
Abstract
Headache is a common problem among adolescents, and variations can be observed in headache types and characteristics. The present study aimed to reach 5562 Turkish children who were investigated six years previously in a school-based childhood headache project, and to evaluate their current headache status. Investigators interviewed the available students with structured questionnaires. New and old data were matched and analyzed. The present study included 1155 adolescents (mean age 15.2 ± 1.1 years), with 582 boys (50.4%) and 573 girls (49.6%). The prevalence of headache was 78.7% (tension-type headache [TTH] 57.5%, migraine 18.6%, unspecified 2.6%). The prevalence of headache was 45.2% six years previously. In the intervening six years, headache prevalence increased and the headache types changed significantly (Kappa: 0.04, p < .01). The most important variation during this time was the significant increase in TTH. Analgesic use was determined in 70.2% of adolescents with headache, with this ratio being higher in migraineurs. In conclusion, there were an increase in headache prevalence and a significant change in headache types over the previous six years. It can also be suggested that new country-based management strategies are required.
Keywords
Introduction
Headaches affect many children during early adolescence. The results of epidemiological studies indicate that headache has become more prevalent among children and adolescents over the last decades throughout the world (1–9). Furthermore, headache is the third-most common illness-related cause of school absenteeism, resulting in substantial impairment among pediatric patients (10).
Migraine and TTH are chronic disorders often starting in childhood and progressing into adulthood. The transition of headache between the two stages is not yet clearly understood. Altering that progression at an early stage may prevent the disabilities that burden most migraineurs. Therefore, it is important to know the factors that possibly affect this process (11).
In line with results from previous epidemiological studies, in the present study the incidence of headache was found to be increased with age during the course of adolescence (12). According to several authors, longitudinal studies and repeated cross-sectional surveys are reported as essential for enhancing the knowledge about the prognostic development of pain disorders and perceived health in the younger population, and for further investigation of possible causal relationships and related factors (13). Recently, several clinical and epidemiological studies have been published on the long-term course of primary headaches in children and adolescents (11,14–21). However, information about the factors influencing the prognosis of headaches in children, especially regarding TTH, is very rare (22–24).
In Turkey, there are no school-based natural history reports about childhood and adolescent headache and there are limited data in the literature on this subject. Also, the effects of headache on daily living activities have not yet been shown in a large study population. This study aimed to reach 5562 Turkish children who had been evaluated by the same team six years prior in a school-based childhood headache project, and to evaluate their current headache status. The determination of the natural history of childhood headache and the variables affecting the progress in Turkey may help to form a basic database about the effects of adolescent headache on daily living activities in a country-specific manner.
Methods
Study design
The details of sample size and design of the original study have been reported previously (2). In the present study, previous data have been compared with the data currently obtained. After acquiring the required permissions (see the ethical issues section below for details), the same schools were visited and the records for students enrolled in the original study were searched. Investigators interviewed the students who were still at the same school as well as students who had been transferred to another school in Mersin, who agreed to join this follow-up investigation. Each student completed a structured headache questionnaire under the supervision of an investigator and a schoolteacher. Schoolteachers were trained on the questionnaire for approximately 45 minutes by two of the investigators (AO and TS). All the data were recorded in a specific database matching with the data of the previous study, and were analysed using appropriate statistical methods. Subjects with unmatched data or deficient questionnaires were excluded.
The number of the students in the second grade was 1385, among the 20 schools studied in 2001. Six years later, in 2007, 570 of them were still in the same school, now in the eighth grade. All of these students agreed to join the investigation and completed the questionnaires. Two schools had to be excluded: one of them was closed, and the principal of the other refused to join the investigation at this stage. Therefore, 815 of the former second-grade students could not be reached because of school changes or deficient school records.
Gender and grade distribution of students a

Data are presented as number of patients and percentage.
χ2 = 0.19, d.f.: 3, p = .97.
χ2 = 3.49, d.f.:3, p = .32.
Headache diagnosis
Frequent headache was defined as at least one headache episode per month. In 2001, results were evaluated according to the published International Classification of Headache Disorders (ICHD) criteria (ICHD-I) (25) and 2007 findings were evaluated by the second, revised edition of the ICHD (ICHD-II) (26).
The ICHD recognizes medication overuse headache (MOH) as a separate headache entity and, in the second edition, defines ergotamine, triptan, analgesic, opioid and combination medication overuse as intake of these drugs as ≥10 days/month doses and simple analgesics with ≥15 days/month doses for >3 months (27). These criteria have been further revised by adding a new subform of MOH emphasizing the combination of acute medications, and evaluating patients overusing medications in different classes, rather than any single class (28). Probable MOH diagnoses have been made according to the mentioned criteria.
Effects of phenotypic variables have been evaluated by anamnesis and body mass index (BMI). The disability caused by headache was evaluated by a PedMIDAS (pediatric migraine disability assessment) questionnaire. The children were asked to record the loss of time due to headache, such as in homework and/or non-work activities (family, social and leisure activities). Total PedMIDAS scores were calculated according to Hershey and colleagues (29). A Turkish translation of the adult form of MIDAS has been previously validated (29,30), and the PedMIDAS questionnaire used in the study was based on this translation.
Ethical issues
The present follow-up study was approved by the Local Ethics Committee of the University of Mersin School of Medicine. Additionally, approvals were obtained from the municipal school administration of Mersin, and from the principals, parents’ associations and the teachers of the participating schools. All data were collected anonymously.
Statistical analysis
Descriptive statistics were used to summarize the data. For comparision of the categorical variables in independent groups, Chi-square was used. The Mann Whitney U test, Student’s t-test, Kruskal Wallis test and Bonferroni correction-Mann Whitney U test were used for continuous variables. For comparison of dependent groups, Kappa analysis, the McNemar test and the Wilcoxon Signed Rank test were used. The Spearman correlation test was used for the correlation of continuous variables. The Binary Logistic Regression test was used in multivariate analysis. In all analyses, a two-tailed p value of less than. 05 was used as the cut-off point of significance.
Results
Sample population
The study included 1155 adolescents (mean age 15.2 ± 1.1 years), with 582 boys (50.4%) and 573 girls (49.6%). Further details are given in Table 1.
We also compared the headache characteristics of the groups (reached and un-reached subjects with headache) and did not find any significant difference except the temple location of the headache. These data indicated that our new group appropriately reflected all of the previous group’s characteristics.
Natural history
Headache was reported in 909 of the adolescents. The point prevalence of headache (headache in the last month) was detected as 78.7%. Six years prior, the headache prevalence was only 45.2% in these students. Regarding headache subtypes, 57.5% were diagnosed as TTH, 18.6% were migraine and 2.6% were unspecified headaches. When the previous and current diagnoses of children were compared, no difference was found in the headache subtypes of 343 children (29.7%). The diagnosis of headaches varied the most (71.3%), and the difference was statistically significant (Kappa: 0.04, p < 0.01). The subjects who did not report headache six years prior commonly reported TTH and subsequently migraine, according to the new interviews. Among the subjects previously diagnosed with migraine, only 16.5% were diagnosed with migraine currently; the current rate was 61.3% for TTH. Overall, 20.3% of subjects previously diagnosed with TTH were diagnosed currently with migraine whereas 14.2% were now headache-free (no headache in the last year). Independent of subjects’ previous diagnoses, TTH was the most prevalent headache type among adolescents in the present study (Table 2).
In girls, the prevalence of headache was higher than in boys (85.3% vs. 72.2%, χ2 = 29.9, d.f.: 1, p < .001). Whereas the migraine prevalence was 9.9% in females six years prior, it was found to be 21.5% in the present study. These rates were 7.9% and 15.8% in males, respectively (Table 3). Headache prevalence was 81.5%, 80.4%, 71.8%, and 70.8% at the eighth, ninth, tenth and eleventh grades, respectively. Headache prevalence was highest at the eighth grade, and this difference was statistically significant (χ2 = 12.0, d.f.: 3, p < .01). The distributions of headache types according to the grades are seen in Figures 1A and 1B.
(A) The linear trend of headache diagnosis 2000–2001. TTH: tension-type headache. (B) The linear trend of headache diagnosis 2006–2007. TTH: tension-type headache.
Changing pattern of headache diagnosis after an interval of six years a

Data are presented as number of patients and percentage.
Headache types of students according to gender a

Data are presented as number of patients and percentage.
χ2 = 12.8, d.f.: 3, p < .01.
χ2 = 38.4, d.f.: 3, p < .01.
Clinical characteristics of migraine and TTH in adolescent students
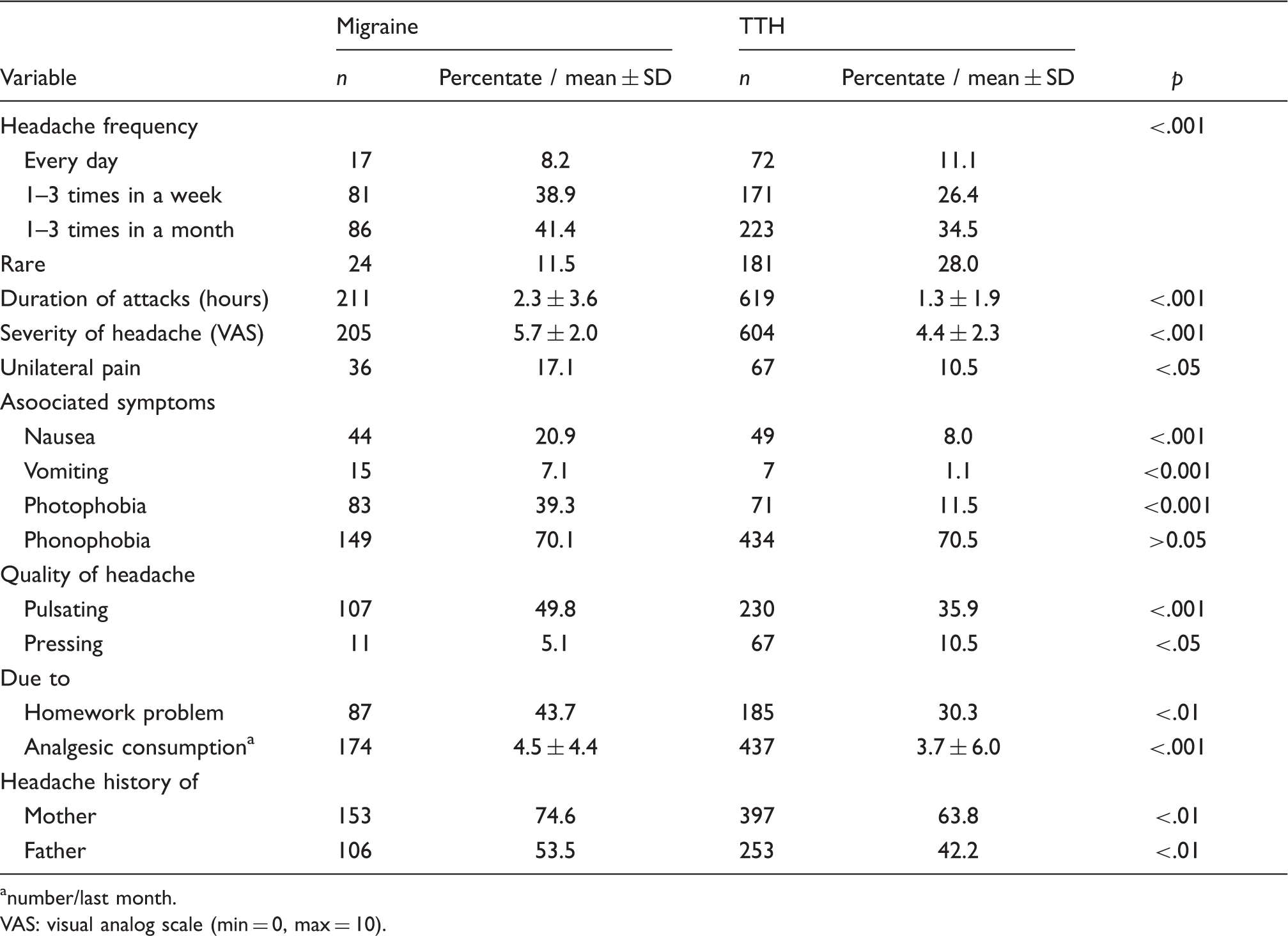
number/last month.
VAS: visual analog scale (min = 0, max = 10).
Markers of prognosis
The risk factors influencing the development of headache in the adolescents without headache in 2001 were as follows.
Female gender increased the frequency 2.36 times (95% confidence interval [CI]: 1.43–3.89, p < .01). Having a working mother increased the frequency 2.53 times (95% CI: 1.20–5.32, p < .05). Having a sibling with headache increased the frequency 2.39 times (95% CI: 1.17–4.87, p < .01). Having no sibling decreased the frequency 0.9 times (95% CI: 0.05–0.15, p < 0.01).
On the other hand, the risk factors influencing the persistence of headache in adolescents who had headache in 2001 were as follows.
Female gender increased the frequency 2.24 times (95% CI: 1.23–4.08, p < .01). Having a mother with headache increased the frequency 2.08 times (95% CI: 1.12–3.85, p < .05).
To analyse the variation in headache characteristics by time, we evaluated 17 subjects with migraine and 160 subjects with TTH, who had the same headache diagnosis at both the original and follow-up studies. Headache severity was evaluated by disruption of daily living activities (interruption in watching TV and games, etc.) in the original study, but the Visual Analog Scale (VAS) was used in the follow-up study. As a result, the variation in headache severity could not be evaluated statistically. No significant differences were detected in headache frequency, headache precipitation by exercise, localization of headache, accompanying nausea or analgesic consumption rates in our migraineous subjects. In the TTH group, the ratio of children with headaches one to three times a week increased significantly (26.4% vs. 42.8%, McNemar test p < .01). The mean headache duration decreased significantly (1.5 ± 1.5 hours vs. 1.3 ± 2.1 hours, Wilcoxon Signed Rank Test Z = −2.5, p < .05). The frequency of accompanying nausea also decreased over time (21.4% vs. 8.0%, McNemar test p < .05). The rest of the antecedents and clinical characteristics did not demonstrate significant differences between the two populations studied.
Medication overuse and headache
Overall, 626 (70.2%) of the children with headache were using an analgesic of any kind. The rates of analgesic usage in migraine, TTH and unspecified headaches were 80.7%, 66.6% and 73.3%, respectively. The high rate of analgesic usage determined in migraine was statistically significant (p < .001; see Table 4). Medication overuse criteria was seen in 118 (13.0%) of the adolescents with headache diagnoses (probable MOH). Medication overuse was observed in 21.4% of migraine subjects, 8.7% of TTH subjects and 46.7% of the unspecified headache group (χ2 = 54.2, d.f.: 2, p < .001). There was no significant difference between males (12.6%) and females (13.3%) (p > .05). Headache severity was 6.2 ± 2.1 (VAS) in medication overusers and 4.6 ± 2.3 (VAS) in others, with a significant difference between them (Student’s t-test: −7.3, p < .001). The other headache characteristics did not show significant differences for this headache group.
Significant variables affecting medication overuse frequency

CI: confidence interval; OR: odds ratio; PedMIDAS: pediatric migraine disability assessment.
Daily living activities and headache
Disability associated with headache was evaluated by PedMIDAS questionnaires. Previous studies have shown that PedMIDAS is a useful test to evaluate daily living activities in children and adolescents.
The median PedMIDAS score was 6 (range, 0–215) in males and 7 (range, 0–167) in females. There was no statistically significant difference between male and female groups in the PedMIDAS score (p > .05). The median PedMIDAS score in the migraine group was 11 (range, 0–215), in the TTH group 5 (range, 0–167), and in the unspecified headache group 18 (range, 0–92) (Figure 2). There was a statistically significant difference between headache types and PedMIDAS scores (Kruskal Wallis test, χ2 = 60.5, p < .001).
Headache type and pediatric migraine disability score (PedMIDAS. TTH: tension-type headache.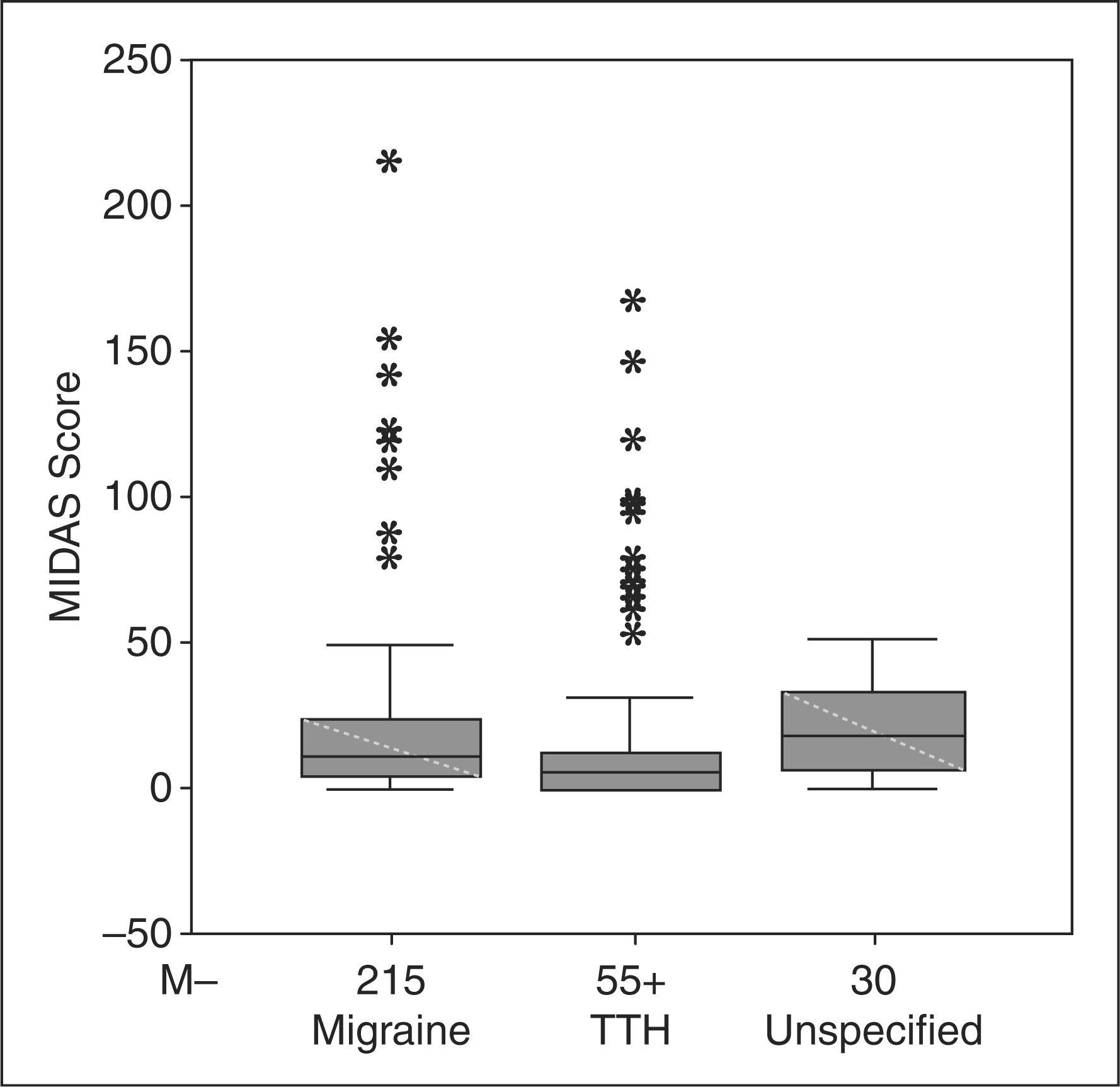
There was a weak, but statistically significant correlation between headache severity and PedMIDAS scores (rho = 0.31, p < .001). There was a statistically significant relationship between headache frequency and PedMIDAS score (Kruskal Wallis test, χ2 = 138.4, p < .001). The PedMIDAS score was higher in subjects with maternal and paternal headache history than the others, respectively (Mann-Whitney U test = 64,260, p < .001; Mann-Whitney U test = 74 737, p < .01).
Body mass index and headache
The mean BMI was 19.8 ± 2.8 kg/m2 (range, 12.3–35.5). According to headache types, BMI was 19.8 ± 3.0 kg/m2 in the group with no headache, 19.6 ± 2.9 kg/m2 in the migraine group, 19.9 ± 2.8 kg/m2 in the TTH group and 19.7 ± 2.4 kg/m2 in the unspecified headache group. There was no statistically significant relationship between headache types and BMI.
Discussion
Sample characteristics
In the present study, the available 1155 students provided enough statistical power to represent the original sample of 5562 students. After an interval of six years, only 21.3% of the subjects evaluated in 2001 remained headache-free (no headache in the last year). Though headache persisted, the diagnoses of headache changed in most of the students (71.3%).
Natural history
Prevalence rates for headache (especially primary headaches) in children and adolescents range from 19.5% to 93.3%. The wide range observed in the studies depends on many methodological, geographical, sociocultural and ethnic factors. From the aspect of adolescence, a period between childhood and adulthood, there are many physiological and psychological alterations and most headache sufferers experience their first attack during this period. Therefore, adolescence and being a student are important cornerstones for the evolution of headaches (5,8,22,31).
There are limited data supporting changes in the incidence of migraine and frequent headaches, over time. In a recent Finnish study, the incidence of recurrent headaches was found to be strikingly high among children at school-starting age (32). Moreover, the highest prevalence rate of headache observed among schoolchildren was at the age of 13 (33). The incidence of childhood migraine and frequent headache has been substantially increasing over the last 30 years. The increase in the incidence is alarming and reflects untoward changes in the lifestyles of children (34). In a 40-year follow-up study, Bille reported that migraine prevalence was 1.4% at the age of 7 and 5.3% at the age of 15, with the peak prevalence at the age of 11, predominantly in females. After 25 years, while migraine improved in 23% of subjects, one-half of them still had headaches by the age of 50 (14).
There are few data published in the literature discussing the evolution or prognosis of migraine and TTH beginning in the pediatric age group, and each study tends to use different methodologies and duration. Congdon and Forsythe found the migraine remission rate to be 34% during a follow-up period between 4 and 10 years (35). Sillanpaa found this rate to be 22% in a seven-year follow-up, if the starting age was before 8 years of age, and 25% if the starting age was after 14 years of age (23).
In a two-year longitudinal study of schoolchildren, about one-third continued to report headaches (12,36). Metsahonkala et al. found that the majority of children aged eight to nine years with migraine headaches (63%) continued to have migraine headaches, which were somewhat more stable than nonmigraine headaches (57%) in a three-year follow-up period (24). In a study from a specific headache center, childhood headaches that did not meet the diagnostic criteria of migraine and TTH at the first visit have been reported to be improved in the next year, with a ratio of 30%. In children with IHS specific diagnoses, 20% remained unchanged, whereas 20% changed diagnoses between migraine and TTH (18). Another study from this center showed that 30% of the children and adolescents admitted to a headache center due to migraine or TTH became headache-free in the longt erm. The other 20% to 25% of subjects shifted from migraine to TTH or vice versa. The prognosis of headaches can be adversely affected by an initial diagnosis of migraine and by changing headache location, and it tends to be affected by increasing time between headache onset and admittance (37). The natural history of headache in children and adolescents has been previously studied. In a 26-year survey, when children with primary headache diagnoses were evaluated 15 years after the original evaluation, according to the IHS criteria, the diagnoses were 10.8% migraine, 8.8% TTH and 5.9% combined headache, but 29% of the headaches were reported as frequent headaches that did not meet IHS criteria. Our long-term study survey with a broad sample population showed a remission rate of headache at 16.4% in the adolescents (86 participants out of 522 with headache became headache-free in the present evaluation). The overall headache frequency (78.7%) increased in students diagnosed with TTH, primarily in girls. The peak rate of headache prevalence was detected in the eighth grade, suggesting the importance of stress factors in our country.
Distressing events can increase combined headaches during childhood and adolescence (13), and TTH was more prevalent in children living with physical stress, while migraine was usually affected by psychological stress (38). In our study group, the increased headache prevalence at eighth and eleventh grades, especially in TTH, supported the role of stress. Also, the increased TTH prevalence from 22.5% to 57.5% and increased migraine prevalence from 8.9% to 18.6% after an interval of six years (2000–2001 compared to 2006–2007) were striking, and demonstrate the increasing prevalence by increasing age.
In a 26-year follow-up study from the United Kingdom, the probability of adolescent headache has been reported to be 2.22 times more than the normal population in childhood headache sufferers (39). In a 15-year follow-up study in the children who had headache at six to seven years of age, 24% of males and 53.9% of females were diagnosed with migraine (40). In our study, 16.5% of childhood migraine sufferers and 14.2% of childhood TTH patients improved to headache-free status.
A small sample (60 of 95 children, 63% of the original cohort) from a long-term (20-year) prognosis study of Atlantic Canadian children showed that 27% were headache-free, 33% had TTH, 17% had migraine and 23% had migraine and TTH. Having more than one headache type was more prevalent at diagnosis or initial follow-up, and headache type varied over time (41). Therefore, we evaluated the changes in clinical characteristics of headache in migraine and TTH subjects in this epidemiological-based long-term survey study. Headache characteristics in adolescents seemed to be similar to the adult headache characteristics, especially in the migraine group. The increase in migraine and TTH prevalence, the headache duration and frequency and the analgesic overuse frequency were striking. Also, changes in lifestyle were effective as provocating factors in migraine subjects.
In a five-year follow-up study from Italy with 64 children, headache diagnoses did not change in 56.2% of subjects with migraine without aura, whiereas headache diagnoses changed to TTH in 12.5% of subjects (42). In another follow-up study from Italy, the changes of headache diagnoses, especially in migraine and TTH, independent of gender, were reported over a period of eight years. At the end of eight years, 43.8% of migraine and 14.3% of TTH subjects maintained the original diagnoses (22). Although there is high sensitivity in diagnosing certainity in clinical studies, the selection of subjects and the limitation of sample size are the main handicaps when compared with epidemiological-based studies. By using questionnaires based on IHS criteria, the diagnosis sensitivity of epidemiological-based studies have improved (2) and the changes between diagnoses have been found to be significantly high. In our study, the transformation rate of migraine to TTH was 62.1% and from TTH to migraine was 20.3%. However, as subtype analyses are not reliable in questionnaire studies, we did not analyse the subtypes of migraine.
Long-term surveys as well as short-term surveys show that female gender constitutes higher risk for migraine (13,22). A study from Sweden supported that children (especially girls) with frequent headaches had poor prognosis, and the authors suggested that intervention is particularly important in these groups (21). The high rates of transition between migraine and TTH observed in these studies, as well as in our current study, suggest that these diagnoses are related or, as previously proposed, are extremes of the same disease spectrum (43–45). In our epidemiological-based study, subjects who did not meet the IHS criteria were coded as unspecified and when compared with the previous records, the changes in diagnoses were mostly seen in migraine (24.1%) and TTH (51.9%). The variables affecting the headache diagnosis at adolescence were female gender (odds ratio [OR]: 2.36, p < .01), having a working mother (OR: 2.53, p < .05), headache in a sibling (OR: 2.39, p < .01) and having a sibling (OR: 0.9, p < .01) according to our database. Having a working mother and a sibling are the striking factors that have not been mentioned in the previous reports.
The risk of having migraine during adult age increases with the low education level of parents and the misuse and/or overuse of analgesics, even if the migraine frequency is low during childhood (46). Analgesic overuse is reported to be 13.8% in our sample population and is even higher (21.9%) in the migraine subgroup. These data are significant and highlight the importance of MOH in adolescents in our country. In a regression model, headache severity, headache type (in favour of migraine), having a sibling, having a sibling with headache and the negative effect of headache on daily living activities are the major determinants of medication overuse. Adolescents with migraine, especially with a family history, are in the high-risk group (14) and prior strategies should be determined for MOH in these groups.
In a community-based cohort, outcomes and predictors of chronic daily headache (CDH) in adolescents were assessed via annual follow-up evaluations by neurologists for two years via a semistructured telephone interview. Most of the adolescents with CDH continued to have frequent headaches (40%), although the incidence of CDH decreased (25%) during follow-up (47). Another clinical-based four-year follow-up study showed that psychiatric disorders are notable in CDH patients (64%), and that the disorders (mainly anxiety) predict poor outcome. Surprisingly, analgesic overuse is not involved in the development of chronic headache (19). The ratio of analgesic use observed in the present study (70.2%) was similar to the ratio (70%) obtained in Canadian Atlantic Children Study (40). An important adult study showed that the frequency of primary headache disorder, ergotamine overuse and disability of chronic headache were estimated by MIDAS as independent predictors of treatment efficacy at a one-year follow-up (48). Perhaps the suggestion that ‘medicine use can be regarded as part of a cluster of risk behaviors among young people’ should be properly considered. Moreover, we think that the prevalence and risk of MOH in adolescents should merit more research in population- and clinical-based designs.
Daily living activities and BMI and headache
School-related disability is one of the most important components of a child’s quality of life. School is important for social, intellectual and emotional development in childhood. Migraine headaches may cause abseentiism from school or may affect a student’s school or homework performance. Many studies have reported that migraine attacks bring significant disruption to family life, with an impact on spouses, children and friends (8). However, there are only limited data about the disability of TTH as measured by PedMIDAS in adolescents. We evaluated headache (migraine and TTH) disability by means of a PedMIDAS questionnaire. A previous report from Turkey showed that total PedMIDAS scores of 9.94 ± 8.41 days in boys and 11.50 ± 12.28 days in girls over a three-month period. There were no statistically significant differences between gender with respect to PedMIDAS scores (8). Our survey showed that migraine caused higher disability scores than TTH, independent from gender, but these scores were highly correlated with headache severity, headache frequency, and positive family history of headache by using PedMIDAS. There was also a significant effect of age on migraine disability scores, possibly correlated with stress factors.
Contrary to our clinical experiences, no significant relationship between BMI and headache characteristics was detected.
Study limitations, strengths, and overall conclusions
All of the students evaluated in the first study could not be reached, and this was the major limitation of this study.
However the present study does have several unique strengths. It was the first school-based, broad sample epidemiological natural history study conducted in Turkey. The data were collected by using validated questionnaires. Additionally, due to the large sample size (1155 students), the subanalyses were well powered. This allowed long-term prognosis and prognostic factors to be determined in both migraine and TTH subjects. Finally, headache and some important associated factors (daily living activities, BMI, medication overuse) were evaluated separately.
In conclusion, this study showed that childhood headache persists in adolescence, although the diagnoses mostly changed over time. Headache prevalence increased with advancing age, especially in females, and stress factors (examination stress, working mother, family history of headache, having a sibling, headache in the sibling) were the most important determinants. We also showed that headache (especially migraine) negatively affects daily living activities in adolescents. Because headaches contribute to school absenteeism and a poorer quality of life, understanding the natural history and the management of headaches is vital for children and adolescents.
Footnotes
Acknowledgements
This study was partially financed by the Turkish Headache Study Group Award of Best Headache Paper of 2006 for the first author (AO). We express our great appreciation to all the junior high school students, teachers and principals in Mersin city for participating in this study, and to the Provincial Governorship of Mersin for permission. We also thank Associate Professor Handan Ankaralı for her worthy statistical support and OMEGA for English revision supported by Pfizer.