Objectives: To assess whether migraine patients display a chronic nitric oxide synthase (NOS) hyperactivity by comparing the nitric oxide (NO) production before and following a loading dose of L-arginine between migraine patients (interictally) and matched healthy control subjects. In addition, we evaluated whether a loading dose of L-arginine triggers an acute migraine headache in migraineurs.
Subjects and methods: Twenty healthy subjects and 20 migraine patients participated in a 2-period, randomised, double-blind, placebo-controlled study. Each subject received a 30-min infusion, by peripheral vein, of 30 g L-arginine hydrochloride or placebo (i.e. an equal volume of 0.9% saline solution). Meanwhile, biomarkers associated with the L-arginine–NO pathway (i.e. exhaled NO/nasal NO), plasma citrulline and urinary excretion of nitrite/nitrate and cGMP were assessed before and for 6 h following the start of the infusion.
Results: At baseline, exhaled NO and nasal NO were higher in migraineurs compared to healthy subjects (mean ± 95% confidence interval): 15.9 (8.8, 23.0) parts per billion (ppb) versus 10.8 (7.0, 14.5) ppb for exhaled NO (P = 0.04) and 76.3 (61.2, 91.4) versus 61.6 (51.2, 72.0) ppb for nasal NO (P = 0.03), respectively. The AUC0–6 in ppb for exhaled NO and nasal NO following L-arginine or saline infusion did not differ between both groups. The increase in L-citrulline, following L-arginine infusion, was smaller in migraine patients (15 (13, 18) µmol/l) compared to healthy volunteers (19 (16, 23) µmol/l; P = 0.046). In healthy subjects, both nitrate and cGMP excretion were higher following L-arginine compared to placebo infusion: 132.63 (100.24, 165.02) versus 92.07 (66.33, 117.82) µmol/mmol creatinine for nitrate (P = 0.014) and 50.53 (42.19, 58.87) versus 39.64 (33.94, 45.34) nmol/mmol creatinine for cGMP (P = 0.0003), respectively. In migraineurs, excretion of these biomarkers was comparable following L-arginine or saline infusion.
Conclusions: The results of the present study do not support the idea of a generalised increase in NO synthase activity in migraine patients outside of a migraine attack. The smaller increase in plasma L-citrulline, urinary nitrate and cGMP excretion following L-arginine infusion in migraine patients might indicate dysfunction of endothelial NO synthase.
Olesen et al. (1) proposed that nitric oxide (NO) plays a crucial role in the pathophysiology of migraine headache. They observed that both administration of exogenous NO donors and stimulation of endogenous NO production by histamine induce delayed headaches in migraineurs, which resemble the characteristics of spontaneous migraine attacks (2–4). In addition, they reported that the non-specific NO synthase inhibitor NG-monomethyl-L-arginine (L-NMMA) provides pain relief to patients experiencing a spontaneous migraine headache (5). Numerous studies suggested an increased NO production in migraineurs, both ictally and interictally, but did not permit a conclusive and final answer regarding the presumed hyperactivity of the L-arginine–NO pathway (6–9). Recently, our group observed plasma levels of 3-nitrotyrosine, a relevant biomarker of NO-dependent oxidative stress, which were over 4-fold higher during a migraine headache compared to in between attacks (10,11). All these observations have strengthened the belief that NO is a key molecule in the pathogenesis of migraine. Caution, however, is warranted, as one of the major difficulties encountered in all studies is the elusive nature of the NO molecule (12). The search for stable end-products of NO furnished inconsistent results. In addition, inhibition of NO synthesis, for a long time seen as a promising target for the treatment of migraine headache, has recently fallen short of expectations (10,13,14).
Three isoforms of NO synthase (NOS) are distinguished: inducible NOS (iNOS or NOS II) and two constitutively expressed NOS isoforms – neuronal NOS (nNOS or NOS I) and endothelial NOS (eNOS or NOS III), respectively. As inhibition of eNOS is undesirable due to its wide-spread physiological role in healthy vascular tissue, research has focused on the development of potent and specific iNOS inhibitors (15,16). Potent iNOS inhibitors unfortunately failed to show any beneficial effect in both the acute and prophylactic treatment of migraine (10,13,14). Despite these recent findings, evidence to support NOS as a potential target for migraine treatment remains strong. In particular for nNOS, which is expressed throughout the trigeminal system and plays an important role in the sensitisation of spinal second order nociceptors (17,18). Neuronal NOS inhibition was shown to have antagonist actions within the trigeminovascular system, thereby reducing neurogenic dural vasodilation (19). It has been suggested that the delayed headache induced by the administration of an NO donor is due to nNOS activation leading to the production of more NO and the subsequent activation of the trigeminovascular system. Therefore, nNOS might be an interesting target for the treatment of migraine and the question whether NO plays a role in the pathophysiology of migraine thus remains unanswered (19,20).
In the present study, the objective was to assess whether migraine patients display a chronic, interictal, NOS hyperactivity. Endogenous NO is synthesised by NOS from the amino-acid L-arginine, yielding L-citrulline as a by-product. The administration of L-arginine in humans results in an increase of exhaled NO and nasal NO, a slight decrease in mean arterial pressure (MAP), an increased plasma citrulline concentration and an increase in urinary nitrate and cyclic guanosine monophosphate (cGMP) (21,22). If the L-arginine/NO conversion in migraine patients is increased due to NOS hyperactivity, this should be reflected by the associated biomarkers characteristic for NO production (exhaled NO, nasal NO, plasma L-citrulline and L-arginine and urinary nitrite/nitrate and cGMP). In addition, the administration of L-arginine would result in a larger increase of NO production in migraine patients compared to healthy volunteers. Furthermore, the increase in NO might provoke a delayed migraine headache in migraineurs as seen following the administration of exogenous NO donors.
To that end, this study compares the NO production before and following a loading dose of intravenously administered L-arginine between a group of migraine patients outside of a migraine headache period and a matched group of healthy control subjects. In addition, we evaluated whether a loading dose of L-arginine triggers an acute migraine headache in migraineurs.
Subjects and methods
Subjects
After approval by the ethics committee of the University Hospital of Leuven, 30 migraine patients with or without aura, as defined by the International Headache Society diagnostic criteria, were recruited (23). In addition, 32 healthy volunteers matched for age, gender and body mass index (BMI) were screened from the general population. Major exclusion criteria were: age <18 years and ≥50 years, history suggestive of asthma, rhinitis or atopy, history of severe herpes infection (i.e. contra-indication for L-arginine administration), diabetes, history of cardiovascular disease, smoking, hypertension (systolic blood pressure > 140 mmHg or diastolic blood pressure > 90 mmHg), pregnancy or lactation and use of chronic drugs (except hormonal contraceptives). Migraine patients with a history of migraine <6 months, having >15 days of headache per month at any given time since the onset of migraine attacks, using anti-migraine drugs > 10 days/month or using prophylactic medication, were excluded. Control subjects experiencing more than one headache per month, with a history of moderate or severe headaches or migraine headache or with a first degree relative with migraine were excluded. Female subjects had to use oral, injected or implanted hormonal methods of contraception from at least the commencement of their last normal menstrual period prior to the first administration of the challenge agent.
The diagnosis of migraine was made by a neurologist or general physician in accordance with the International Headache Society diagnostic criteria (23). Migraine patients fulfilling criteria for both migraine with and without aura were considered as migraine patients with aura. The Migraine Disability Assessment Score (MIDAS) was used to assess headache-related disability (24).
Based on the medical history, physical examination and routine laboratory tests, 9 patients and 11 healthy volunteers were excluded. From the remaining 21 migraine patients, one was excluded because of severe hypotension following L-arginine administration. One of the healthy volunteers withdrew from the study because of the difficult venous puncture. The 20 remaining migraine patients and 20 healthy volunteers completed the study successfully. The study flow chart is provided in Appendix 1.
The study was conducted in accordance with the Declaration of Helsinki. All subjects provided written informed consent prior to participation.
Study design
All eligible subjects participated in a 2-period, randomised, double-blind, placebo-controlled study. Each subject received a 30-min infusion, by peripheral vein, of 30 g L-arginine hydrochloride (R-Gene®, 100 ml of 10% arginine hydrochloride injection for intravenous use, Pfizer Inc., New York, NY, USA) or an equal volume of 0.9% saline solution (B Braun, Melsungen, Germany) as per the flow chart in Figure 1. There was at least a 7-day washout interval between both study periods. The infusion was always administered in the morning in order to avoid potential diurnal variations. Placebo and L-arginine doses were given under the supervision of a research physician.
Flow chart of the study protocol. The horizontal axis represents a time scale indicating the start of supine rest, the start and stop of infusion of L-arginine, the time of the meal for the study volunteer and the end of in hospital stay. At baseline and at 60 min, a blood sample was taken. NO indicates exhaled NO and nasal NO measurements (3 times); BP indicates measurement of vital signs (2 times).
Measurements
Measurements were performed in a quiet, temperature-controlled (23 ± 1°C) room. Female subjects were studied outside the ‘pill-free’ period. Each subject received a list of dietary sources of nitrates/nitrites (e.g. red meat or cured meat) and was instructed to refrain from such foods for at least 48 h before the start of the experiments. Subjects abstained from any drugs (except oral contraceptives) for at least 3 days. Migraine patients had to be headache free for at least 3 days. Subjects fasted at least 8 h before L-arginine or placebo administration and no food was allowed until 4 h and 15 min after the infusion. Six hours and 15 min after the infusion, subjects were allowed to go home but were still expected to refrain from dietary sources of nitrates/nitrites up to 24 h after L-arginine infusion, as was required in the 48-h period prior to the experimental session.
In each study period, during the 60 min period following the start of the infusion, exhaled NO, nasal NO, blood pressure and heart rate were measured at 15-min intervals. Measurements were repeated at 1.5, 2, 4, 6 and 24 h after the start of the infusion (Figure 1).
Blood samples for L-citrulline and L-arginine were taken at baseline and 1 h after the start of the infusion (Figure 1). Urine was collected for cGMP and nitrite/nitrate assays. The collection was performed during the 6-h period following the start of the L-arginine/placebo infusion. The headache response was evaluated according to the criteria of the International Headache Society (IHS, 2004) in the 24-h period following the administration of the L-arginine/placebo loading dose. Headache intensity was scored on a visual scale that measures from 0 to 10.
Brachial blood pressure and heart rate
Supine systolic blood pressure (SBP), diastolic blood pressure (DBP) and heart rate (HR) were recorded at the left upper arm by use of a validated, non-invasive semi-automated oscillometric device (OMRON 705IT; Omron Healthcare, Hamburg, Germany) (25). At each time-point, measurements were performed twice, and the mean was used for analyses.
Exhaled and nasal NO
During each study period, exhaled NO and nasal NO were measured using the CLD 88sp NO analyzer supplied by Eco Medics, UK. At each time-point, exhaled NO and nasal NO were measured three times and the mean of these three readings was used for analysis. The expired NO was measured using a chemiluminescence analyzer (CLD 88sp, Eco Medics, Switzerland) with a lower and upper limit of detection that were 0.002 ppb and 5 ppb, respectively. The instrument was calibrated at 0 ppb and 400 ppb as recommended by the manufacturer. Exhaled NO and nasal NO measurements were performed according to the guidelines of the American Thoracic Society (ATS) (26). The subjects were asked to exhale at a constant flow, which they could readily see displayed on the computer screen in the form of a bar that remained red until target flow was obtained, and then turned green. If the flow dropped below, or increased above, the desired range, the green bar changed back to red. The influence of ambient NO levels was excluded by placing an NO-scrubbing filter in the inspiratory limb of the collection apparatus.
Plasma L-arginine and L-citrulline
Plasma L-arginine and L-citrulline concentrations were determined by liquid chromatography (LC)-tandem mass spectrometry (MS) analysis as described by Chace et al (27).
A 50-µl aliquot of plasma was spiked with stable isotope-labeled L-arginine and L-citrulline, which served as internal standards. Protein was precipitated with 100 µl of methanol, filtered through a 0.22-µm hydrophilic membrane (Multiscreen HTS™; Millipore, Molsheim, France), derivatised with butanolic HCl (1 N, 65°C, 17 min) and analysed by LC-tandem MS. Quantification was performed by selected reaction monitoring of the respective daughter ions of analytes and internal standards.
Urinary nitrite/nitrate concentrations
Urinary nitrite/nitrate levels were determined using nitrate reductase and the colorimetric Griess reaction (28). A 1 : 4 dilution in PBS of the urinary samples (200 µl) was ultra filtered (6000 g, 45 min, 4°C) through 10,000-kDa molecular weight filters (Ultrafree-MC Biomax; Millipore). Aliquots of the filtrates (50 µl) were analysed in duplicate. A standard curve was prepared, ranging from 0–50 µM, and was included in duplicate in each assay. Nitrate in the standards and samples was converted to nitrite by addition of 50 µl PBS with 600 U/l nitrate reductase from Aspergillus (Roche Diagnostics Corp.) and 100 µM NADH (Sigma-Aldrich). Complete conversion was achieved with an incubation time of 4 h at room temperature, as evaluated by comparison of a converted nitrate standard curve with a nitrite standard curve. Nitrite was then measured after addition of 50 µl PBS, 50 µl 1% sulfanilamide in 5% phosphoric acid and 50 µl 0.1% N-(1-naphthyl)ethylenediamine dihydrochloride. The absorbance was read at 540 nm and corrected for absorbance at 650 nm. Urinary excretion rates of nitrite/nitrate were corrected for creatinine excretion.
Urinary cGMP levels were determined by a cGMP enzyme immunoassay (R&D systems Europe, Ltd). This assay is commercially available and based on the competitive binding technique in which cGMP, present in the sample, competes with a fixed amount of horseradish peroxidase (HRP)-labeled cGMP for sites on a rabbit polyclonal antibody. During the incubation, the polyclonal antibody becomes bound to a goat anti-rabbit antibody coated onto a microplate. Following a wash to remove excess conjugate and unbound sample, a substrate solution is added to the wells to determine the bound enzyme activity. The colour development is stopped and the absorbance is read at 450 nm. The intensity of the color is inversely proportional to the concentration of cGMP in the sample.
Statistical analysis
Exhaled and nasal NO values are expressed in parts per billion (ppb). The change in exhaled NO and nasal NO following L-arginine or placebo administration is expressed as the absolute change from baseline in ppb. At each time-point, the mean of observations and standard error of mean (SEM) are given.
As the data for exhaled NO and nasal NO are not normally distributed, they were ln-transformed prior to statistical analysis. The baseline values were then compared between migraine patients and healthy volunteers using a two sample Student’s t-test. Of the remaining time-points, only those from the 6 h of in-house stay were included in the analyses, as the measurements of the 24 h time-point proved to be unreliable due to poor compliance, notably with the dietary requirements. The areas under the curve from baseline up to 6 h following infusion (i.e. AUC0–6) were calculated as summary measures for the absolute values and for the change from baseline for exhaled NO and nasal NO. Subsequently, they were compared between migraine patients and healthy volunteers using a two sample Student’s t-test on ln-transformed data. The AUC0–6 for the absolute values and for the change from baseline were also compared between the L-arginine and the placebo period using a paired Student’s t-test after ln-transformation.
Plasma L-citrulline and L-arginine data are expressed in µmol/l. Both the baseline values and the values 1 h after the start of the infusion with L-arginine/placebo were compared between migraine patients and healthy volunteers using a two sample Student’s t-test. In addition, the L-arginine and the placebo period were compared using a paired Student’s t-test.
Urinary nitrite/nitrate and cGMP concentrations were simultaneously quantified to allow differentiation between impaired NO synthesis (in which case nitrite/nitrate levels and cGMP levels are expected to be low) and oxidative inactivation (in which case cGMP levels are expected to be low, but nitrite/nitrate levels should be normal) (29,30). Urinary nitrite/nitrate and cGMP concentrations were corrected by urinary creatinine concentrations to depict the urinary excretion rates of these metabolites and eliminate variability due to differences in renal excretory function (31). Both the values following L-arginine and saline infusion were compared between migraine patients and healthy volunteers using a two sample Student’s t-test on ln-transformed data. In addition, the L-arginine and the placebo period were compared using a paired Student’s t-test on ln-transformed data.
To analyze brachial blood pressure changes, the MAP was calculated. MAP is defined as the sum of the level of DBP plus one-third of the difference between SBP and DBP. The baseline MAP values were compared between migraine patients and healthy volunteers using a two sample Student’s t-test. In addition, the maximal decrease in MAP following L-arginine infusion was compared between migraineurs and healthy volunteers using a two sample Student’s t-test. Finally, the AUC0–6 for the MAP was compared between migraineurs and control subjects after placebo and L-arginine infusion by a two sample Student’s t-test.
Based on the within-subject standard deviation, observed in a reproducibility study with L-arginine infusions in 12 healthy volunteers, and given a type I error probability (α) of 0.05, sample size calculations were performed to provide 80% power for detecting a given difference between the group of patients and the healthy volunteers for the biomarkers exhaled NO, nasal NO and plasma L-citrulline. Thirteen subjects had to be included in each group in order to detect a 25% difference in the baseline values of nasal NO. 25% difference in the AUC0–6 of nasal NO after L-arginine administration, a sample size of only 11 subjects was needed. For exhaled NO, the sample sizes needed to detect a 25% difference were 55 and 43 subjects for the difference in baseline and AUC0–6, respectively. To detect a 25% difference in the increase of L-citrulline following L-arginine infusion, a sample size of six subjects was sufficient.
Results
Mean ± SD for age and BMI was 28 ± 8 years and 24 ± 3 kg/m2 for migraine patients and 27 ± 8 years and 24 ± 3 kg/m2 for healthy volunteers, respectively. Both groups consisted of 4 men and 16 women. Migraine patients had an average MIDAS (range) of 19 (2–46) and used no prophylactic medication. All patients and healthy volunteers completed the study. Except for one female healthy volunteer who developed severe genital herpes in the week following L-arginine administration, no adverse events of note were reported. Her data were included in the analysis as L-arginine was administered during the last study period.
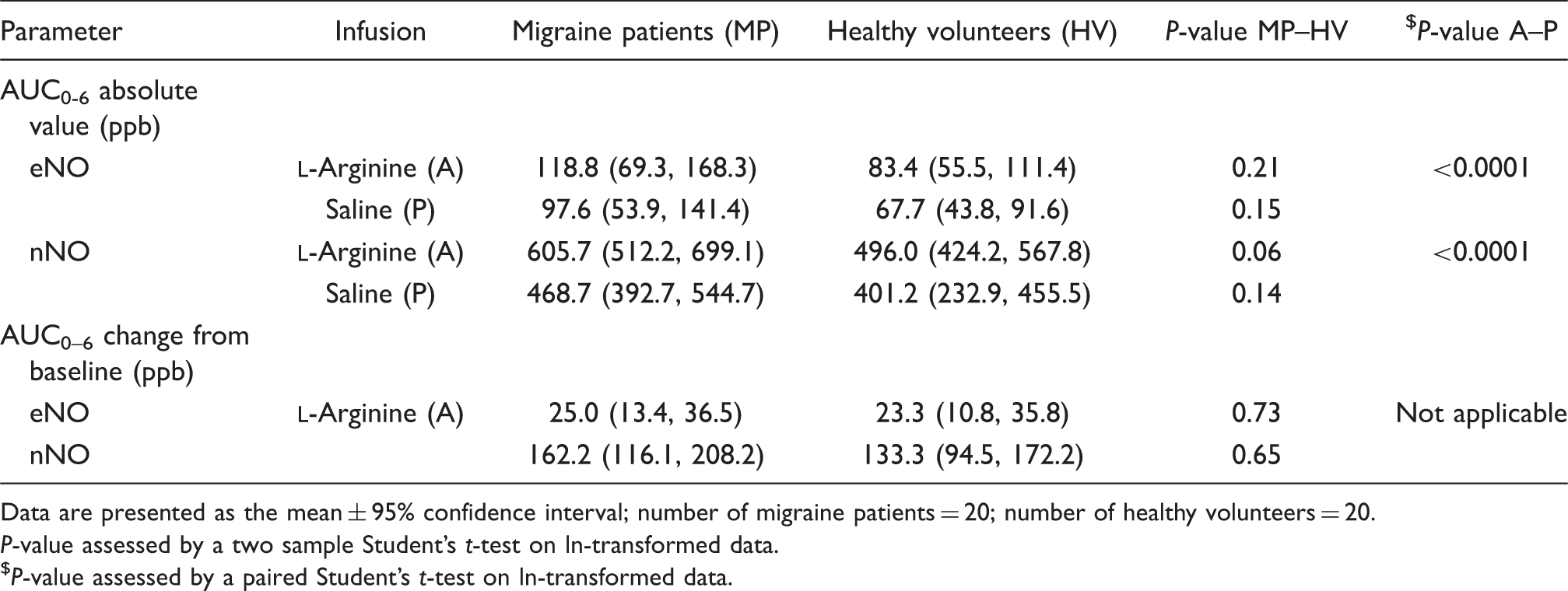
At baseline, both exhaled NO and nasal NO were significantly higher in migraineurs compared to healthy volunteers: 15.9 (8.8, 23.0) ppb compared to 10.8 (7.0, 14.5) ppb for exhaled NO (mean (95% CI), P = 0.04, two sample Student’s t-test) and 76.3 (61.2, 91.4) ppb compared to 61.6 (51.2, 72.0) ppb for nasal NO (mean (95% CI), P = 0.03, two sample Student’s t-test). Figure 2 shows exhaled NO and nasal NO following the infusion of L-arginine or saline. In Table 1, the AUC0–6 for the absolute value in ppb is given for both migraine patients and healthy volunteers following L-arginine or saline infusion. In addition the AUC0–6 for the change from baseline is given for the period in which L-arginine was infused.
(A) Exhaled NO (mean ± SEM); number of migraine patients = 20; number of healthy volunteers = 20. Diamonds, migraine patients, squares, healthy volunteers. Full line and symbols correspond to the period in which L-arginine was infused; dotted lines and open symbols correspond to the placebo period. (B) Nasal NO (mean ± SEM); number of migraine patients = 20; number of healthy volunteers = 20. Diamonds, migraine patients, squares, healthy volunteers. Full line and symbols correspond to the period in which L-arginine was infused; dotted lines and open symbols correspond to the placebo period.
AUC0–6 for the absolute value of exhaled NO (eNO) and nasal NO (nNO) and for the change from baseline during the L-arginine period
Data are presented as the mean ± 95% confidence interval; number of migraine patients = 20; number of healthy volunteers = 20.
P-value assessed by a two sample Student’s t-test on ln-transformed data.
P-value assessed by a paired Student’s t-test on ln-transformed data.
Plasma L-citrulline levels at baseline did not differ averaging 26 (23, 29) and 29 (26, 32) µmol/l for migraine patients and healthy volunteers, respectively (mean (95% CI), P = 0.32, two sample Student’s t-test). The increase in L-citrulline following L-arginine infusion was smaller in migraine patients (mean (95% CI), 15 (13, 18) µmol/l) compared to healthy volunteers (mean (95% CI), 19 (16,23) µmol/l; P = 0.046, two sample Student’s t-test) (Figure 3A). Plasma levels of L-arginine were similar at baseline at 65 (56,75) and 68 (60, 76) µmol/l for migraine patients and healthy volunteers, respectively (mean (95% CI), P = 0.66, two sample Student’s t-test). Plasma L-arginine levels increased after L-arginine infusion by 2602 (2267, 2937) and 2651 (2391, 2910) µmol/l in migraine patients and healthy volunteers, respectively (mean (95% CI), P = 0.81, two sample Student’s t-test; Figure 3B).
(A) L-Citrulline (mean ± SEM); number of migraine patients = 20; number of healthy volunteers = 20. HV, healthy volunteers; MP, migraine patients. P, two sample Student’s t-test comparing migraine patients to healthy volunteers. $P, paired Student’s t-test comparing baseline to 1 h post-arginine. (B) L-Arginine (mean ± SEM); number of migraine patients = 20; number of healthy volunteers = 20. HV, healthy volunteers; MP, migraine patients. P, two sample Student’s t-test comparing migraine patients to healthy volunteers. $P, paired Student’s t-test comparing baseline to 1 h post-arginine.
Urinary nitrite/nitrate and cGMP excretion did not differ between migraine patients and healthy volunteers during the placebo period (Table 2). Interestingly, whereas no significant increase in urinary nitrite/nitrate and cGMP excretion could be detected in migraine patients between the L-arginine and the placebo period, there was a significant increase of both biomarkers in healthy volunteers following L-arginine infusion (Table 2).
Urinary nitrite/nitrate and cGMP excretion from 0–6 h after infusion
P-value comparing nitrite/nitrate excretion between saline and L-arginine period
0.21
0.014
Not applicable
P-value comparing cGMP excretion between saline and L-arginine period
0.99
0.0003
Data are presented as the mean ± 95% confidence interval; number of migraine patients = 20; number of healthy volunteers = 20.
P-value assessed by a two sample Student’s t-test on ln-transformed data.
P-value assessed by a paired Student’s t-test on ln-transformed data.
MAP was similar at baseline in migraine patients and healthy volunteers. The maximal decrease in MAP following L-arginine infusion did not differ between migraine patients and healthy volunteers: −11 (−14, −8) mmHg in migraine patients versus −10 (−13, −8) mmHg in healthy volunteers (mean (95% CI); P = 0.72, two sample Student’s t-test). In addition, no difference in AUC0–6 was detected between migraine patients and healthy volunteers following L-arginine or placebo infusion (Figure 4).
Mean arterial pressure (mean ± SEM); number of migraine patients = 20; number of healthy = 20. Diamonds, migraine patients; squares, healthy volunteers. Full line and symbols correspond to the period in which L-arginine was infused; dotted lines and open symbols correspond to the placebo period.
Seven migraine patients developed a migraine headache in the 72-h interval following L-arginine infusion. Three of those also developed a migraine headache after saline infusion. In total, seven patients developed migraine following placebo administration. None of the biomarkers was significantly different between those patients who developed a migraine headache and those who did not.
Discussion
The results of the present study do not support the idea of a generalised increase in NO synthase activity in migraine patients outside of a migraine attack. When comparing migraine patients to healthy subjects, challenge with L-arginine does not result in a larger increase in biomarkers associated with NO production (i.e. exhaled NO, nasal NO, plasma L-citrulline and urinary excretion of nitrite/nitrate and cGMP). On the contrary, following L-arginine infusion, the increase in plasma L-citrulline levels and urinary excretion of nitrite/nitrate and cGMP is smaller in migraine patients compared to healthy volunteers.
L-Arginine infusion results in a systemic hypotensive response due to an increase in endogenous NO production as indicated by both the increased plasma L-citrulline and the expired NO. The magnitude of the response to L-arginine infusion in our study is comparable to previous reports in healthy volunteers and confirms the concept that changes in expired NO may be a useful reflection of changes in systemic NO production (21).
An interesting finding in the present study is that the increase in L-citrulline following L-arginine infusion is slightly smaller in migraine patients. In addition, no significant increase in urinary nitrite/nitrate and cGMP excretion can be detected in migraine patients when the L-arginine period is compared to the placebo period. This is in sharp contrast with the healthy volunteers in whom a robust and significant increase in both urinary excretion of nitrate and cGMP is observed (Table 2). If anything, this would rather suggest a decreased NOS activity in migraine patients compared to healthy volunteers. The plasma L-citrulline level and the urinary excretion of nitrite/nitrate and cGMP largely depend on vascular eNOS activity (30–33). Therefore, the smaller increase in both plasma L-citrulline and urinary nitrite/nitrate and cGMP excretion following L-arginine challenge might indicate dysfunction of eNOS in migraine patients. This adds to the on-going discussion about migraine being an endotheliopathy leading to decreased eNOS activity (34). Indeed, several studies suggest that endothelial function is abnormal in migraine patients (35,36). Notably, our group conducted a study in which brachial artery flow mediated dilation (FMD) was measured to compare endothelial vasomotor function between migraine patients and healthy volunteers (37). FMD of the brachial artery was significantly decreased in migraine patients, suggesting that endothelial dysfunction is present in migraine patients and impedes on endothelium-dependent vasodilation. Our findings suggest that the decrease in endothelium-dependent vasodilation in migraineurs might be due to hypoactivity of eNOS. Nevertheless, reserve is warranted as large discrepancies exist between reports concerning endothelial function in migraine patients (38,39).
A second interesting finding is the slightly higher values at baseline for exhaled NO and nasal NO in migraine patients outside of an attack compared to healthy volunteers at baseline. L-Arginine is abundant in humans and, therefore, the absence of a higher increase in exhaled and nasal NO following L-arginine infusion in migraine patients might simply be a reflection of the fact that the L-arginine concentration is not the limiting factor for NO production in humans. Therefore, a challenge with L-arginine would not amplify the effect of increased NOS activity in migraine patients. Nevertheless, a significant increase in all biomarkers associated with systemic NO production is seen following L-arginine infusion and, therefore, increased NOS activity would be expected to lead to a greater increase in migraine patients. So, although it is tempting to hypothesise that the increase in expired NO at baseline reflects an increased NO production as part of the pathophysiology of migraine, such claims should, in view of our current results, be made cautiously. First, because the differences observed between both groups in the present study are small: expired NO is barely 5 ppb and 15 ppb higher in migraine patients compared to healthy volunteers for exhaled NO and nasal NO, respectively. Taking into account that the 5th and 95th percentiles for exhaled NO in healthy subjects are considered to be 4.5 ppb and 20.6 ppb for males while 3.6 ppb and 18.2 ppb for females, one can not but wonder what a 5 ppb difference in exhaled NO between two groups clinically implies (40). For nasal NO, the amplitude to ensure that a difference is genuine and not ascribable to the noise of measurement is even larger, which implies that interpretation of the difference in nasal NO between migraine patients and healthy volunteers might be over-interpretation (41). Second, it is generally accepted that expired NO is mainly of airway epithelial origin (42,43). Nevertheless, some studies have suggested that a systemic increase of NO production can translate into an increase in expired NO (21,44,45). In this study, however, none of the other biomarkers support differences in systemic NO production between migraine patients and healthy volunteers at baseline. Third and last, studies in humans demonstrate that iNOS is the most important contributor to the formation of NO in human breath (10,42). The potent iNOS inhibitor GW273629 was able to decrease both exhaled NO and nasal NO by approximately 80% (10). If excess NO would be present in the expired air of migraine patients, it would thus most likely be of iNOS origin. Whilst, until recently, iNOS was considered a promising target for the treatment of migraine, recent clinical trials have failed to show any efficacy of potent iNOS inhibitors, both in the acute and the prophylactic treatment of migraine headache (10,13,14). Consequently, whilst iNOS involvement in the pathophysiology of migraine can not entirely be excluded, other targets like nNOS look stronger candidates as a target in the treatment of migraine.
In those patients who developed a migraine headache following L-arginine or placebo infusion, no significant early increases in biomarkers associated with NO production are observed. This further discredits NO as a main player in the pathophysiology of migraine. Though, caution is warranted while interpreting the data concerning the latter, as these were retrieved only from the 14 patients who developed a migraine headache during one of the study periods.
The observed higher interictal exhaled NO and nasal NO values in migraine patients remain puzzling. In this respect, one might evoke the fact that an association between migraine and asthma, rhinitis and atopy has been reported by some authors (46,47). Nevertheless, other reports have denied such associations (48,49). Moreover, in this study, patients with a history or complaints suggestive of asthma, rhinitis or atopy were excluded, making it very unlikely that a potential association might have affected the data. Interpreting the higher exhaled NO and nasal NO values in migraineurs as a proof for the involvement of NO in the pathophysiology of migraine, would be thoughtless. Nonetheless, it would also be wrong to discard any role for NO in the pathophysiology of migraine solely based on the results of this study which has several limitations.
First, the biomarkers associated with the L-arginine-NO pathway are sampled peripherally and might thus not adequately reflect variations in NO production within the trigeminovascular system itself. Changes in nNOS activity in non-adrenergic, non-cholinergic (NANC) fibres supplying cerebral blood vessels might have been obscured. Indeed, several studies suggest a relationship between NO and the phenomenon of neurogenic inflammation in the trigeminovascular system, which appears to be a key step in the development of neurovascular headaches (50). Neurogenic inflammation is characterised by the release of various vasoactive peptides, including calcitonin gene-related peptide (CGRP), from trigeminal perivascular nerve endings and results in vasodilation of the cranial blood vessels and sensitisation of perivascular sensory afferents. The latter leads to increased transmission of nociceptive information to the brainstem. While the link between the production of NO and the release of CGRP is controversial, CGRP and NOS do seem to co-exist in trigeminal ganglion cells (51,52). In addition, nNOS appears to co-ordinate NO production to provoke CGRP release and vasodilation at the level of the trigeminovascular system (19). As nNOS involvement might have been missed by the peripheral sampling, it should still be considered as a potential therapeutic target in the treatment of migraine. Second, the L-arginine-NO pathway is assessed during a headache-free period. In the 14 patients who developed a migraine headache, no data are available concerning the biomarkers associated with NO production as the headache occurred only 6–24 h after L-arginine or placebo infusion. Third, the search for end-products of NO furnishes inconsistent results, mainly because of a broad range of inter-individual variation. This is partly due to dietary habits and, therefore, a nitrite/nitrate-restricted diet was imposed on all participants. Nevertheless, differences in physical activity between migraine patients and healthy volunteers might also have introduced bias (53,54). Last, the evidence for the involvement of NO in the pathophysiology of migraine remains strong (1,55). This, however, does not imply that there should be an overproduction of NO in migraineurs, as the relation between migraine and NO might be due to hypersensitivity to NO.
Conclusions
The results of the present study do not support the idea of a generalised increase in NOS activity in migraine patients outside of a migraine attack. In combination with the results of recently conducted clinical trials with potent iNOS inhibitors, which turned out to be ineffective, this study favours the involvement of nNOS in the pathogenesis of migraine above iNOS and eNOS. Therefore, nNOS remains a potentially valid target in the treatment of migraine. The smaller increase in plasma L-citrulline, urinary nitrite/nitrate and cGMP excretion following L-arginine infusion in migraine patients might indicate dysfunction of eNOS in migraine patients.
Footnotes
Acknowledgements
The authors gratefully acknowledge Jo Van Effen, Marc Oeyen, Godelieve Jansen and Karin Vaes for their practical work during the study and Sonia Demarsin for her help with the bio-analysis. This work was supported by grants from the Research Foundation-Flanders (F.W.O.–Vlaanderen) and GSK.
Appendix 1
CONSORT flow diagram.
References
1.
OlesenJThomsenLLLassenLHOlesenIJ. The nitric oxide hypothesis of migraine and other vascular headaches. Cephalalgia1995; 15: 94–100.
2.
IversenHOlesenJTfelt-HansenP. Intravenous nitroglycerin as an experimental model of vascular headache. Basic characteristics. Pain1989; 38: 17–24.
3.
KrabbeAAOlesenJ. Headache provocation by continuous intravenous infusion of histamine. Clinical results and receptor mechanisms. Pain1980; 8: 253–259.
LassenLHAshinaMChristiansenIUlrichVOlesenJ. Nitric oxide synthase inhibition in migraine. Lancet1997; 349: 401–402.
6.
SarchielliPAlbertiACodiniMFloridiAGallaiV. Nitric oxide metabolites, prostaglandins and trigeminal vasoactive peptides in internal jugular vein blood during spontaneous migraine attacks. Cephalalgia2000; 20: 907–918.
7.
D’AmicoDFerrarisALeoneM. Increased plasma nitrites in migraine and cluster headache patients in interictal period: basal hyperactivity of L-arginine-NO pathway?Cephalalgia2002; 22: 33–36.
8.
NatteroGMengozziGInconisTParadisiL. Nitric oxide, endothelin-1, and transcranial Doppler in migraine. Findings in interictal conditions and during migraine attack. Headache1996; 36: 307–311.
9.
StepienAChalimoniukM. Level of nitric oxide-dependent cGMP in patients with migraine. Cephalalgia1998; 18: 631–634.
10.
Van der SchuerenBJLunnonMWLaurijssensB. Does the unfavourable pharmacokinetic and pharmacodynamic profile of the iNOS inhibitor GW273629 lead to inefficacy in acute migraine?J Clin Pharmacol2009; 49: 281–290.
11.
OhshimaHFriesenMBrouetIBartschH. Nitrotyrosine as a new marker for endogenous nitrosation and nitration of proteins. Food Chem Toxicol1990; 28: 647–652.
PalmerJEGuillardFLLaurijssensBEWentzALDixonRMWilliamsPM. A randomised, single-blind, placebo-controlled, adpative clinical trialof GW274150, a selective iNOS inhibitor, in the treatment of acute migraine. Cephalagia2009; 29: 124–124.
14.
HoyeKLaurijssensBEHarnischLO. Efficacy and tolerability of the iNOS inhibitor GW274150 administered up to 120 mg daily for twelve weeks in the prohylactic treatment of migraine. Cephalagia2009; 29: 132–132.
15.
PalmerRMFerrigeAGMoncadaS. Nitric oxide release accounts for the biological activity of endothelium-derived relaxing factor. Nature1987; 327: 524–526.
16.
YunHYDawsonVLDawsonTM. Neurobiology of nitric oxide. Crit Rev Neurobiol1996; 10: 291–316.
17.
DohrnCSMullettMAPriceRHBeitzAJ. Distribution of nitric oxide synthase-immunoreactive interneurons in the spinal trigeminal nucleus. J Comp Neurol1994; 346: 449–460.
18.
LinQPalecekJPaleckovaV. Nitric oxide mediates the central sensitization of primate spinothalamic tract neurons. J Neurophysiol1999; 81: 1075–1085.
19.
AkermanSWilliamsonDJKaubeHGoadsbyPJ. Nitric oxide synthase inhibitors can antagonize neurogenic and calcitonin gene-related peptide induced dilation of dural meningeal vessels. Br J Pharmacol2002; 137: 62–68.
20.
HoskinKLBulmerDCGoadsbyPJ. Fos expression in the trigeminocervical complex of the cat after stimulation of the superior sagittal sinus is reduced by L-NAME. Neurosci Lett1999; 266: 173–176.
21.
MehtaSStewartDJLevyRD. The hypotensive effect of L-arginine is associated with increased expired nitric oxide in humans. Chest1996; 109: 1550–1555.
22.
SchwedhelmEMaasRFreeseR. Pharmacokinetic and pharmacodynamic properties of oral L-citrulline and L-arginine: impact on nitric oxide metabolism. Br J Clin Pharmacol2008; 65: 51–59.
23.
Headache Classification Subcommittee of the International Headache Society. The International Classification of Headache Disorders, 2nd edn. Cephalalgia2004; 24(Suppl 1): 1–160.
24.
StewartWFLiptonRBWhyteJ. An international study to assess reliability of the Migraine Disability Assessment (MIDAS) score. Neurology1999; 53: 988–994.
25.
El AssaadMATopouchianJAAsmarRG. Evaluation of two devices for self-measurement of blood pressure according to the international protocol: the Omron M5-I and the Omron 705IT. Blood Press Monit2003; 8: 127–133.
26.
American Thoracic Society. Recommendations for standardized procedures for the on-line and off-line measurement of exhaled lower respiratory nitric oxide and nasal nitric oxide in adults and children-1999. This official statement of the American Thoracic Society was adopted by the ATS Board of Directors, July 1999. Am J Respir Crit Care Med1999; 160: 2104–2117.
27.
ChaceDHKalasTANaylorEW. Use of tandem mass spectrometry for multianalyte screening of dried blood specimens from newborns. Clin Chem2003; 49: 1797–1817.
28.
LangoucheLVanhorebeekIVlasselaersD. Intensive insulin therapy protects the endothelium of critically ill patients. J Clin Invest2005; 115: 2277–2286.
29.
Bode-BogerSMBogerRHSchroderEPFrolichJC. Exercise increases systemic nitric oxide production in men. J Cardiovasc Risk1994; 1: 173–178.
30.
BogerRHBode-BogerSMThieleWJunkerWAlexanderKFrolichJC. Biochemical evidence for impaired nitric oxide synthesis in patients with peripheral arterial occlusive disease. Circulation1997; 95: 2068–2074.
31.
BogerRHBode-BogerSMGereckeUGutzkiFMTsikasDFrolichJC. Urinary NO3-excretion as an indicator of nitric oxide formation in vivo during oral administration of L-arginine or L-NAME in rats. Clin Exp Pharmacol Physiol1996; 23: 11–15.
32.
RashidPAWhitehurstALawsonNBathPM. Plasma nitric oxide (nitrate/nitrite) levels in acute stroke and their relationship with severity and outcome. J Stroke Cerebrovasc Dis2003; 12: 82–87.
33.
MylesPSChanMTKayeDM. Effect of nitrous oxide anesthesia on plasma homocysteine and endothelial function. Anesthesiology2008; 109: 657–663.
34.
AppenzellerO. Pathogenesis of migraine. Med Clin North Am1991; 75: 763–789.
35.
GabrielliMSantarelliLAddoloratoG. High prevalence of antiendothelial cell antibodies in migraine. Headache2002; 42: 385–386.
36.
TietjenGEAl-QasmiMMAthanasKDaferRMKhuderSA. Increased von Willebrand factor in migraine. Neurology2001; 57: 334–336.
37.
VanmolkotFHVan BortelLMde HoonJN. Altered arterial function in migraine of recent onset. Neurology2007; 68: 1563–1570.
38.
de HoonJNSmitsPTroostJStruijker-BoudierHAVan BortelLM. Forearm vascular response to nitric oxide and calcitonin gene-related peptide: comparison between migraine patients and control subjects. Cephalalgia2006; 26: 56–63.
39.
ThomsenLLDaugaardDIversenHOlesenJ. Normal radial artery dilation during reactive hyperaemia in migraine without aura. Endothelium1996; 4: 199–206.
BartleyJFergussonWMoodyAWellsAUKolbeJ. Normal adult values, diurnal variation, and repeatability of nasal nitric oxide measurement. Am J Rhinol1999; 13: 401–405.
42.
DillonWCHamplVShultzPJRubinsJBArcherSL. Origins of breath nitric oxide in humans. Chest1996; 110: 930–938.
43.
SartoriCLeporiMBuschT. Exhaled nitric oxide does not provide a marker of vascular endothelial function in healthy humans. Am J Respir Crit Care Med1999; 160: 879–882.
StewartTEValenzaFRibeiroSP. Increased nitric oxide in exhaled gas as an early marker of lung inflammation in a model of sepsis. Am J Respir Crit Care Med1995; 151: 713–718.
46.
WilkinsonIAHallidayJAHenryRLHankinRGHensleyMJ. Headache and asthma. J Paediatr Child Health1994; 30: 253–256.
47.
AamodtAHStovnerLJLanghammerAHagenKZwartJA. Is headache related to asthma, hay fever, and chronic bronchitis? The Head-HUNT Study. Headache2007; 47: 204–212.
48.
MedianaJLDiamondS. Migraine and atopy. Headache1976; 15: 271–273.
49.
ScheleRAhlborgBEkbomK. Physical characteristics and allergic history in young men with migraine and other headaches. Headache1978; 18: 80–86.
50.
MoskowitzMA. The neurobiology of vascular head pain. Ann Neurol1984; 16: 157–168.
51.
HughesSRBrainSD. Nitric oxide-dependent release of vasodilator quantities of calcitonin gene-related peptide from capsaicin-sensitive nerves in rabbit skin. Br J Pharmacol1994; 111: 425–430.
52.
EdvinssonLMulderHGoadsbyPJUddmanR. Calcitonin gene-related peptide and nitric oxide in the trigeminal ganglion: cerebral vasodilatation from trigeminal nerve stimulation involves mainly calcitonin gene-related peptide. J Auton Nerv Syst1998; 70: 15–22.
53.
ScherAITerwindtGMPicavetHSVerschurenWMFerrariMDLaunerLJ. Cardiovascular risk factors and migraine: the GEM population-based study. Neurology2005; 64: 614–620.
54.
Rodriguez-PlazaLGAlfieriABCubedduLX. Urinary excretion of nitric oxide metabolites in runners, sedentary individuals and patients with coronary artery disease: effects of 42 km marathon, 15 km race and a cardiac rehabilitation program. J Cardiovasc Risk1997; 4: 367–372.
55.
LassenLHAshinaMChristiansenIUlrichVOlesenJ. Nitric oxide synthase inhibition in migraine. Lancet1997; 349: 401–402.