
Abstract
This was a questionnaire survey on headache and migraine prevalence in 2873 Singaporean schoolchildren aged 6 to 16 years. ICHD-II headache classification, disability assessment with PedMIDAS and screening of psychosocial co-morbidities with the Paediatric Symptom Checklist were conducted. Lifetime headache prevalence was high at 80.6%, migraine prevalence was 8.6% and tension headache prevalence was 10.0%. Headache and migraine prevalence was high compared with that found in other Asian studies. Factors significantly associated with headache included adolescent age (OR = 1.5 [95% CI 1.3–1.9], p < .001), female gender at primary (OR = 1.4 [95% CI 1.1–1.8], p = .003) and secondary (OR = 1.8 [95% CI 1.3–2.5], p < .001) levels and Malay ethnicity at the primary level (OR = 2.8 [95% CI 1.6–4.9], p < .001). The average PedMIDAS score for headache disability was 3.2 ± 8.4, and migraine disability (PedMIDAS 8.1 ± 11.2–15.2 ± 29.6) was lower than in some studies. Self-medication (20.5%) and use of alternative therapy (59.0%) were high among chronic daily headache sufferers. Routine sleep and stress screening is recommended for children with headaches. Recognition of the influence of genetics, lifestyle and cultural factors on headache management should be emphasized.
Keywords
Introduction
Headaches are common in children, although the problem may be under-diagnosed. Many adult studies have supported lower migraine prevalence in Asians than in Caucasian or African communities (1,2), including a study in our local community (3). Published studies of paediatric headache and migraine in Asians are limited, though these have mostly been done in ethnically homogenous populations. These studies demonstrated lower migraine prevalence (0.5%–14%) (4–8) when compared with findings from urbanized countries such as the United States, the United Kingdom and Europe (6.3%–21.3%) (9–13). These studies on headaches in children, however, varied in the demographics, methodology, age and criteria of children enrolled, and not all have adopted similar migraine definitions.
Singapore represents an urban but ethnically diverse Asian country, with Chinese (75.2%), Malay (10.8%), Indian (5.3%) and other ethnic groups, including Caucasians (2.8%). Though culturally diverse, all children undergo rigorous academic training from ages 6 to 16, before entering pre-university. The stress among schoolchildren due to the relentless pursuit of academic excellence is a common discussion theme among parents and the media, supported by some local reports (14). Sleep deprivation among local schoolchildren has also been a concern among health professionals. The Asia-Pacific Paediatric Sleep Alliance global survey (unpublished) revealed that local schoolchildren sleep at least an hour later than their Western counterparts, with a higher percentage of local parents (45%) versus Western parents (28%) demonstrating concerns about this issue. Psychosocial stressors and sleep have been known to factor importantly in headache occurrence (15). Additionally, a local study among adults revealed that 11.1% of a cohort of headache patients sought treatment from traditional practitioners (16). Ethnic beliefs and practices—for example, attitudes to pain as a spiritual virtue among Malays (17), and the use of acupuncture and traditional Chinese medicine (TCM) among Chinese—may also affect health-seeking behaviours and treatment in the population, especially in relation to disabling headaches (e.g. migraine) and chronic daily headaches.
This study was undertaken to determine the prevalence of headache and migraine in our population, with the hypothesis that, similar to that of adults in Singapore, migraine prevalence among our children is low despite the lifestyle influences of stress and sleep patterns. Screening for psychosocial co-morbidities, stress, sleep deprivation and headache disability was also performed, with analyses of ethnic differences. The prevalence and treatment modalities in children and adolescents with chronic daily headaches were also determined, specifically focusing on their risks of self-management and seeking of alternative therapies.
Methods
Sampling and headache classification
School-aged children were enrolled for the study from nine primary and eight secondary schools, randomly selected from the northern, southern, eastern and western parts of the country over a period of two years (2005 to 2006). As the population density and ethnic distribution was fairly similar throughout the country, this sample allowed as fair as possible a representation of the true population. The sampling age was 6 to 12 years for the primary schoolchildren, and 13 to 16 years for the secondary school adolescents. The school sampling register and approval for the study were provided by the Ministry of Education, Singapore. Ethics approval for this study was also provided by the Institutional Review Board. These schools represented a mixed population of boys and girls, and mixed ethnicity. Two boys-only schools and two girls-only schools were also randomly selected in each category of primary and secondary schools. We excluded religious schools and international schools, which tended to enrol students of particular ethnic and cultural backgrounds, which would not reflect the true population ethnic distribution. Random sampling of class register numbers from classes at all levels was performed, with each matched to a study participant. Questionnaires, along with an explanatory letter and parental consent forms, were distributed by the teachers, and student anonymity was maintained to the research assistant who collected the completed questionnaires. To reduce non-participation and non-response, surveys were timed to avoid school examinations and start of term, which were busy periods. For every school, two trips were made by the research assistant to ensure collection of all questionnaires.
Parents assisted children with the questionnaires if the children were in primary school. Those in secondary schools filled in the questionnaires without parental supervision. Students were asked ‘Have you ever had headaches?’. Those who answered positively were asked further questions on what their headaches were usually like, with information collected on headache location, characteristics, frequency and associated symptoms, according to the headache classification criteria of the International Headache Society, 2004 (International Classification of Headache Disorders, Second Edition [ICHD-II]) (18). This meant that the modified paediatric migraine criterion, with headache duration of 1–72 hours and bilateral location of headaches, was adopted. Though ICHD-II mentions that migraine headaches of less than two hours require corroboration with headache diaries, this study had to be less restrictive in the duration criteria to avoid underestimating migraine prevalence in the community setting. The questionnaire had been validated in a pilot study among children in our centre, with clinical interviews and physical examination, and using similar migraine criteria (unpublished but presented as abstract).
Headaches were classified as primary types (migrainous or tension-type headache [TTH]) if they fulfilled the characteristics, and assigned probable migraine or TTH criteria as far as possible, if short of one criteria. No physical examination was conducted, but questions covering possible secondary causes were provided as a checklist. Pictures related to headache location (19) and the Wong-Baker pain faces scale (20) were used to assist in accurately locating headaches and to determine the severity of headaches. Aura symptoms for migraine were explained in simple language. The phrases ‘flickering lights, loss or blurring of vision, spots and lines’ were used for visual aura symptoms, ‘pins and needles or numbness’ for sensory symptoms, and ‘difficulties in talking’ for dysphasic speech disturbances. Onset, temporal features and duration of aura symptoms were established and motor weakness was excluded. Headache treatment was also determined, which included information on complementary and alternative medicines (CAM) such as acupuncture and TCM.
Headache disability, psychosocial co-morbidities and sleep
Headache and migraine disability was determined using the Pediatric Migraine Disability Assessment (PedMIDAS), which is an adapted Migraine Disability Assessment (MIDAS) questionnaire for children and adolescents (21). All children were administered the questionnaire regardless of whether they eventually received a migraine diagnosis (22). The Paediatric Symptom Checklist (PSC) (23), which is a validated, one-page questionnaire listing a broad range of emotional, cognitive and behavioural problems in children, was also administered. Two versions were used: the parent-completed version (PSC) for younger children, and the youth self-report version (Y-PSC) for children 11 years old and above. A score based on each item in the questionnaire was compiled, and cut-off scores of PSC scores ≥28, and Y-PSC scores ≥30 were considered significant, indicating high risks of psychosocial dysfunction. Separately, five screening questions were asked about stress at home and in school. Three simple questions related to sleeping late, waking up feeling tired and average sleep duration were also included.
Chronic daily headaches
Children were classified as having chronic daily headache (CDH) if they had headaches daily or almost daily for more than 15 days/month for more than three months (24). In this study, there were limitations on sub-classification of CDH under the new ICHD-II to chronic migraine (CM) and chronic tension-type headache (CTTH). Instead, the terms ‘chronic with migraine features’ or ‘chronic with tension headache features’ were used, as questionnaires cannot effectively exclude medication overuse through determination of headache improvements with stopping medications (18). Similarly, within the limitations of a questionnaire, ‘new daily persistent headache’ with rapid development of unremitting headaches could not be confirmed with certainty without a thorough clinical history. Lastly, the questionnaires could not confirm ptosis or miosis, or establish headache response to indomethacin specifically, hence excluding children with ‘hemicrania continua’. As these were very rare forms of CDH, children were not further sub-classified according to these two diagnoses.
Data analysis
To increase accuracy in headache classification, independent coding agreements for each questionnaire were obtained by the investigator and three other medically trained research assistants. Statistical analyses were performed using SPSS for Windows (Version 15.0; SPSS. Chicago, IL). Descriptive statistics for categorical variables were presented as N (%) and mean (standard deviation [SD]) for quantitative variables. Analyses were performed separately for the primary and secondary levels, the former group referred to as ‘children’ and the latter as ‘adolescents’. Logistic regression analysis was performed to determine the unadjusted and adjusted (race, gender and education level) odds ratios. Statistical significance was set at p < .05.
Results
Headache prevalence and classification
Among 3840 children invited to participate, 1725/2465 (70.0%) from primary schools and 1148/1375 (83.5%) from secondary schools returned questionnaires, with valid consent and complete data. This represented a general response rate of 2873/3840 (74.8%). Among responders, 1286 were boys and 1587 were girls. Ethnic distribution was similar to that in the population (81.1% Chinese, 10.8% Malay, 5.3% Indian, 2.8% Caucasian and other). The remaining students chose not to respond, or handed in questionnaires which were invalid by any of the following criteria: incomplete parent or subject consent; missing sections on headache descriptions, PSC, PedMIDAS, medications and treatment; or nonsense answers on any of these parts.
Headache prevalence in primary and secondary students, with subgroup analysis and adjusted odds ratio for ethnicity and gender

OR = odds ratio. CI = confidence interval.
Migraine prevalence was 8.6% (247), consisting of migraine without aura (MO) in 167 (5.8%) students, and migraine with aura (MA) in 80 students (2.8%) (Table 2). Migraine prevalence was 7.9% in boys and 9.2% in girls, and was higher in secondary students (11.9%) than in primary school students (6.4%), with gradual increases from childhood to adolescence (Figure 1). By adolescence, migraine was 1.2 times more likely in girls. If the criterion for minimum migraine duration was changed to two hours instead of one hour, 117 students (4.1%) would still have MO, and 63 (2.2%) would have MA, for a total migraine prevalence of 6.3% (180 students). TTH was present in 287 (10.0%) of students. Among them, frequent episodic headaches (FTHs) were present in 125 (4.4%) and infrequent episodic headaches (ITHs) were present in 162 (5.6%); the latter were more likely to be present in secondary than primary schoolchildren (OR = 2.1 [95% CI 1.5–2.9], p < .001), and boys than girls (OR = 1.6 [95% CI 1.1–2.2], p = .006).
Headache and migraine prevalence in boys and girls according to age: Headache prevalence in boys = 76.8%; headache prevalence in girls = 83.6%. Migraine prevalence in boys = 7.9%; migraine prevalence in girls = 9.2%. Headache prevalence, disability and Paediatric Symptom Checklist scores according to headache subtype PedMIDAS = Pediatric Migraine Disability Assessment. SD = standard deviation. Question items relating to stress and sleep among headache sufferers with significant versus non-significant PSC scores PSC = Paediatric Symptom Checklist. CI = confidence interval. aAdjusted for gender, race and educational level.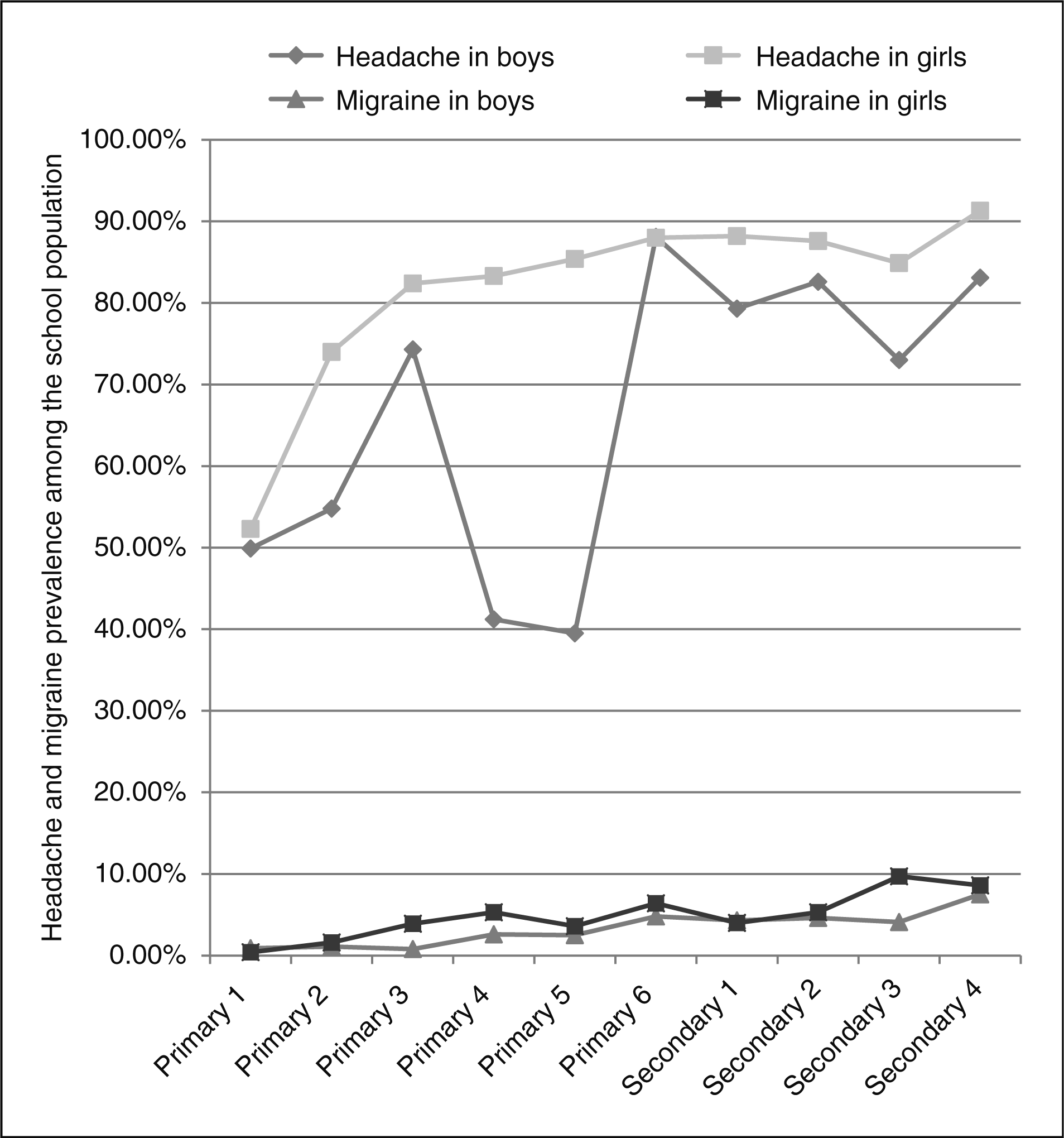


Five hundred and sixty-two students (19.6%) had probable TTH (Table 2). Among them, a significant proportion (79.6%) did not fulfil sufficient episodes for diagnosis. Probable migraine was present in 363 (12.6%) of individuals. Among 132 (4.6%) of the cohort who met criteria for both probable migraine without aura (PMO) and TTH, PMO was assigned to avoid under-appreciating the prevalence of these headaches, which have been demonstrated in studies to have disabilities and health impact (25,26). In 856 (29.8%) of students, headaches were unclassified (U). The proportion of unclassified headaches fell in the transition from primary (40.4%) to secondary (32.0%) school. Among headache sufferers in secondary school (N = 970) compared to primary school (N = 1345), more were able to receive a diagnosis of either migraine (14.2% vs. 8.2%) or TTH (15.2% vs. 10.5%).
Major headache subtypes according to ethnic groups, educational level and gender
Among primary schoolchildren, Malays were more predisposed to headaches than other ethnic groups (OR = 2.8 [95% CI 1.6–4.9], p <.001) (Table 1). Malay (OR = 4.6 [95% CI 2.0–11.0], p < .001) and Indian (OR = 4.1 [95% CI 1.1–14.9], p = .03) schoolgirls at the primary level were also more predisposed to migraine with aura MA than Chinese schoolgirls at this level.
Among secondary schoolchildren, Malay secondary schoolboys (OR = 4.9 [95% CI 1.8–13.2], p = .002) and girls (OR = 6.7 [95% CI 2.6–17.1], p < .001) were also more predisposed to MA than Indians or Chinese. No ethnic differences were found for chronic daily headaches and unclassified headaches.
Migraine disability and psychosocial co-morbidities
The burden of headache reflected by PedMIDAS scores was an average of 3.2 ± 8.4, which according to the grading scale of disability was classified as ‘little to none’ (PedMIDAS 0–10). The proportion of children with moderate-to-severe disability (PedMIDAS ≥ 31) was highest for MA (Table 2). PedMIDAS scores were higher for adolescents (3.9 ± 10.5) than for younger children (2.7 ± 6.5) (p < .001), and were significantly greater for CDH sufferers (10.0 ± 14.5) than for non–CDH sufferers (2.6 ± 7.4) (p < .001), with no difference in the scores between boys (3.1 ± 9.7) and girls (3.2 ± 7.0) (p = .783). Adjusting for gender and educational level, there were also no ethnic differences in PedMIDAS among headache (p = .21) and migraine patients (p = .25).
The proportion of children reaching significant scores on the PSC was highest for MA (48.8%) and PMA (36.0%) (Table 2). Among those without headaches, only 7.6% were found to have significant PSC scores on this screen. Thus, a positive score was more likely to be encountered in subjects having headache (any subtype), compared with those without headaches (p < .001). In addition, CDH sufferers (49.5%) received more significant PSC scores than non–CDH sufferers (15.4%) (p < .001), as did children in secondary schools (OR = 1.3 [95% CI 1.1–13], p = .003) versus those in primary schools. There were no ethnic differences in significant PSC scores among headache (p = .39) and migraine patients (p = .37). Significant PSC scores among headache sufferers predicted children who answered positively to questions about stress at home and in school, as well as sleeping late, feeling tired and suffering from lack of sleep (p < .001) (Table 3).
Chronic daily headaches and treatment
Chronic daily headaches (CDHs) were present in 204 (7.1%) of the study cohort: 58/204 (28.4%) fulfilled criteria for ‘chronic with migraine features’ and 45/204 (22.1%) ‘chronic with tension headache features’. Among the remaining 49.5%, headaches were unclassifiable or had features matching ‘probable tension headaches or probable migraine’ due to shortage of descriptive criteria. Adolescents were more likely to suffer from CDH (OR = 1.4 [95% CI 1.0–1.8], p = .037). No gender or ethnic group had a predilection for CDH. Treatment modalities revealed a high proportion self-medicating or not being treated, and a significant proportion using CAM (Figure 2). Migraine patients, on the contrary, were more likely to seek physician treatment. Among the listed alternative therapies, acupuncture and TCM were sought more commonly among migraineurs (6.9%) than in headache (1.5%) or chronic daily headache (2.4%) sufferers.
Treatment modalities in headache (N = 2315), migraine (N = 247) and chronic daily headache (N = 204). Except for ‘no treatment’, children may report receiving more than one treatment modality. Complementary and alternative medicines include traditional Chinese medicine, acupuncture, dietary restrictions, relaxation therapy, meditation, yoga and massage with medicated oils.
Discussion
The prevalence of headache in Singapore schoolchildren is high at 80.6%, and is comparable to that in the developed countries of Europe (10,11), though higher than the general prevalence quoted by studies in India (18%–21%) (6) and China (17.0%) (7), countries whose ethnic groups are represented in this study. Similarly, migraine prevalence in this study was similar to that in Europe and the United States (9–12), but higher than that reported in Japan (4.8%) (8). School-entry headache prevalence was similar to that shown by Sillanpaa et al. (51.1%) (27). Similar to other studies, girls were more predisposed to headaches and migraine, with prevalence increasing with age (10,28,29). In adolescents, however, this study had a higher migraine prevalence of 1 in 8 compared with 1 in 16 adolescents in the American Migraine Prevalence and Prevention (AMPP) study (30).
Similar to studies demonstrating strong associations between examination periods with headaches (31,32), headache peaks were found in Primary 3 (national screening for gifted education suitability) and Primary 6 (Primary School Leaving Examination) among boys. There was, however, lower prevalence of headache in Primary 4 and 5, this corresponding to a major nationwide revision to streaming at Primary 4 to a less stressful curriculum in 2004, capturing students in this study transitioning through these changes. These findings may suggest a gender-based predisposition towards headaches in the setting of heavy academic demands. Further investigation into these cause-effect relationships and the relative roles of gender, different school environments and parental expectations can only be validated in future prospective studies.
Surprisingly, the prevalence of migraine in children stood in direct contrast to a local study of adults by Ho et al (3)., which reported migraine prevalence to be lower (3.1%) in the Singaporean population than in the Caucasian communities. The reason for this difference may be twofold. Firstly, there were differences in migraine definitions in the adult study: MA was not included in the general migraine prevalence of 3.1%, though estimates of MA in local adults potentially ranged from 1.2% to 13.1%. Secondly, migraine prevalence in adults could have been underestimated because of over-restrictive migraine duration by ICHD criteria, as mentioned by the authors. In this study, if the more restrictive duration of two hours was adopted as the cut-off for migraine definition, prevalence of migraine in children would still be higher at 6.3%.
Prevalence of TTH was lower than that found in epidemiological studies of children and adolescents in Europe (24.7% and 18%, respectively) (12,33), but higher than India (3.6%) (6). A majority of children (79.6%) with probable TTH did not fulfil criteria because of an inadequate number of headache episodes. It is possible that the prevalence of tension headaches was underestimated, and it could be higher if these children were followed up over time (34). On the contrary, the prevalence of probable migraine may be overestimated, as 4.6% in the cohort could have alternatively been assigned as TTH. The nature of this study, asking for ‘typical’ headaches, also involved difficulties in assessing the co-existence of two headache types. Absence of a physician-directed history may have been an important reason for this ascertainment difficulty, and these diagnoses could only be clarified with clinical evaluation. The proportion of unclassified headaches actually decreased in adolescents, likely reflecting the natural evolution of migraine as well as better symptom reporting. Follow-up of younger children with unclassified headaches is therefore important, as there is a chance that unclassifiable headaches may evolve into headache types warranting specific treatment.
Results from the PSC checklist screening highlighted the important link between headaches, stress and sleep (especially insomnia and sleep deprivation) that are core to the headache-sleep-affective syndrome (35). This link should be emphasized in schools for better management of children with headaches in the local population. It is of concern that a high proportion of headache sufferers perceived stress in schools. The PSC can hence function as a tool useful for the holistic evaluation of children in this area. Sleep screening strategies should also be encouraged in the routine management of such children (36).
The burden of headache disability in our community was low despite high headache prevalence. Migraine disability was similar to that found in a school-based study in Turkey (9.94 ± 8.41 to 11.50 ± 12.28) (37), though lower than in another U.S. study (25.1 ± 36.5) (21). The PedMIDAS was higher in subjects with MA (15.2 ± 29.6) than in subjects with CDH (10.0 ± 14.5). It is possible that headache and migraine disability may be underestimated in the local context using this tool. This is because school absences and loss of function in activities, such as homework, as described in PedMIDAS are rare in the local setting because of the strong emphasis on academic performance. In this study, the lower PedMIDAS scores in those with CDH may be because this was a rather heterogeneous group, including children with tension headache features or unclassifiable headaches who may have frequent though milder headaches, diluting the severity of headache disability. These children are also unlikely to report school absences. The Headache Impact Test-6 (HIT-6) could be considered as an alternative, as it does not limit quantifying headache frequency alone as a disability measure, and has been shown to reflect the burden of headache well using questions on pain severity, cognitive and social functioning, vitality and distress (38).
Malays were more predisposed towards having headaches and migraine with aura, but interestingly, there was no difference in disability or PSC scores across ethnic groups. This finding is in contrast to the local adult study by Ho et al (39)., where non-Chinese headache sufferers were more likely to report severe pain and take medical leave than were Chinese headache sufferers. One possible explanation may be that children have headaches of lesser severity and hence lesser disability impact than adults. However, this study also supports that culture-bound differences in attitudes and tolerance to pain are unlikely to be responsible for ethnic differences in headache prevalence. A higher headache and migraine prevalence in Malays may be indicative of a genetic predisposition or other factors contributing to migraine, especially MA (40), and may indeed reveal a true susceptibility that is not accounted for by behavioural responses alone (41).
‘Chronic daily headache’ as defined in this study is not a diagnosis, but a category of disorders that may represent a broad phenotype. There are limited population-based prevalence studies of the disorder in children and adolescents, but this study had a much higher prevalence than quoted in the United Kingdom (0.9%) (10) and Taiwan (1.5%) (42). The discrepancy may be largely due to limitations in this questionnaire study with respect to accurate ascertainment of the onset, evolution and frequency, and role of medication overuse in CDH, which can only be confirmed through a face-to-face interview. The difficulties of rigorous classification to CM and CTTH under ICHD-II also limit strict epidemiological comparisons with other studies, and the evaluation of symptomatology and treatment under each subtype. This study, however, made preliminary observations that up to 7.1% of our students reported such chronicity and frequency to their headaches, findings sufficient to warrant attention and further verification in this community. The biopsychosocial perspective of this disorder was also supported in these children, who had greater disability and psychosomatic complaints (43). Furthermore, CAM is widely practiced among our population with disabling headaches (e.g. migraine and CDH), although unlike in other studies (44), alternative treatments may not be performed in combination with standard medical treatment. Parental beliefs in these therapies may result in under-diagnosis, under-treatment and under-prophylaxis of these children. Parents may need to be educated on the lack of quality of evidence for CAM modalities like paediatric acupuncture (45), and the importance of headache recognition and proper medical treatment as the primary standard of care.
This study may have had limitations in terms of children providing accurate recall of headache symptoms and characteristics. Another limitation was the difficulty in establishing behavioural manifestations of headache, which may be important in migraine diagnosis for young children. It was also difficult to ensure that parents assisting in answering the questionnaires did not modify children’s responses, the original intention being that parents’ involvement would increase accuracy and not over-amplify symptoms.
Despite these limitations, this study revealed novel insights into migraine and headache epidemiology in Singapore children, some of which seemed to differ from other Asian studies, and highlighted previously unexamined differences in predisposition and coping behaviours among ethnic groups. There were some distinct differences from local headache data in adults, and the study findings expand our knowledge of headache phenotypes in our community. The study highlighted limitations in adopting the PedMIDAS in cross-cultural contexts where lifestyle practices of children were different, and revealed the need for better education of Asian parents on headache treatment. This was, however, a cross-sectional study which could not establish direct cause-effect relationship between high headache prevalence, and lifestyle factors of stress and sleep. Nonetheless, this study suggested a possible association between these factors that deserves attention in local school communities and among parents. Prospective cause-effect studies can be performed to validate these factors in child and adolescent headache sufferers in future.
Footnotes
Acknowledgements
This study was supported by the National Healthcare Group Small Innovative Grant NHG-SIG/05013.