
Abstract
The aim of this study was to estimate the prevalence of primary headaches in pre-adolescent children, as well as headache frequency and days of treatment in this population. Sample consisted of 1994 children (aged 5–12 years). Parents were interviewed by a paediatric headache specialist using a questionnaire that allowed the classification of headaches using the criteria of the Second Edition of the International Classification of Headache Disorders. The most severe headache type was classified (mutually-exclusive diagnoses). Prevalence and prevalence ratios were calculated overall, as well as by age, gender and race. The overall prevalence of migraine was 3.76%, non-significantly higher in boys (3.9%) than in girls (3.6%). Prevalence of probable migraine was significantly higher than the prevalence of migraine for all ages (overall prevalence of 17.1%). Chronic migraine (CM) happened in 0.8% (girls, 1.15%; boys, 0.5%). Infrequent episodic tension-type headache (ETTH) happened in 2.3% of the sample while prevalence of frequent ETTH was 1.6%. Probable TTH happened in 13.5%. Most children with migraine had consulted a medical doctor because of their headaches, and the proportion was higher among children with CM (93.7%). Prevalence of primary headaches is high in young children. Probable diagnoses are more common than full diagnoses. Consultation rates are elevated.
Introduction
Although primary recurrent headaches are common at all ages, the effects of age on their prevalence may be dramatic (1,2). Taking migraine as an example, before puberty, prevalence is slightly higher in boys than in girls; as adolescence approaches, incidence and prevalence increase more rapidly in girls than in boys. The prevalence increases throughout childhood and early adult life until approximately 40 years of age, declining thereafter (3,4). The age influence on prevalence is also seen for other primary headaches, including tension-type headache (TTH) (5,6) and chronic daily headaches (CDH) (7–9).
Age not only influences headache prevalence, but also phenotype and clinical presentation. For migraine, it has been demonstrated that the ratio between probable migraine (PM) and migraine decreases with age, suggesting that full-blown migraine is more common in adolescence and adulthood than in childhood (10). Similarly, the presentation of CDH differs considerably when comparing adolescents and adults; chronic TTH and new daily persistent headache are relatively more common in adolescents, while chronic migraine (CM) responds to a higher proportion of adult CDHs. Furthermore, adolescents with CDH are less likely to overuse acute medications than adults, suggesting that individuals with the early onset form of the disease, may be at increased biological risk (7).
Studying the prevalence of headaches at age extremes is relevant. Paediatric studies provide information about determinants of incident disease; elderly studies report on the long-term consequences of headaches, as well determinants of headache remission.
Studies on the epidemiology of primary headaches in adolescents have been published (9,11). For younger children, studies either focused on migraine or TTH without distinguishing subtypes (5,11–14), or did not use the Second Edition of the International Classification of Headache Disorders criteria (15).
Accordingly, herein, we conducted a population study to estimate the prevalence of primary headaches in childhood. We also aimed to describe the headache frequency and days of treatment within this population.
Subjects and methods
Overview
This study was conducted as part of a large ongoing population study aiming to investigate the mental health of children and adolescents in Brazil (Attention-Brazil Project) (16). Target sample consisted of all children from 5–12 years registered in the public school system of a city (Santa Cruz das Palmeiras, SP, Brazil). Direct interviews were made with the parents, and children were examined (see details below) in February 2009.
Geographic characterisation and target sample
According to the demographic census, the studied region covers an area with 32,862 inhabitants (year 2008). Of these, 30,387 (92.4%) are in the urban area. Life expectancy is 73.71 years, and fecundity rate is 2.13, rates that are similar to the overall Brazilian rates (17).
Our target sample consisted of children from 5–12 years, registered in any of the five public elementary school of the city (n = 2173); children registered in the middle school were not included in this study. Both children from urban and rural areas were assessed, as long as they were enrolled in the school system (which is mandatory). Therefore, although all children younger than 11 years were targeted, only a subsample of those aged 11 and 12 years were included.
Of the target sample, consent was obtained from 1994 (91.0%), and analysable data (complete demographic and headache information), from 1906 (87% of target sample and 95% of respondents).
Interviews
The overall aim of this study was to assess the prevalence of learning disabilities at childhood, as well as to diagnose other conditions that may influence learning (including pain). To establish the headache status, parents were interviewed (97.3% mothers), and children were examined (to exclude secondary disorders). Parental interview was made by a paediatric headache specialist with over 20 years experience (MAA), using a questionnaire that captured the ICHD-2 criteria. Children were examined to exclude secondary disorders by the same headache specialists. Accordingly, we followed the gold standard procedure for paediatric headache diagnosis, interviews with the parents (note that, as stated below, median age of our sample was 7 years), and physical examination, using standardised criteria (ICHD-2).
In addition to capturing distinguishing headache features, we also asked about behaviours related to pain. The questionnaire followed the ICHD-2 classification criteria for primary headaches, but also assessed headache frequency over the past month and year, and other headache parameters (15).
Headache diagnosis
Based on the response to the questionnaires, headache diagnoses were assigned strictly following the ICHD-2 (15). Children with migraine fulfilled all the criteria proposed for migraine, while probable migraine was assigned when children fulfilled all but one criterion for migraine and did not fulfil full criteria for any other headache syndrome (15). Chronic migraine was classified based on the appendix criteria to the ICHD-2 (18). Similarly, tension-type headache (TTH) was subdivided into infrequent episodic TTH (<1 headache day per month), frequent episodic TTH (1–14 days of headache per month), and chronic (CTTH, 15 or more days of headache per month). Probable TTH fulfilled all but one criterion for TTH and did not fulfil criteria for other primary headaches. Diagnoses were mutually exclusive, and classification was made based on response for most severe headache type.
Analyses
Sex-specific prevalence estimates of primary headaches (1-year period prevalence) were derived by age. To characterise the sample, descriptive statistics were performed. To represent the relationship between sociodemographic characteristics and migraine status, cross tabulations were performed. Crude and adjusted prevalence ratios were obtained using binary regression model. Relative risk and 95% confidence intervals (CIs) compared specific categories (e.g. age categories or race) with the reference category. The level of significance adopted was 5%. Statistical analysis was performed with the aid of the SPSS v.15.0 for Windows (SPSS Inc.; Chicago, IL, USA).
This study and surveys received full approval from a Human Research Committee (School of Medicine at Sao Jose do Rio Preto, State University of Sao Paulo, Brazil). The study design and aims were discussed with the children and parents. Written informed consent (approved by the Human Research Committee) was obtained from all the parents (legal guardians).
Results
Characteristics of the sample
Of 2173 children, our participant sample consisted of 1994 (91.7%) children from 5–12 years old, registered in one of five public elementary schools. Of the children, 955 (47.9%) were girls (58.7% white), while 1039 (52.1%) were boys (56.2% white). Of these, complete information on the children’s headache was obtained from 907 girls (94.9%) and 999 boys (96.2%), for a total rate of 95.5%.
Demographic distribution of the sample and response rates

Prevalence of primary headaches
Prevalence of migraine subtypes in pre-adolescent children

Non-stated cases are not displayed.
Prevalence of PM was significantly higher than the prevalence of migraine for all ages. Overall, prevalence was 17.1% (ranging from 14.2% at the age of 6 years to 20.7% at the age of 9 years). Prevalence was significantly increased in girls than in boys (18.7% vs 15.4%; RR, 1.21; 95% CI, 1.0–1.5). Prevalence did not vary significantly by race.
The vast majority of cases of PM failed to receive a migraine diagnosis based on missing the duration criteria (had untreated headaches lasting less than 1 h, 76%). The second reason for a PM diagnosis was due to missing the associated symptoms criteria (having only one of photophobia or phonophobia and no nausea or vomiting).
Pooling migraine and PM together, prevalence of episodic headaches with migraine features was 20.8% (22.3% in girls and 19.4% in boys).
CM happened in 0.8% of the sample, and prevalence was non-significantly different in girls and boys (1.1% vs 0.5%) or in non-whites and whites (1.2% vs 0.6%).
Prevalence of tension-type headache in pre-adolescent children

Non-stated cases are not displayed.
As seen with migraine (PM was more prevalent than full blown migraine), probable TTH was also more prevalent than ETTH (13.5%, 13.0% in girls and 14.0% in boys). Pooling ETTH and probable TTH together, prevalence was 17.4%, being 17.0% in girls and 17.7% in boys. CTTH was rare, being diagnosed in only one case of our sample (0.05%) and, therefore, is not represented in Table 3.
The 1-year prevalence for chronic daily headaches was 1.68%. Prevalence in girls was 2.1%, versus 1.3% in boys (non-significant differences). When dichotomising age, neither overall nor gender-stratified prevalences were statistically different in children younger than 9 years old versus 9 years or older.
Frequency of headaches, use of acute medications and medical consultation
Most children with migraine had consulted a medical doctor because of their headaches, and the proportion was higher among children with CM (93.7%). Conversely, only a minority of children with TTH had ever consulted a medical doctor for headache reasons (Figure 1).
Proportion of preadolescent children who sought medical care because of their headaches, stratified by the headache diagnosis (over life time).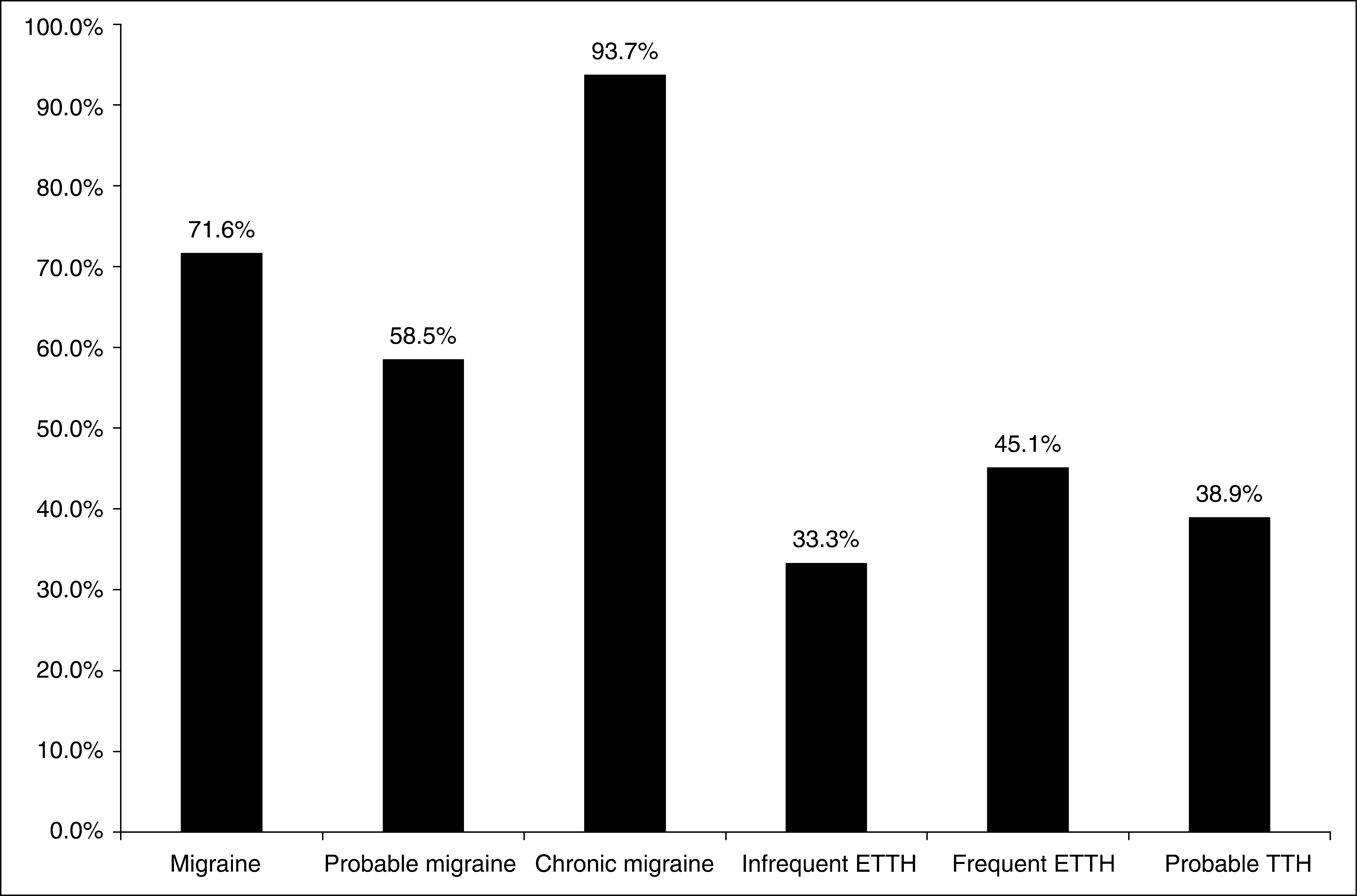
Figure 2 displays the number of days using any acute treatment in the past month as a function of headache frequency, among children with migraine subtypes. Of interest is the fact that, for all subtypes, most children used acute medication at least one day; 42.7% of the children with migraine used acute medication on 2–4 days, and over 8% used it on 5 or more days; only 12.5% of the children with CM used medication on more than 10 days.
Frequency of use of acute medication as a function of the migraine subtype (over 1 month).
Figure 3 presents equivalent data for TTH. The vast majority of children with infrequent ETTH have not used medication over the past month, and most with frequent ETTH used it only once.
Frequency of use of acute medication as a function of the tension-type headache subtype (over 1 month).
Discussion
Several studies have assessed the epidemiology of primary headaches in the paediatric population (5,11–13,19) but, to the best of our knowledge, studies assessing the prevalence of headaches at childhood using the ICHD-2 criteria have not been conducted. Although the ICHD-2 maintained the basic structure of the ICHD-1 (20), several changes were placed (15). For migraine, changes included the introduction of criteria for CM, as well as re-naming what was previously known as migrainous headache as PM. For TTH, the most important modification was subdividing the episodic TTHs into infrequent (<1 headache day per month) and frequent (1–14 days per month), as well as the introduction of criteria for probable TTH.
Prevalence of migraine in our study was 3.7%, and the classical female and white increased prevalence was not seen in our sample (1). In the classical study of Bille (11,13) in school children, prevalence of migraine was 1.4% at the age of 7 years (2.9% in our study) and gradually increased with age, although at rates lower than ours. Other studies in slightly older samples found prevalence rates higher than ours (5,21). Methodological differences, as well as different genetic backgrounds likely explain these differences. Nonetheless, by all standards, the prevalence of migraine in young children is not small. Of interest, however, is the fact that the prevalence of PM was significantly higher than the prevalence of migraine; indeed, 17% of the children had headaches fulfilling criteria for PM. In a study conducted in a health plan, around 14% of the adults had migraine, and another 15% had PM (10), suggesting that PM is prevalent at all ages (22). However, while most adults with PM fail to be classified as having migraine because they lack one necessary associated symptom (23), we found that the vast majority of children with PM received this diagnosis because of the short duration of their attacks. Since in children, the ICHD-2 criteria require attacks lasting at least 1 h (4 h in adults), this means that a sizable proportion of children have what otherwise would be a migraine, but lasting minutes rather than hours or days. Future studies should focus on this subgroup in order to subsidise the maintenance or modification of the migraine duration criterion for paediatric migraines at the ICHD-3.
CM happened in 0.8% of our sample. Comparable results from the population are missing, since criteria for CM were not available before the ICHD-2. It is well established that CM responds for a large proportion of children with CDH presenting to tertiary care (9,24–26). The prevalence of overall CDH in adolescents is around 2% (27). Populational (25) and clinic-based (28) studies also suggest that early onset of CDH is associated with poorer outcomes, and that CDH in adolescents is less frequently associated with excessive use of medication (7,19,24), a finding supported by our study. Since early onset of CDH may reflect a stronger biological predisposition (28), our findings are of interest and we plan to use the cases identified herein to establish a CM cohort in order to conduct longitudinal studies.
Episodic TTH happened in 3.9% of our sample and most had infrequent TTH. The prevalence is lower than that reported by others, but this information should be taken with caution. We diagnosed the most severe headache reported by the children, following several other studies (3,29). That means that children with migraine and TTH were probably classified as having migraine only. Accordingly, the prevalence reported by ourselves should be interpreted as the proportion of children with TTH but not migraine. Interestingly, the prevalence of CTTH was very low, and the prevalence of probable TTH was higher than the prevalence of full-blown TTH.
Most children with migraine participating in our study had been seen by a doctor, and figures are considerably higher than what has been reported in adults (2,29–33). It can be speculated that early onset of migraine inspires fear in the parents, triggering medical consultations. Typical migraine features (since rates were higher in migraine than PM) and headache frequency (consultation rates were higher in CM than in migraine) are associated with higher rates of consultation. On the other hand, a minority of children with TTH had been seen by a provider, suggesting that it is not the presence of headache per se that triggers consultations in children, but the migraine features.
Finally, a sizable proportion of children with migraine used acute medication more than once a month, and 39% used it more than twice, demonstrating that migraine and subtypes are not only common, but also burden a subgroup of children. Paediatricians need to be aware of the relevance of primary headaches and need to be adequately trained in the diagnosis and treatment of these common conditions.
Study limitations
Our study has limitations. First, we identified children registered in the public school system. Although this is a well-established method to investigate the epidemiology of diseases in the paediatric population (12,13), since education is mandatory in most countries, children from higher socio-economic strata are less likely to study in the public school system, and adjustments would not perfectly address this topic. More importantly, we did not differentiate migraine between with or without aura. Because of the age of our population, we felt that it would be difficult to differentiate aura from photophobia in the younger children, and this procedure has been adopted by others (13). We plan to explore this issue further in subsequent studies. Third, as shown below, we likely underestimated the prevalence of the TTHs, since we only classified the most severe type of headache presented by patients. Again, this is justifiable, since young children may not be capable of providing information on more than one type of headache, and will likely focus on the most severe or frequent forms. Furthermore, the criteria of the ICHD-2 recommend that paediatric migraine lasting less than 1 h (without treatment) should be confirmed by headache calendars, and this was not conducted by ourselves. Finally, we have not collected information about menarche and, by not doing so, we missed the opportunity of contrasting, for specific ages, the prevalence of headaches in girls as a function of their pubertal age.
Conclusions
The prevalence of primary headaches is significantly high in young children. Probable diagnoses are more common than full diagnoses. Consultation rates are elevated, suggesting that paediatric headache inspires fear in the parents.