
Abstract
The aim of this study was to evaluate the impact of gender and age on headache characteristics and disability. Headache characteristics were assessed at an initial visit to a paediatric specialty care centre and five follow-up visits. A total number of 4121 patients were evaluated. Fifty-eight per cent of the sample was female. Boys were younger at their first headache and initial visit. They more frequently described headache pain as squeezing and location as top of the head. Girls reported more frequent and longer headaches. Girls more often described headache pain as sharp and location as back of the head. Age accounted for more variance than gender in headache severity, duration, frequency and disability. Gender differences exist in headache characteristics. Age is also an important factor in the variability in characteristics and disability. Longitudinal studies are needed to describe further the natural history of headaches in childhood and compare outcome between genders.
Introduction
Headache is one of the most common disorders in childhood, with an estimated 75% reporting a significant headache by age 15 years (1). Of school-aged children and adolescents, 10–15% report headaches that result in significant functional impairment. Although many families seek treatment for headaches each year, the characteristics of these children have not been adequately described in the literature.
Several studies have reported the prevalence of headache in childhood and found that headache occurrence increases as children approach adolescence. The prevalence of migraine headache has been reported as 1–3% in preschoolers, 4–11% in school-aged children and 8–23% in adolescents (2). Boys with migraine outnumber girls with migraine before age 7 years, and are equally likely as girls to have headaches between the ages of 8 and 11 years. Girls have a greater incidence of headaches in adolescence (3).
Headaches can have a large impact on the daily lives of children and parents. These children frequently miss school, social activities and activities with their families (4). In addition, they may be at a heightened risk of developing additional physical problems in adulthood as well as mental difficulties such as anxiety and depression (4).
Although researchers have reported information on the characteristics of children with headaches, the variability of these characteristics and the subsequent identification of subgroups of patients may allow for individualization of treatment in children with headaches. The current study extends this research and provides additional information on gender differences in the headache characteristics reported by children seen in a subspecialty headache clinic.
Methods
All patients attending a paediatric multidisciplinary Headache Center were given the Cincinnati Children's Headache Center Questionnaire at their initial and follow-up evaluations (5). These questionnaires were completed by parent and child together and the responses validated with the child in a semistructured interview. Variables included in the questionnaire were headache frequency, duration, severity, location, pain quality, associated symptoms and headache disability using PedMIDAS (6). PedMIDAS is a paediatric-specific disability tool that analyses the impact of headaches on a child's school, home and social activities. Patients' demographic information including age, race and gender was also collected. Questionnaire information was then entered into an electronic database. Questionnaires and database entry had been approved by the local Institutional Review Board.
A retrospective analysis of the data was completed for all patients who completed the questionnaires between January 1998 and October 2007. Differences between average age of onset, age of presentation, severity, duration and frequency were evaluated by gender using two-sample t-tests. A multiple regression was conducted to determine effects of age and gender on dependent variables severity, duration and frequency. Furthermore, pain location, headache features, associated symptoms, and disability were assessed for gender differences using a P-value significance level of 0.01 using a χ2 test.
Results
Demographics
Data were assessed for 4121 patients (mean age 11.76 ± 3.64 years, range 1–21 years), both as a whole and then separated by gender. There were 2383 female (mean age 12.54 ± 3.59 years), and 1738 male patients (mean age 10.69 ± 3.43 years) with 57.8% of the sample being female. The sample was predominantly White (82.5%), with 11.7% African-American, and < 6% comprising Asian, Hispanic, Middle Eastern and other races.
Headache onset The mean age of headache onset was 8.48 ± 3.72 years for the entire sample. When evaluated by gender, boys reported an earlier mean age of onset (t = 16.09, P < 0.01) of 7.43 ± 3.41 years, and girls reported a mean age of headache onset of 9.26 ± 3.74 years.
Headache presentation
The mean age of presentation for the sample was 11.76 ± 3.64 years. In a similar pattern (t = 16.64, P < 0.01), boys presented younger (mean age 10.69 ± 3.43 years) than girls (mean age 12.54 ± 3.59 years). The mean difference between estimated age of onset and age of presentation for boys was 3.28 ± 2.86 years, whereas for girls it was 3.26 ± 2.95 years. This difference was not statistically different (t = 0.20, P = 0.84).
Headache characteristics
Severity
Headache severity was similar between the groups (t = 0.35, P = 0.73). Girls reported a mean severity of 6.61 ± 1.76, and boys a mean severity of 6.63 ± 1.93. The effects of age and gender on headache severity were assessed using a multiple regression model. On the first step, age was entered into the model for headache severity. It was significantly correlated with headache severity. Older children perceived their headaches as being less severe (r =−0.053). On the second step, age and gender were entered simultaneously and did not result in a significant increase in ΔR 2. Age accounted for 0.6% of the variance (R 2 = 0.006, P < 0.01), whereas including gender had no significant effect (R 2 = 0.000, P = 0.629) on the variance of headache severity in the sample. Overall, the model that included age and gender was significantly greater than zero and provided the best fit, F 3,3785 = 7.86, P < 0.001.
Duration
Girls reported longer average headache duration of 11.31 ± 16.34 h and boys an average duration of 8.1 ± 13.43 h (t = 6.75, P < 0.01). To assess headache duration using a multiple regression model, age was first entered into the model and was significantly correlated with headache duration. As children aged they reported increased headache duration (r = 0.18). On the second step, age and gender were entered simultaneously and did not result in a significant increase in ΔR 2. Age accounted for 3.3% of the variance in headache duration (R 2 = 0.033, P < 0.01), and including gender accounted for an additional 0.4% of the variance. The full model R 2 that included age and gender was significantly greater than zero and provided the best fit, F 3,3765 = 47.41, P < 0.001.
Frequency
Girls also reported a higher frequency (15.88 ± 10.73 headaches per month) than boys (11.39 ± 9.99 headaches per month) (t = 13.65, P < 0.01). To evaluate the effects of age and gender on headache frequency, age was first entered into the model and was significantly correlated with headache frequency. Older children reported greater headache frequency than did younger children (r = 0.29). On the second step, age and gender were entered simultaneously and did not result in a significant increase in ΔR 2. Age accounted for 8.4% of the variance (R 2 = 0.084, P < 0.01) and gender accounted for an additional 1.9% of the variance (R 2 = 0.019, P < 0.01) in headache frequency within the sample. The full model R 2 with age and gender included was significantly greater than zero, F 3,3958 = 151.50, P < 0.001.
Headache pain, location and associated symptoms
There were several differences in reported headache location, pain quality and associated symptoms. Girls reported that their headache location was frontal, temporal, and in the back of the head. They also described headache pain as throbbing, pressure, constant and sharp. Associated symptoms included photophobia, phonophobia, nausea and light-headedness. Boys reported that their headache location was frontal, temporal, and on the top of the head. Boys described headache pain as throbbing, pressure, constant and squeezing. Their associated symptoms were mostly reported as photophobia, phonophobia, nausea, vomiting, and confusion or difficulty in thinking. Headache characteristic differences between boys and girls are reported in Table 1.
Headache features by gender
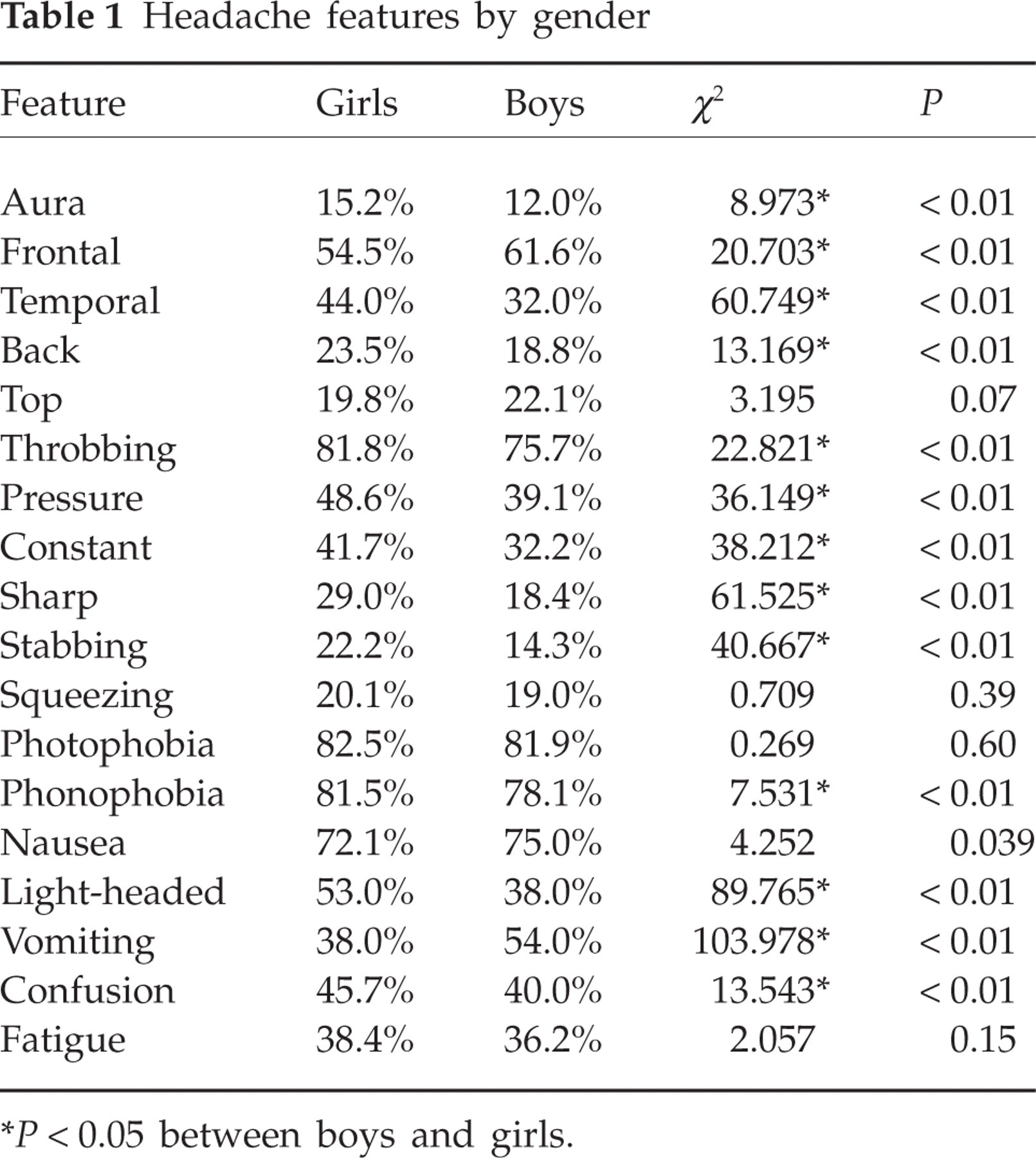
∗ P < 0.05 between boys and girls.
Headache disability
Girls reported higher levels of disability than boys in both PedMIDAS score and number of school days missed. Girls reported a significantly higher average PedMIDAS of 44.77 ± 50.57 compared with boys (32.13 ± 38.65) (t = 8.72; P < 0.01). On average, girls reported missing 4.46 ± 7.8 days of school within a 3-month period, whereas boys missed 3.75 ± 7.21 days of school (t = 2.97; P < 0.05).
The effects of age and gender on headache disability were assessed using a multiple regression model. On the first step, age was entered into the model for headache disability. It was significantly correlated with headache disability. The older a child was at the initial visit, the higher the PedMIDAS score, meaning that older children were more disabled. On the second step, age and gender were entered simultaneously and it also resulted in a significant increase in ΔR 2. Age accounted for 5.8% of the variance (R 2 = 0.058, P < 0.01), whereas including gender had a significant effect (R 2 = 0.006, P < 0.01) on the variance of headache disability scores in the sample. Overall, the model that included age and gender was significantly greater than zero and provided the best fit, F 2,3032 = 102.78, P < 0.001.
The average PedMIDAS score and change in PedMIDAS score were assessed for up to five follow-up appointments. Girls reported significantly higher average PedMIDAS scores than boys at the first three visits to the Headache Center. Girls reported an average PedMIDAS of 44.77 ± 50.57 at their initial appointment, 24.5 ± 37.53 at their first follow-up, 18.51 ± 29.61 at their second follow-up and 16.22 ± 28.26 at their third follow-up appointment. Boys reported an average PedMIDAS of 32.13 ± 38.65 at their initial visit, 16.51 ± 26.72 at their first follow-up appointment, 14.13 ± 24.07 at their second follow-up and 13.43 ± 19.02 at their third follow-up appointment. Once patients returned for a fourth or fifth follow-up visit, both boys and girls reported similar PedMIDAS scores. Girls reported an average PedMIDAS of 15.84 ± 24.96 at their fourth follow-up appointment and 14.45 ± 24.51 at their fifth follow-up appointment. Boys reported an average PedMIDAS of 17.33 ± 38.09 at their fourth follow-up appointment and 13.72 ± 21.15 at their fifth follow-up appointment. Additional information on disability can be seen in Table 2.
Change in disability

Headache diagnoses
Using International Classification of Headache Disorders, 2nd edn criteria (7), the majority of patients had a diagnosis of migraine (n = 3753, 91.1%), with most of these being either migraine without aura (n = 3209, 77.94%) or migraine with aura (n = 412, 10.0%). In addition, 583 (14%) had headaches sufficiently frequent to be classified as chronic migraine. Using a clinical diagnosis, 97.3% had a diagnosis of migraine, with 83.2% having migraine without aura, 11.4% migraine with aura and 14.8% chronic migraine. Non-primary headaches were seen in only 65 patients (1.6%), with the majority of these being post-traumatic (1.1%). Multiple diagnoses were allowed, so the total was > 100%.
Discussion
The current study suggests that there are gender differences in paediatric headache presentation, headache characteristics and functional disability. The onset and presentation to a tertiary headache clinic were influenced by age and gender. In preadolescence (< 13 years old), more boys than girls presented for treatment (boys 29.4% vs. girls 25.6%), whereas more adolescent girls than adolescent boys presented for headache treatment (boys 12.7% vs. girls 32.3%). This result supports previous research that has documented a developmental pattern to gender differences in headache onset and age at presentation for treatment (8). The variation in presentation mirrors the progression of migraine to a female predominance in adolescents. The observation that boys present in greater numbers with earlier onset also suggests that in the preadolescent period there are biological or sociological factors that increase the risk of migraine in boys, which shifts as children enter adolescence.
Developmental differences also emerged when the influence of age and gender on the report of headache severity, frequency and duration was explored. Age accounted for a significant amount of variance in headache severity, frequency and duration. Gender did not account for additional variance in scores when age and gender were entered into the model together, suggesting that age and not gender accounts for differences in this sample's headache severity. This implies that boys and girls of the same age perceive the severity of their headaches equally, but that as children age they perceive their headaches as less severe.
When evaluated together, both age and gender accounted for significant variability in headache duration and frequency scores. Age, however, was a larger determining factor than gender in headache duration and frequency. These results indicate that there is a developmental component to headache pain that may need to be considered when children present to a physician for treatment. In particular, pubertal development may play a part in gender differences in headache occurrence.
The study also found several gender differences in the use of headache descriptors. Overall, girls and boys used many of the same words to describe their headache location and pain. They used headache descriptors such as frontal, temporal, throbbing and pressure, and top (location) at a comparable frequency. However, girls most often described their headache location as back and characterized pain as sharp, whereas boys most often described their headache location as top and described pain as squeezing.
Furthermore, girls in this sample reported greater functional disability associated with headaches than did boys. Girls also reported missing more days of school because of headaches than did boys. This implies that headaches in girls have a greater impact, which may be a combined influence of frequency and duration, but not severity, as severity varied with age and not gender. Thus, gender alone could be considered a marker of response to treatment.
Gender differences in functional disability were significant at the initial medical visit and first three follow-up appointments, with girls remaining more disabled. These differences in disability were not significant at fourth and fifth follow-up visits, suggesting that girls and boys may respond equally well to medical treatment and no longer experience significant headache disability.
Future research should focus on the extent to which pubertal changes, such as menstruation, account for gender differences in headaches during adolescence. Being aware of these changes and their impact on paediatric headache's outcome may influence treatment choices. Based on the observations of this study, gender appears to be a positive marker of outcome in boys, especially as regards disability due to headaches. Furthermore, understanding the biological, psychological and sociological factors that underlie these gender and age differences may help identify biomarkers that can identify which children are most likely to develop headaches and present to a specialty clinic for treatment.