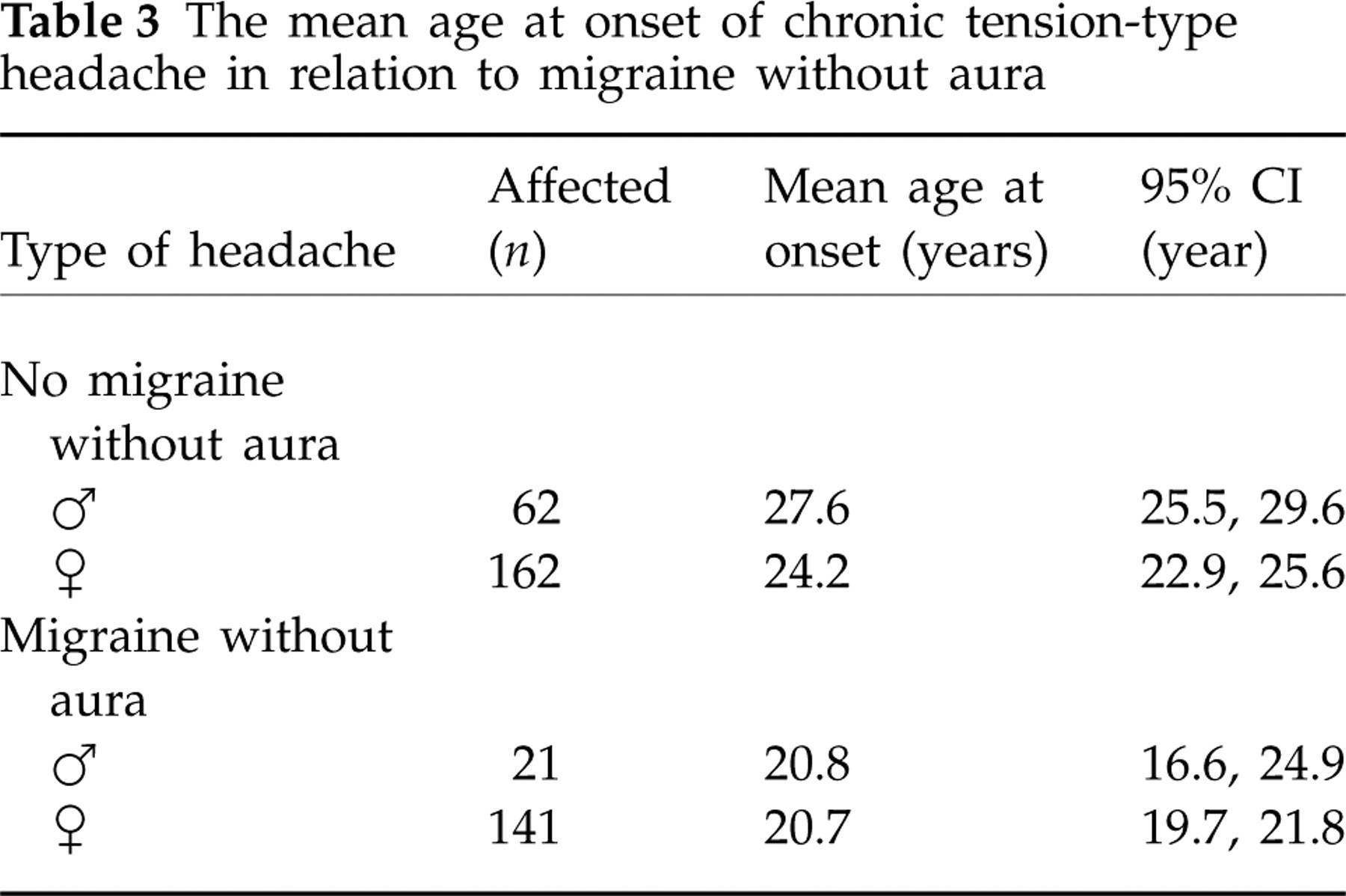
Table 4 shows the relation of mean age at onset of CTTH and MO. The mean age at onset was not significantly different between men and women, or between those with and without medication overuse.
The relation of age at onset of chronic tension-type headache with or without medication overuse (CTTH) and migraine without aura (MO)
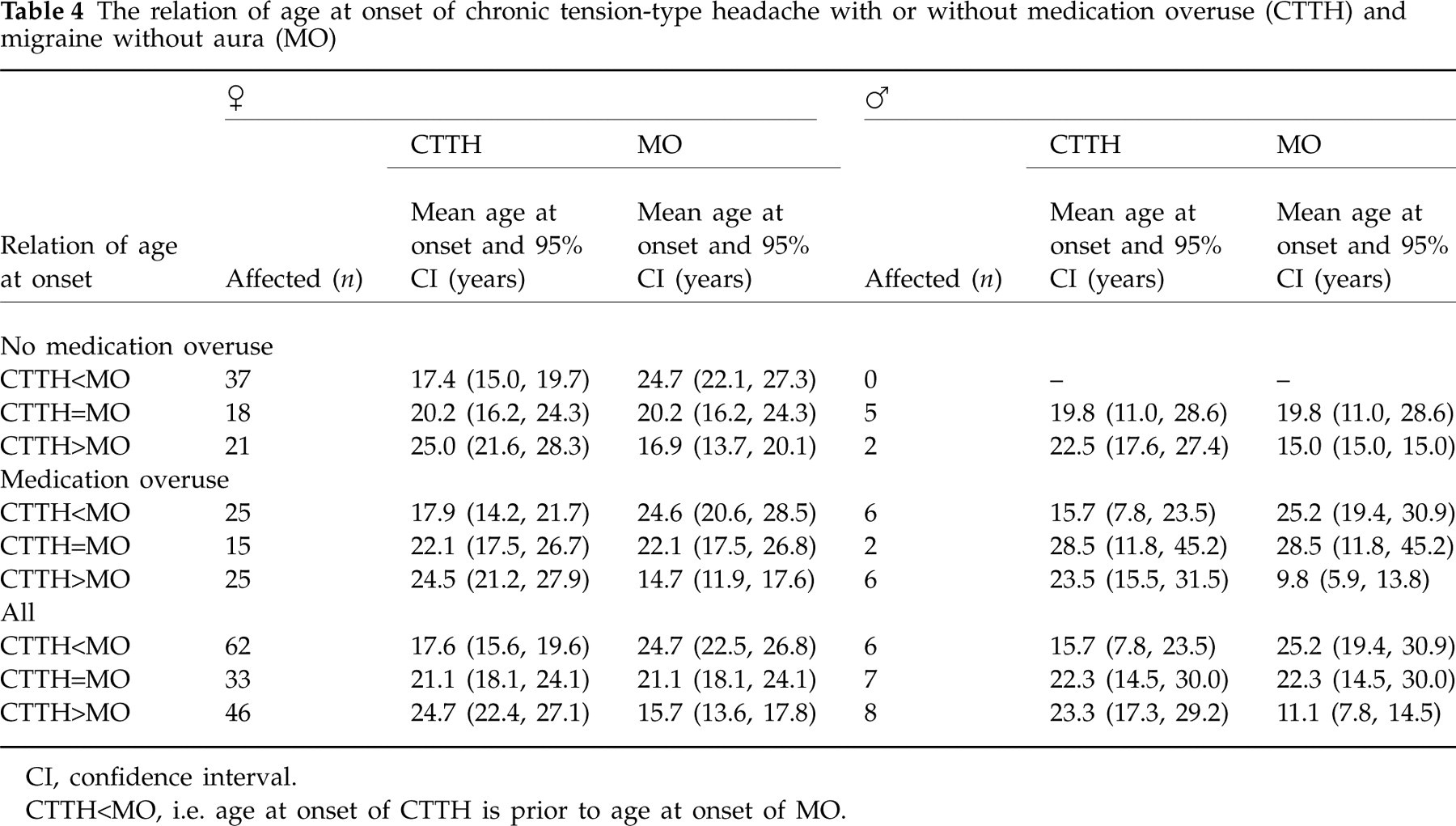
CI, confidence interval.
CTTH<MO, i.e. age at onset of CTTH is prior to age at onset of MO.
Migraine without aura
Of the 162 persons with MO, 13 (two men and 11 women) had no attacks of MO within the last year. Among those with MO within the last year, 27.5% (41/149) had between 1 and 11 days with MO, 68.5% (102/149) had between 12 and 179 days with MO, and 4.0% (6/149) had ≥ 180 days with MO. Eight fulfilled the revised criteria for chronic migraine and 16 fulfilled the diagnosis of probable chronic migraine.
The frequency of MO was independent of the age at onset relation between CTTH and MO (P = 0.289). An analysis of the pain characteristics (location, quality, intensity and aggravation by routine physical activity) and accompanying symptoms (nausea, vomiting, photophobia and phonophobia) of MO showed no significant differences between those with and those without medication overuse, either in men or in women. Analysis of the three different age at onset categories relating age at onset of CTTH and MO showed that the subgroup CTTH<MO had significantly more bilateral MO than the CTTH>MO subgroup (39/68 vs. 19/54; P = 0.018). Other MO pain characteristics and accompanying symptoms were not significantly different between the three age at onset categories.
Chronic tension-type headache
Analysis of pain characteristics and accompanying symptoms of CTTH showed no significant differences except that pressing/tightening headache was experienced slightly more in subjects with than without medication overuse (170/170 vs. 210/216; P = 0.037). A similar analysis in those with and without MO showed no significant differences. Analyses of the subgroups CTTH<MO and CTTH>MO revealed no significant differences in pain characteristics or accompanying symptoms analysed separately by gender, but women experienced nausea significantly more often than men (54/332 vs. 5/78; P = 0.019).
Discussion
Methodological considerations
The sample size was chosen to ensure adequate numbers of people with chronic headache for accurate descriptive statistics. The age range 30–44 years was chosen because the prevalence of chronic headache is relatively higher than in a younger age range, whereas comorbidity of other diseases is less than in an older age range. As this was an epidemiological survey on headache, headache may be over-represented among responders of the questionnaire. However, similar replies to the first, second and third issued questionnaire imply that this was not the case. Furthermore, a previous Danish epidemiological survey based on a short migraine screening questionnaire found no significant difference in the frequency of migraine among responders and non-responders (17). Questionnaires are generally not valid for diagnosing headaches (20). However, short, simple questions are more valid, as has been discussed previously (13, 17, 20). Making specific headache diagnoses is not an easy task, especially among those with chronic headache and those with co-occurrence of several headaches. The gold standard is an interview and physical and neurological examination by a physician experienced in headache diagnostics. For that reason, neurological residents with experience in headache diagnostics conducted our investigation. Although prospective headache diaries can provide detailed descriptions, we refrained from the use of such instruments in our population-based epidemiological survey, since compliance is far from 100% and the participation rate would decrease (21, 22). In our epidemiological survey the diagnosis medication-overuse headache was applied to persons with chronic headache and medication overuse, in accordance with revised criteria of the ICHD (16).
Our data were adjusted according to age and gender when compared with Danish prevalence data, due to the different age and gender composition in order to make the data comparable (17). These data must be interpreted with care, since they were collected from different populations at different time periods. A direct comparison in the Norwegian population would have been preferable, but valid data on migraine prevalence are not available from Norway. Thus, we compared the most valid data available. Our analyses focused on gender as well as the whole sample. However, the number of men in some of the subsamples is relative small and may have rendered type 2 errors.
Results
Our results indicate that CTTH and MO are interrelated, as the prevalence of MO is significantly increased among those with CTTH compared with the general population (Table 1). In contrast, CTTH and MA do not seem to be interrelated, as the prevalence of MA among those with CTTH corresponds to that in the general population (Table 1). The frequency of MO was much higher in those with CTTH than in those from the general population, as only 27.5% (0.21–0.35) of our patients had MO 1–11 days within the last year compared with 87.3% (0.73–0.94) in the general population (23). This might indicate an association between MO and CTTH. Table 1 also shows the relation of age at onset between CTTH and MO and MA analysed separately by gender in three subgroups. The increased risk of MO cannot specifically be allocated to one or more of the three age at onset categories. Thus, the increased risk of MO is probably caused by a contribution from all three age at onset categories. The fact that MO is bilateral in 65% among those with age at onset of CTTH prior to MO, but only 43% among those with age at onset of MO prior to CTTH, suggests that MO might evolve from CTTH in some patients, as bilateral headache is a more common symptom in TTH than in migraine. Bilateral MO was reported by 45% of those from the general Danish population (24). The possible interrelation between CTTH and MO is further strengthened by the observation that the mean age at onset of CTTH was significantly higher in those without than those with co-occurrence of MO (Table 3). Central sensitization is probably of major importance in CTTH (25–27), and the change from CTTH to co-occurrence of CTTH and MO might be caused by the same mechanisms.
About 25% (40/162) reported equal age at onset of CTTH and MO. Thus, the interrelation of CTTH and MO cannot be determined in this group by age at onset. About 33% (54/162) had age at onset of MO prior to CTTH. Can an abortive attack of MO simulate TTH characteristics? We cannot exclude that, but > 75% of the general population experience TTH, whereas < 25% experience migraine (3, 4, 17, 28). Thus, the majority of people have TTH unrelated to migraine. However, an investigation of migraineurs with severe disability has shown a significant effect of sumatriptan in the treatment of migraine, migrainous and tension-type headaches (29). One possible reason might be treatment of abortive attacks of migraine. We have experienced that some patients with co-occurrence of frequent MO and CTTH sometimes respond well to prophylactic migraine medication, with a reduction in the number of migraine attacks as well as disappearance of their TTH. Central sensitization is likely to be involved in these patients, occurring as a result of repeated MO attacks developing into CTTH over time.
Evaluation of the literature is complicated, since terms like chronic daily headache (CDH) and transformed migraine (TM) encompassing unspecified headache diagnoses are frequently used, although not recognized in the ICHD (1, 29–31). CDH is a headache that occurs > 15 days per month, whereas TM is a headache that evolves from migraine. In our sample, some of those with age at onset of MO prior to age at onset of CTTH might meet the criteria for TM. However, our population-based data can neither confirm nor reject the hypothesis that CM is an earlier stage of TM, as has been proposed based on an investigation of 402 persons with TM from a headache centre (30). A population-based survey of CDH based on lay telephone interviews has shown that the headache frequency decreased in 71%, while 3% of controls developed CDH (31). Since our epidemiological survey is cross-sectional, we do not have serial data for comparison. However, although different headache definitions are used in the literature, a classification alone is not likely to shed light on the pathophysiology or aetiology. What causes mixed headache diagnoses is not known, and different theories have been suggested. Several mechanisms are possibly involved, and it has been debated whether mixed chronic headaches represent different evolutionary stages of chronification. Medication overuse complicates matters further. However, medication overuse seemed to have no influence on the interrelation between MO and CTTH.
The ICHD includes mild nausea in the criteria for CTTH (1). Of the 386 people with CTTH, five men and 49 women had mild nausea, an accompanying symptom usually experienced by migraineurs. The relationship between nausea in CTTH and MO is a complicated issue, since nausea is not allowed as accompanying symptom in infrequent and frequent TTH.
The interrelation of CTTH and MO is complex, and is most likely to be influenced by different mechanisms. Hopefully, pathophysiological studies can further elucidate the interrelation of CTTH and MO, since genetic studies of MO and CTTH seem unlikely to give an answer to this question in the near future.
Footnotes
Acknowledgements
This study was supported by grants from East Norway Regional Health Authority and Faculty Division Akershus University Hospital. The authors thank Akershus University Hospital for providing research facilities.