
Abstract
Assessment of attack intensity in primary headaches of paediatric age has not received great attention in the literature to date and in the international classification the criteria to define pain intensity are also not specified. The purpose of this research was to evaluate whether behaviour during attacks, reported by the child or a parent, can be used as a measure of attack disability, and so as an indirect measure of attack intensity in primary headaches of children and adolescents. The subjects were 320 patients aged between 3 and 14 years (mean age 9.9 years, SD 2.6 years) affected by primary recurrent headaches and first seen at a headache clinic. Twelve variables taken from their history were considered and sequentially analysed with multiple correspondence analysis and cluster analysis. Five types of behaviour during attacks were identified: (i) the child (or the parent) is unable to answer the questions or the child has no limitation in activities; (ii) the child may have some activity limitation, but only in lively games; (iii) the child has limitations in daily life with regard also to quiet activities; (iv) at least during some attacks the child lies down with closed eyes or in the dark; (v) during each attack the child lies down with closed eyes or in the dark. The least important variables for the identification of the five behaviour types were studying at school and absence from school. There are some limitations in considering child's behaviour as a measure of attack intensity/disability; one of these is the fact that it was found to be related to the educational level of the mother. However, behaviour during attacks, reported by the child or the parent, provides useful information independently of child's age and, together with the score of pain, when this is given, it can be used as measure of attack intensity.
Introduction
In adult patients, von Korff (1) makes a distinction between attack intensity and global severity of chonic pain status, considering this last aspect as the result of intensity and interference with daily activities. In his opinion, ‘attack severity’ can be characterized by intensity of pain, presence and intensity of associated symptoms, episode duration, headache frequency, frequency of use of headache medication, and interference with activities. Terminology used in the literature can be confusing and the impact of illness on ability to function in various life areas over a period of time has also been called disability; this was examined mainly in adults for whom the Migraine Disability Assessment (MIDAS) questionnaire was created and validated (2, 3). For paediatric age, some changes in the questionnaire have been made and a specific PedMIDAS has been created (4). Assessment of attack intensity and of disability is important for planning treatment and for judgement of treatment efficacy.
Attack intensity is also important for classification. In fact, the International Classification of Headache Disorders (ICHD) (5) includes pain intensity among the criteria to differentiate migraine without aura (in which pain intensity is moderate or severe) from tension-type headache (in which pain intensity is mild or moderate). In a previous study (6) performed on 320 children or adolescents with primary headaches, we found that intensity and number of precipitating factors may be useful for distinguishing between migraine without aura and tension-type headache: patients with migraine showed a higher number of precipitating factors and a greater attack intensity. Wöber-Bingöl (7) found that intensity of pain, together with aggravation of headache by physical activity and nausea and vomiting, were the most important features for distinguishing migraine from tension-type headache in the paediatric age group. In the ICHD the criteria to define pain intensity are not specified.
Furthermore, generally, assessment of attack intensity in primary headaches of paediatric age has not received great attention in the literature. The purpose of this research was to evaluate whether a child's behaviour during attacks can be used for the assessment of attack intensity in primary headaches of children and adolescents.
Subjects and methods
Participants
The subjects were the same 320 patients described in a previous paper (6), seen since 1997–2000 in Milan (2nd Paediatric Department of Milan University). They were aged between 3 and 14 years and were first seen for primary recurrent headaches at our headache clinic. None of them had ever had a migraine prophylaxis. Children were included in the study if their history of headache had lasted for at least 4 months; definition of migraine or tension-type headache was performed according to the ICHD (5).
Procedure
All children of school age were requested to fill in a short questionnaire concerning characteristics of their headaches, associated symptoms and precipitating factors; the results of the questionnaire were then discussed with the child and the child's parent(s) and a detailed history was recorded. The educational level of the mothers was also taken into account.
The medical doctor (who had experience with children affected by headache and was specifically instructed) filled in a second questionnaire. To assure homogeneity, a paediatric neurologist supervised all the cases. Then both a neurological and a general examination were performed; if necessary, other types of investigations (e.g. neuroradiological imaging) were done. Children with secondary headache were excluded from the study. The paediatric neurologist then filled in a final form which was used to construct the database for this study.
In the last form the following variables describing the attacks were considered: (i) characteristics of headache (type and localization of pain, aggravation or not by routine physical activities); (ii) associated symptoms or signs (presence of any symptom or sign, its frequency and duration); (iii) frequency and total duration of attacks; (iv) precipitating factors; (v) behaviour during attacks; (vi) drugs given during attacks and their effects, effects of lying and sleeping on attacks. A mean score of the pain and of the associated symptoms according to a 10-point analogue scale was also given by the patient when the patient was able to do this. Frequency of associated symptoms or signs was coded according to the three following possible results as: present in no attack, in some attacks, in all attacks. For subjects who had had a change in their attacks, the characteristics of the attacks during the last 2 months were considered.
The procedure is described in detail in the above-mentioned paper (6).
Statistical analysis
The 320 children were grouped according to their behavioural characteristics during headache attacks, so as to obtain a behavioural classification. With this aim the interrelationships between 12 categorical variables describing the behaviour were analysed by multiple correspondence analysis (MCA) (8, 9) and cluster analysis (CA) was sequentially performed.
MCA, which is a descriptive technique similar to factor analysis, leads to a graphical display where subjects are represented as points. The location of points indicates the characteristics of the subject and the difference between the characteristics of subjects is proportional to the distance between points.
CA defines groups of subjects in such a way that the differences between the groups are as large as possible and, at the same time, differences between subjects within each group are as small as possible. The groups have been named B1 to B5.
The significance of the association between behavioural groups (B1–B5) and characteristics of headache was tested by χ2 test.
Results
Among the 320 children, 144 were male (45%). Mean age at first examination was 9.9 years (SD 2.6 years). Mean age at onset of headaches was 7.3 years (SD 2.7 years).
In the MCA the first two axes (each of them explaining about 37–38% of the total information given by the data) differentiated the types of behaviour of the children during their headache attacks: from a strongly modified behaviour (e.g. they must stop playing even quiet games) to a slightly modified behaviour. In the first factorial axis the most significant variables, among the 12 variables considered, were, in decreasing order of importance: playing (or not) quiet games, watching the TV, lying down with closed eyes, lying down, sleeping. In the second axis the most significant variables in decreasing order of importance were: playing (or not) lively games, doing homework, playing quiet games, watching the TV, eating, playing with computer. The least important variables for the identification of the behaviour groups were: studying at school and absence from school.
The five behaviour groups identified with the CA are shown in Fig. 1. The most significant variables for the description of the different types of behaviour are shown in Table 1.
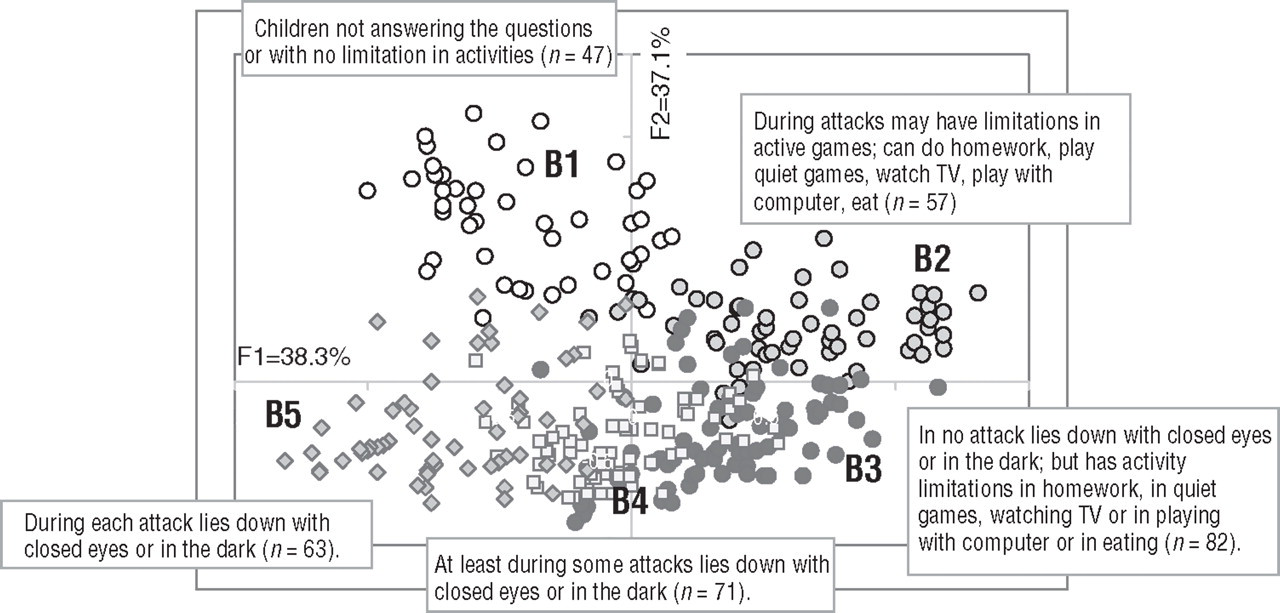
Location of the five behaviour groups (B1–B5) on the plane of the two first factorial axes of the multiple correspondence analysis. Percentages are the proportions of variance explained by factorial axes.
Percentage of children within each behaviour group (B1–B5) for the most important variables of the multiple correspondence analysis

All the variables are significantly associated with the behaviour groups (P < 0.01) and are shown in decreasing order of importance.
To assess the clinical significance of the above described behaviour groups, a clinician with much experience with children affected by headaches was requested to identify different types of behaviour during the attacks, ordering them according to her opinion about attack intensity. The classification obtained by the clinician was compared with the results of the CA and a substantial association concerning the sequence of the behaviour groups was obtained (χ2 = 403.9; d.f. = 12; P < 0.001). However, CA isolated a group of children (B1) more effectively than the criteria suggested by the clinician; this group was composed mostly of children who did not answer the questions. When compared with the other four behaviour groups, group B1 was composed of a higher percentage of children with mothers of a lower degree of education (χ2 = 17.8; d.f. = 4; P < 0.01) (Table 2). No significant relationship was found between behaviour groups and gender or child's age.
For each behaviour group, description of mother's education and children's gender and age
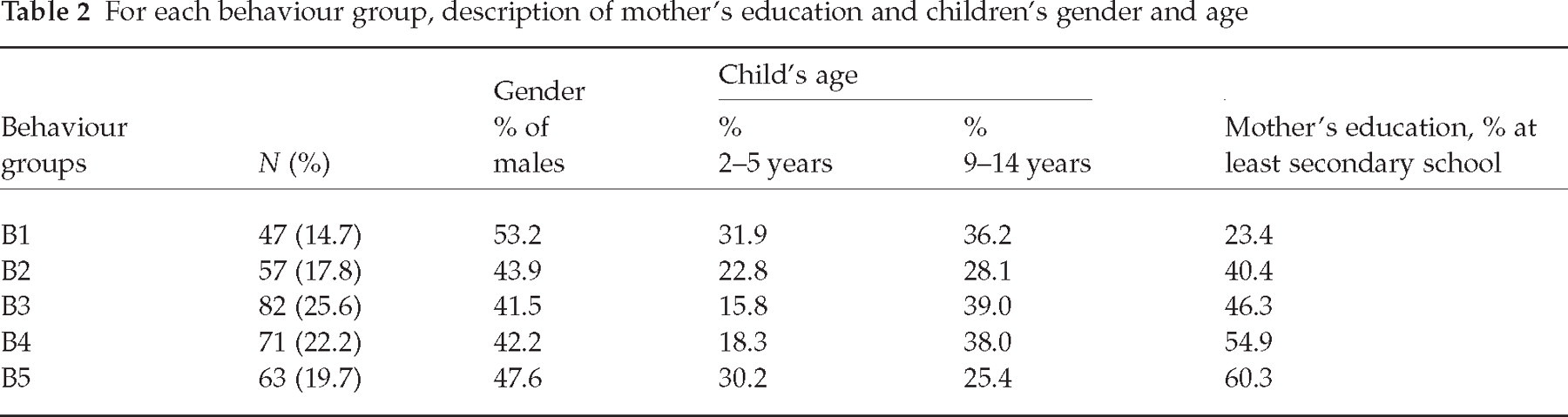
Table 3 shows the relationship between the obtained behaviour groups and the definition of the headache form according to the ICHD, and also that between the groups and the variables which are useful for the distinction between migraine and tension-type headache; the number of precipitant factors was also taken into consideration.
Frequency distribution of variables within behaviour groups obtained by cluster analysis

Among the 28 excluded subjects: 12 had migraine with aura; 16 were unclassifiable.
A highly significant relationship (χ2 = 55.8; d.f. = 6; P < 0.001) was found between age and score of pain intensity given by the child, the score being higher for older children. The relationship between age and pain score was higher for the children with mothers of a higher educational level (P < 0.001). In contrast, no significant relationship was found between child's age and score of photophobia or phonophobia.
Discussion
For assessment of attack intensity in adult patients, von Korff (1) uses a 10-point rate scale; the patient judges the average and the intensity of his own worst pain in the previous 6 months; furthermore, he reports ‘how many days in the last 6 months she/he was kept from usual activities because of headaches’. In literature, as far as we know, no study deals specifically with assessment of attack intensity in paediatric patients.
This study shows that it is possible to distinguish patients according to various types of behaviour during headache attacks and that these behaviour types correspond to different associations of clinical characteristics. Therefore, behaviour during attacks, reported by the child or a parent, can be used, at least partially, as a measure of attack disability, and so as an indirect measure of attack intensity. This seems to be true also for very young patients, who are unable to give a score of their pain. The existing significant relationship between behaviour during attacks and the scores of pain intensity given by the patients, according to a 10-point rate scale, seems to show reliability in reported behaviour. Report of behaviour during attacks differs from the PedMIDAS questionnaire because it is related to the individual attacks and does not indicate the impact of the attacks on various life areas over a period of time.
Among the variables used to describe behaviour, the least related to the five behaviour types found were those concerning activity in school. Therefore, activity in school is perhaps the consequence of the practice of teachers or parents more than being strictly related to attack intensity. In contrast, in the PedMIDAS this aspect is accorded high importance (4).
The groups of behaviour showing the highest attack intensity (types 4 and 5) were found to be highly related to the following clinical characteristics: high intensity of pain, presence of vomiting, attack duration longer than 1 h, high number of precipitating factors. Behaviour types 4 and 5 have also been found related to high intensity of photophobia; however, to determine the intensity of associated symptoms, scores given by the patients according to a 10-point analogue scale were used. As associated symptoms are not typically rated in this way, we doubt the importance of this finding. Surprisingly aura seemed to be of no importance in the relationship with behaviour. Visual aura, in our experience, is very frightening for children and adolescents but probably this symptom does not affect their behaviour in general during attacks because it seldom recurs in the same patient.
There are some limitations in considering behaviour as a measure of attack intensity/disability. One of these is the fact that behaviour was found to be related to the educational level of the mother. More children with mothers with a higher educational level lie down during their headache attack. Perhaps this is due to the mothers' greater ability to find a means to decrease pain. Therefore the variability of behaviour may be due at least in part to factors which have nothing to do with the intensity of attacks, but are more related to social or cognitive characteristics. In a study of adult patients with migraine or tension-type headache the behaviour during attacks was found to vary with the diagnosis (10); the authors of the study concluded that the behavioural differences may be due to the different pathogenesis or to different ways of dealing with the pain.
Another limitation is the fact that in ‘behaviour group 1’ we put together children who were unable to describe their behaviour during attacks with children who showed no limitations during attacks; the reason is that we had the impression that in several cases children (or parents) were unable to describe the behaviour because attacks were mild. A further limitation of the study is that, when considering the most common behaviour during attacks, the variability of attack intensity is not taken into account; this is a common problem in all studies concerning evaluation of attack intensity. For example, in studies on PedMIDAS the mean intensity of attacks is considered (4). Also the impact of medication on attack intensity is not considered in this study; again, this is a problem in all studies on attack intensity, because of the fact that several variables need to be taken into account (such as kind of medication, drug dosage, time of administration after the beginning of the attack), and this makes the evaluation of the impact of medication very difficult.
Unlike the PedMIDAS questionnaire, description of behaviour during attacks could be employed for the definition of ‘mild, moderate, or severe intensity’, which is one of the criteria employed in the ICHD (5) to distinguish migraine without aura from tension-type headache. As expected, in this study a relationship was found between the groups of behaviour showing the highest intensity of attacks (groups 4 and 5) and the definition of migraine according to the ICHD.
In conclusion, we think that behaviour during attacks, reported by the child or a parent, provides useful information about attack intensity/disability, especially for those children who are unable to give the score of their pain. Together with the score of pain, when this is given, it can be used as a measure of attack intensity. Behaviour could also be used to define intensity in the ICHD, independently of a child's age. It is worth stressing that the behaviour described in this study refers to both the clinical aspects and the children's cultural context. Further studies are necessary to verify if the behaviour types which we identified can be used in different clinical settings.