
Abstract
The aim of this study was to measure quality of life (QOL) across a broad age range of paediatric migraine patients. Children and adolescents (n = 686) with migraine completed the Pediatric Quality of Life Inventory, version 4.0 (PedsQL 4.0) and a standardized headache assessment at an initial clinic visit. The sample size for each PedsQL age group was: age 2-4 = 21, age 5-7 = 86, age 8-12 = 298, and age 13-18 = 281. Mean total score was 72.7 ± 14.8, significantly less than healthy norms (P < 0.01). Teens reported lower School Functioning than older and young children (P < 0.05) and young children reported lower Social Functioning than older children and teens (P < 0.001). A moderate relation was found between self and parent report. Age-related effects on QOL have implications for the evaluation and management of migraine in paediatric practice. The self and parent report forms of the PedsQL can be used in a practice setting.
Introduction
Health-related quality of life (QOL) is an emerging area of clinical research with a direct impact on patient adherence, patient satisfaction, and treatment effectiveness (1). QOL is a multidimensional construct that reflects the interplay between disease and patient's subjective evaluation of his or her physical, social, and emotional functioning (2). Several studies have examined the impact of recurrent headache on the QOL of adult patients (3, 4). For the most part, these studies have found that adults with migraine report lower physical and emotional functioning and greater impairment at work and in social activities than adults without headache or with other chronic disorders (3). However, despite the fact that up to 11% of children between the ages of 5 and 15 years and 28% of adolescents between the ages of 15 and 19 years may have migraine (5, 6), QOL is only an emerging area of research in these age ranges (7). A central reason for this research deficit is the lack of appropriate and practical measures of QOL that can be applied to the broad age range in which migraine occurs (8).
The assessment of QOL in children is difficult, since measures must consider children's changing cognitive and social development. In addition, there is the question of who should provide the information, the parent or the child. The Pediatric Quality of Life Inventory, version 4.0 (PedsQL 4.0) is a valid, developmentally appropriate measure of QOL for children between the ages of 2 and 18 years (8). The instrument is a general measure of QOL and has two forms, a child report form and a parent-proxy form. It has been used for assessment of QOL in children and adolescents with cancer, rheumatoid disease, diabetes mellitus, and orthopaedic conditions (9). Children's QOL is significantly affected by disease when compared with healthy normative children. Knowledge of the specific ways in which disease can impact QOL can have a direct effect on the recognition and development of clinical and educational programmes for children with these illnesses (7, 8).
While there is little research examining QOL of children and adolescents with migraine, the few studies available have found individuals with headache to report lower physical and emotional well-being as a result of their disorder (10–14). The majority of these studies have focused on adolescents. An objective measure of childhood migraine disability, Pediatric Migraine Disability Assessment (PedMIDAS), identified that many children and adolescents (ages 4–18) experience moderate to severe impairment in school, home, and play activities due to their headaches (15). Research that includes data from a large clinical sample of children and adolescents (ages 2–18) and their parents is needed to assess the impact of headache on daily activities (e.g. school, social functioning) as well as on physical and emotional functioning (i.e. QOL).
The aim of this study was to characterize age-related effects of migraine using a reliable, valid, and developmentally appropriate general measure of QOL. The impact on QOL in a large clinical sample of children and adolescents with migraine was compared with the QOL of a healthy, normative sample. It was expected that children and adolescents with migraine and their parents would report lower QOL than healthy, normative individuals and their parents as evidenced by lower PedsQL 4.0 scores. Within the sample of children and adolescents with migraine, developmental differences in QOL were tested. Specifically, it was expected that older children and adolescents would report lower QOL than young children. Finally, it was expected that the concordance between child/adolescent self report and parent-proxy report of QOL would be moderate, with each perspective adding unique information about the impact of migraine.
Methods
Procedure
Patients were evaluated at the Headache Center at Cincinnati Children's Hospital. At the initial appointment, families completed detailed questionnaires concerning the features of their child's headache, their child's general health status, and an age-appropriate version of the PedsQL 4.0. PedsQL 4.0 responses were collected from both parents and children for patients between the ages of 5 and 18 years. Only parents completed the study questionnaires for children between the ages of 2 and 4 years. A thorough history and neurological examination were performed to establish a clinical diagnosis and a diagnosis using the International Headache Society (IHS) criteria (16).
Measures
The Headache Center intake questionnaire includes a self-report measure which asks patients to indicate the severity of their headache using a 10-point scale (10 = most severe pain), duration of their headache, and the frequency as the average number of headache days per month over the past 3 months. PedsQL 4.0 (17) is a brief 23-item measure that evaluates QOL in four areas of functioning: physical functioning (eight items), emotional functioning (five items), social functioning (five items), and school functioning (five items). The PedsQL 4.0 has four age ranges: toddlers (2–4 years), young child (5–7 years), child (8–12 years), and adolescents (13–18 years). Parent-only report is obtained for toddlers (2–4 years). The PedsQL 4.0 asks respondents to indicate how much of a problem each item has been during the past month. For the child self report (8–18 years) and the parent report forms, respondents use a 5-point Likert scale to rate the item severity (0 = never a problem; 1 = almost never a problem; 2 = sometimes a problem; 3 = often a problem; 4 = almost always a problem). For the younger children (5–7 years), a simplified 3-point Likert scale, anchored with a happy and a sad face, is used (0 = not at all a problem; 2 = sometimes a problem; 4 = a lot of a problem) to increase further the developmental sensitivity of the measure. In this study, children and adolescents were assisted by a paediatric psychologist, if needed, to complete the measure successfully. Parents and children/adolescents independently completed the PedsQL across the age range.
The PedsQL 4.0 yields a total QOL score and two summary scores: Physical Health Summary Score and Psychosocial Health Summary Score. To obtain scores, items are reversed scored, transformed to a 0–100 scale (0 = 100, 1 = 75, 2 = 50, 3 = 25, 4 = 0), and averaged – total scores near 0 indicate lower QOL while scores approaching 100 indicate higher QOL. To obtain the Physical Health Summary Score, the Physical Health Subscale is used (eight items) and a mean score is computed. To calculate the Psychosocial Health Summary Score, items in the Emotional, Social, and School Functioning subscales (15 items) are used and a mean score is computed. Individual subscale scores are calculated for each of the four areas of functioning by calculating mean scores for each subscale.
Prior research with the PedsQL 4.0 demonstrated good internal consistency (α child = 0.88, α parent = 0.90) in healthy children and children with acute or chronic illnesses and headache (9, 14). Construct validity for the measure was established through known-group comparisons, which revealed expected differences in the QOL of healthy children vs. children with acute or chronic illnesses. An additional measure of validity was provided through correlations between QOL scores and criterion variables such as the number of days that the child needed medical care and the number of days missed from school or work due to the child's illness. Finally, factor analyses revealed a factor solution that was consistent with the a priori conceptually derived hypotheses set by the scale developer (9).
PedsQL 4.0 has been described as one of the three available general measures of QOL in childhood and adolescence with adequate psychometric properties for application in clinical research (8). Of the other two measures, one does not offer a child-report format and the second has too many items for efficient use in a clinic setting. A headache-specific measure of QOL has not yet been developed that spans the entire age range used in this study. Since this study focused on comparing QOL across disease and non-disease groups, and across age within the disease group, PedsQL 4.0 was uniquely suited for the purpose.
Results
Demographics and headache parameters
This study evaluated 686 children and adolescents (391 girls and 295 boys) consecutively seen in the Headache Center at Cincinnati Children's Hospital Medical Center. The sample size for each PedsQL 4.0 age group was: age 2–4 = 21, age 5–7 = 86, age 8–12 = 298, and age 13–18 = 281. Eighty-six percent of participants met the IHS criteria for migraine or migraine with aura, while every child and adolescent was clinically diagnosed with migraine. Those who met the definition of clinical migraine included individuals with IHS migraine or migraine with aura and individuals whose symptoms were consistent with the IHS diagnosis except the duration criterion. This difference reflects the sensitivity of the IHS criteria among children (6, 18, 19). Forty percent of children had ≥ 15 headache days per month (e.g. chronic daily headaches; (20)). For the total sample, mean age at study enrolment was 11.4 ± 3.6 years. The mean age of onset for headache was 8.1 ± 3.6 years. The racial distribution of children and adolescents was: 88% Caucasian, 11% African-American, and 1% other. The mean migraine frequency was 13.3 ± 10.4 per month. The mean severity of migraine was 6.7 ± 1.8 on a scale of 0–10 with increasing severity. The mean duration of a typical migraine was 9.6 ± 16.0 h.
Table 1 presents demographic and headache characteristics for each of the age groups examined in this study. Frequency and duration of migraine appear to increase across the age groups, whereas intensity was similar across the groups. The gender ratio was near 1 : 1 except for the teen-age group (13–18 years) where 73% of the subjects were female. As for headache diagnosis/type, the percentage of individuals meeting IHS criteria was similar for each age group, except toddlers (age 2–4 years) who met the criteria less often (probably due to the duration requirement of IHS diagnosis). There was a pattern of greater frequency of chronic daily headache (CDH) as the groups advanced in age. Each of these findings is consistent with our current understanding of headache and migraine across different age groups of children and adolescents (21).
Demographic information and headache parameters by age group
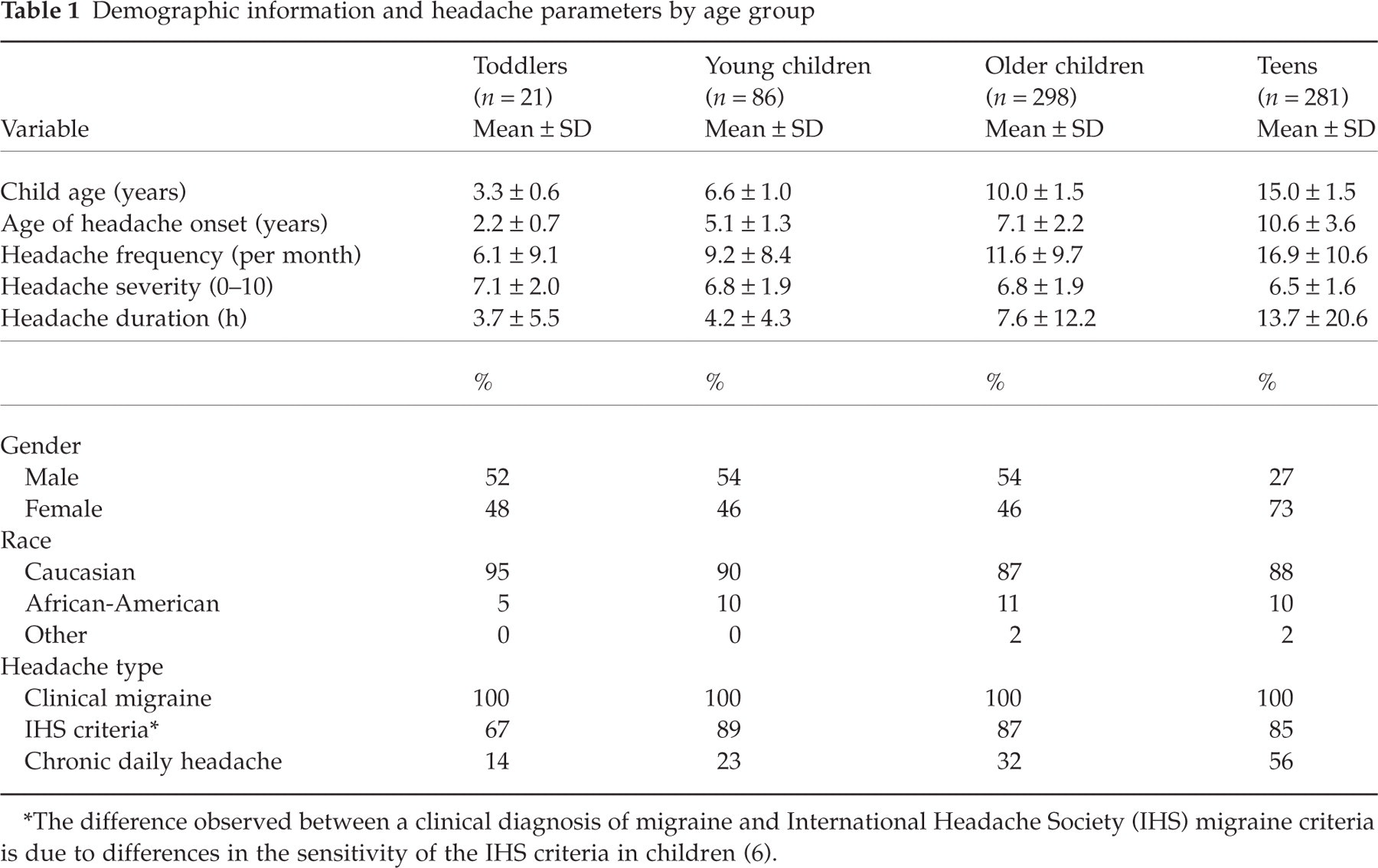
∗The difference observed between a clinical diagnosis of migraine and International Headache Society (IHS) migraine criteria is due to differences in the sensitivity of the IHS criteria in children (6).
Descriptive statistics and reliability
Table 2 presents means and standard deviations by each self-report subscale of the PedsQL 4.0 for the total migraine sample and for each age group. Healthy children population scores across all age groups are presented in Table 2 as well (9). These scores are based upon normative values from prior published data and are not based upon a contemporary, matched sample of healthy children. Parallel descriptive data are presented for parent-report scales in Table 3. Both child/adolescent self-report and parent-report scales met the minimum reliability standard of 0.70 for group comparisons across subscales and age (22). Descriptive and reliability data for headache subtype (i.e. clinical migraine diagnosis, IHS migraine, and CDH) for child/adolescent self-report and parent-report scales, specific to each age group, are available from the authors.
Descriptive statistics for PedsQL 4.0 child self-report for healthy and migraine children/adolescents for all ages and across age groups for migraine sample

∗Healthy children population scores across all ages from Varni, Seid, & Kurtain, 2001.
Descriptive statistics for PedsQL 4.0 parent report for healthy and migraine children/adolescents for all ages and across age groups for migraine sample

∗Healthy children population scores across all ages from Varni, Seid, & Kurtain, 2001.
Comparisons with healthy children and adolescents
Based on previous literature, it was predicted that the total sample of children and adolescents with migraine would report lower QOL than healthy control children and adolescents. Consistent with this hypothesis, one-sample t-tests revealed that children/adolescents with migraine reported significantly lower QOL than healthy children/adolescent norms (P < 0.001) across subscales and total scores. Parent report of QOL for children/adolescents in the migraine group was also significantly lower than parent report norms (P < 0.001) across subscales and total scores. A Bonferroni correction was applied to analyses comparing QOL in healthy individuals with children/adolescents with IHS migraine and CDH. Across parent and child report, significant differences (P < 0.001) remained for both groups of children/adolescents with headache vs. healthy children/adolescents.
Age group comparisons for children and adolescents with migraine
Table 4 presents the relation of total self-report PedsQL 4.0 score to the headache parameters of frequency, duration, and severity for each age group. Pearson product–moment correlation coefficients were determined and the results indicated weak relationships regardless of age group. The most consistent association was between higher quality of life and less frequent migraine.
Correlations between total PedsQL 4.0 scores and headache parameters by age group

∗P < 0.05
∗∗P < 0.01.
Multivariate analysis of variance (MANOVA) tests were conducted to determine differences between age groups within the sample of migraine patients for both parent and child/adolescent report. Because older children typically are involved in several school and extracurricular activities, it was predicted that children (ages 8–12 years) and adolescents (ages 13–18 years) would report lower QOL scores than young children (ages 5–7 years).
Results of these analyses on the self-report scales demonstrated a main effect for child age [F (6, 650) = 5.40, P < 0.001], with specific differences found for the Social Functioning [F (2, 653) = 8.58, P < 0.001] and School Functioning [F (2, 653) = 6.96, P < 0.001] subscales. Post hoc analyses revealed differences between the young child (5–7 years) and child (8–12 years) age groups (P < 0.01), and between the young child and adolescent (13–18 years) age groups (P < 0.001) on the Social Functioning subscale, with young children reporting lower QOL than both children and adolescents. Differences were also observed between the young child and adolescent age groups (P < 0.01), and between the child and adolescent age groups (P < 0.001) on the School Functioning subscale, with adolescents reporting lower QOL than both children and young children.
Results of MANOVA tests on the parent report scales also revealed a main effect for child age [F (6, 650) = 2.36, P < 0.01]. For these analyses, differences were found for the Physical Functioning [F (2, 654) = 5.21, P < 0.01] and School Functioning [F (2, 654) = 4.26, P < 0.05] subscales and total scores [F (2, 654) = 3.59, P < 0.05]. Post hoc analyses demonstrated differences between the child and adolescent age groups (P < 0.001) on the Physical Functioning subscale, with parents of adolescents reporting lower scores than parents of children. Differences were also observed between the young child and adolescent age groups (P < 0.01), and between the child and adolescent age groups (P < 0.05) on the School Functioning subscale, with parents of adolescents reporting lower scores than parents of both children and young children. Finally, there was a difference between the child and adolescent age groups (P < 0.01) on the total score, with parents of adolescents reporting lower scores than parents of children.
Parent and child/adolescent response concordance
Bivariate correlation analyses were conducted to examine the relation between parent and child/adolescent responses on the PedsQL 4.0. Table 5 presents the correlation matrix for total sample data across subscales for migraine. Overall, parent-report and self-report correlations ranged from 0.65 to 0.77, suggesting a moderate degree of concordance between parents and children/adolescents.
Bivariate correlations between PedsQL 4.0 subscales

Child self-report coefficients appear below the diagonal; parent-report coefficients appear above the diagonal; Child–parent coefficients appear on the diagonal in parentheses.
∗P < 0.01.
Discussion
Migraine is a common problem for children and adolescents. However, despite the prevalence of this disorder, the evaluation of QOL in children and adolescents with migraine is only beginning to emerge as an area of research. This is in stark contrast to the amount of research that has been conducted on the burden of migraine on the functioning and QOL in adults (4). To assess patients’ QOL, researchers have developed both general and disease-specific measures of QOL. Disease-specific measures of QOL have the advantage of including items that are appropriate for patients with a specific disease or condition. These measures can offer a more precise estimate of areas of impairment that may be unique to a specific chronic illness. In contrast, general measures of QOL offer the opportunity to assess QOL across disease populations and in healthy normative samples, which can allow for a more comprehensive evaluation of QOL with appropriate comparison groups (14). The PedsQL 4.0 offers researchers interested in evaluating the QOL of paediatric patients the only valid, general measure of QOL which can be easily administered to children/adolescents and parents within a clinic setting and across a broad age range (8). A headache-specific measure of QOL with these attributes has yet to be developed.
Findings of this study revealed that the PedsQL 4.0 is a reliable measure of QOL in children and adolescents with migraine. It met the minimum standards for internal consistency for both the child/adolescent report and parent-proxy report forms. In addition, the degree of concordance between child/adolescent and parent report suggests adequate interrater reliability. However, the correlations between child/adolescent and parent ratings were moderate in strength, suggesting some variation in their perspectives. From a research standpoint, these moderate correlations highlight the importance of gathering the perspectives of both parents and children/adolescents when measuring a subjective construct, such as QOL (8).
There are also clinical implications for these findings. Specifically, for individuals from age 2 to 18 years, these findings suggest the importance of teaching and empowering children and adolescents to communicate with others about their headache pain. In addition to asking children and adolescents to provide information about the characteristics of their headaches, it is crucial to understand their perceptions of the impact of the headaches on their lives, their goals for management of the headaches, and their perspectives on how they can be actively involved in treating their headaches. As is the case with adults with headaches (23), this communication is essential for determining the appropriate diagnosis and treatment of headache as well as ensuring effective administration of interventions and assessment of outcomes. Both children/adolescents and their families provide important and unique information for the evaluation and management of paediatric migraine.
A comparison of the QOL of children and adolescents with migraine with norms for healthy children and adolescents demonstrated impaired QOL in all areas of functioning. Similar findings were obtained when comparing parents’ perceptions of children/adolescents’ QOL for parents of individuals with migraine and norms for parents of healthy children and adolescents. These results are consistent with reported literature, which also found lower physical, social, emotional, and school functioning in children and adolescents with headache (10–12, 14). Moreover, these findings are similar to results of a study which used an objective measure of disability and found that children and adolescents with migraine may experience moderate to severe impairment in school, home, and play activities due to their headaches (15). In the PedMIDAS study, researchers measured disability according to the number of full days missed from school and/or the number of days that children functioned at less than half of their ability at school, home, or during play activities due to migraine. Future research will need to examine the relationship between contextual measures of functioning, such as the PedMIDAS, and subjective evaluations of functioning, like the PedsQL 4.0, to understand the full impact of migraine on the functioning of children/adolescents and families.
Cross-sectional comparisons within the migraine sample found differences in functional impairment across age groups. Adolescents (ages 13–18 years) reported more impairment in School Functioning than children (ages 8–12 years) and young children (ages 5–7 years). Parents similarly viewed differences in this area of functioning. In contrast, young children reported more impairment in Social Functioning than children and adolescents. Parents did not view such a difference. Parents viewed adolescents as more impacted by migraine in the areas of physical functioning and overall QOL than children aged 8–12, whereas these differences were not present based upon self report. As this is the first report to examine age-related effects on QOL in children and adolescents with migraine, additional research is needed to replicate these findings and to understand better the possible determinants of age-related effects on specific areas of QOL.
There were weak associations between QOL and headache parameters across the age groups. However, in future research these findings will need to be replicated with more methodologically sophisticated measures such as prospective, daily headache diaries or retrospective report over the same 1-month period used for the PedsQL 4.0 assessment. The current data suggest the importance of measuring both headache characteristics such as frequency and duration and the impact of headaches on functioning with general (e.g. PedsQL 4.0) and disease-specific (e.g. PedMIDAS) instruments in clinical practice and research. Exclusively assessing headache features and change in headache parameters over time (regardless of the specific method of measurement) does not provide a comprehensive evaluation of a child's or adolescent's headache experience. Prior research has demonstrated that both general (i.e. PedsQL 4.0) and disease-specific (i.e. PedsMIDAS) instruments add to the comprehensive evaluation of treatment outcome in paediatric migraine and could be used in longitudinal studies focused on the epidemiology of headache disorders in children and adolescents (14, 15). An additional implication of these relations is the importance of research to determine models that better explain how and why certain children and adolescents with similar headache features do better than others in the domains of physical, emotional, social, and school functioning (1, 7, 24, 25).
This sample of children and adolescents is representative of the population seen at the Cincinnati Children's Headache Center and the Cincinnati metropolitan area. However, research with other samples (e.g. community, paediatric primary care, across multiple paediatric headache centres) is needed to demonstrate the generalizability of these findings. PedsQL 4.0 used both child/adolescent report and parent report with good interrater reliability. Self- and other report methods are vulnerable to subject bias, so objective measures of the impact of headache on children/adolescent's daily life and prospective measures of headache parameters (e.g. daily headache diaries) should be added in future investigations. While the PedsQL 4.0 is a valid and practical tool for examining QOL in children/adolescents and families within a busy clinic setting, it does not provide a complete assessment of the many specific psychosocial variables that comprise the QOL construct, or include a reliable, disease-specific module for paediatric headache (8). Thus, variables such as family functioning, depression, and social support would be better assessed through multiple measures, and disease-specific questions regarding QOL applicable across the age range of the PedsQL 4.0 need to be developed and examined for psychometric integrity. PedsQL 4.0, however, does demonstrate that migraine significantly impairs QOL across a broad age range of children and adolescents, emphasizing the importance of early, appropriate recognition and treatment.
Footnotes
Acknowledgements
We thank the following individuals for their assistance with data management: Molly L. Heidemann, Anna-Liisa Vockell, Susan LeCates, and Ann Segers. We also thank the children, adolescents, and parents who participated in this project.