
Abstract
This study aimed to assess the availability, design, and contents of difficult airway trolleys in hospitals in Victoria, Australia. A survey audit was conducted with a 92.3% reply rate, and the responses from 22 major Victorian hospitals were analysed. The results showed that difficult airway trolleys were available in 100% of operating theatres, emergency departments and intensive care units, and the rate of standardisation was high. Compliance with recommended design features and resources was on average 68.3%. There was no significant difference in the compliance rate of major tertiary centres compared with other hospitals. The carriage of non-essential items was reduced compared with earlier audits. However, there was heterogeneity in the brands of supraglottic airway devices, videolaryngoscopes and cognitive aids used. The study highlights the need for ongoing improvement to the organization and content of difficult airway trolleys, and for further discussion regarding the safety of equipment variation across institutions.
Introduction
The presence of a difficult airway trolley (DAT) in an operating theatre (OT) improves patient safety, especially during an unexpected airway crisis. The Australian and New Zealand College of Anaesthetists (ANZCA) recommends its presence in all theatre locations.1 –3 As equipment issues can contribute to up to 24% of all airway complications,4,5 ideally the DAT should be organised in a logical, useable manner that allows adherence to agreed difficult airway algorithms during scenarios with high stress and cognitive load. 6 Since 2008, ANZCA has maintained and updated a non-prescriptive professional document, PG56(A) guideline on equipment to manage difficult airways (2021), with recommendations for the DAT on general design, organisation and essential items. 3
Historically, the availability and organisation of DATs have varied considerably across health services within Australia and New Zealand. For example, in 2007 Baker et al. found that only 43% of audited metropolitan hospitals in Auckland had a dedicated DAT. 7 They also raised significant concerns regarding DAT quality and equipment availability, finding only one DAT with capnography, and several trolleys with expired equipment. Over the subsequent decade, other studies have shown that while access to a DAT had improved significantly within OTs, compliance with recommended content and design of the ANZCA PG56(A) document remained variable,5,8 and access to a DAT within the intensive care unit (ICU) and emergency department (ED) was less than 50%, identifying a significant safety gap. 8 This was particularly significant given that the Fourth National Audit Project (NAP4) demonstrated an increased incidence of intubation failure and airway-related deaths within the ICU and the ED. 4 The creation and continued updates of the ANZCA PG56(A) guideline, with input from experts from anaesthesia, intensive care medicine and emergency medicine, was part of the effort to improve this. 3 However, the current situation regarding the DAT in Victorian hospitals remains unknown.
A previously unexplored area is the heterogeneity in key airway rescue equipment stocked across the hospital system. The ANZCA PG56(A) background paper makes detailed recommendations regarding the contents of the trolley; it provides generic and non-prescriptive advice regarding standardisation, recommending some degree of standardisation at least ‘within an institution’. 2 The anaesthetic workforce is heavily based on the visiting medical officer (VMO) model of staffing across the country.9,10 Many VMOs work across multiple institutions, and encountering unfamiliar equipment and processes has been identified as a major safety risk.11,12 This is particularly relevant due to the increase in recent years of different types of new airway devices and protocols, notably including the videolaryngoscope, second-generation supraglottic airway devices (SADs) and difficult airway algorithms.3,13 Each one requires its own learning curve,14,15 so the acquisition of different commercial brands by health services presents a risk of eroding the safety and redundancy built into the DAT.
This study aimed to audit the DATs within the OTs of a comprehensive sample of hospitals from both private and public (as well as metropolitan and rural) hospitals in Victoria, Australia. We estimated that these hospitals would serve over 90% of Victoria’s population. In particular, we aimed to investigate: (a) The availability and accessibility of DATs in the OT, ED, and ICU settings; (b) The compliance of the DATs within OTs with content and key design recommendations of the ANZCA PG56(A) document; (c) To identify areas of heterogeneity of DATs within OTs across health services; and (d) To assess standardisation of the DATs between the three critical care departments within the same health service.
Methods
Study design
The investigators designed a prospective web-based 168 data point questionnaire (online supplementary material) to audit the DATs based on the extent to which they followed the recommendations of the ANZCA PG56(A) document for DAT design and contents. The questions were predominantly designed to elicit binary ‘yes’ or ‘no’ responses. Tick boxes were used in sections where a wide variation of answers was expected. Standardisation criteria were created by consensus among investigators based on ANZCA guideline recommendations. Comment sections were included to allow further clarification.
Participant population
We used purposive and convenience sampling through the Victorian ANZCA Airway Lead Committee to choose hospitals to participate in this study. The airway lead is a nominated anaesthetist endorsed by the local anaesthesia department director whose roles include ensuring airway equipment availability and procurement, liaising with ICU and ED, and auditing local airway practices. The leads are organised into the airway lead network at a state and national level to promote safe airway practices Australia-wide. 16 This method of sampling was chosen for the advantage of ready access to expert participants with a mandate to engage in safety research and access to a wide cross-section of health services.
The Victorian ANZCA Airway Lead Committee comprised one member from each major hospital and the past chairs of the ANZCA Airway Management Special Interest Group. The invitation to participate in the audit was sent to all Victoria’s ANZCA Airway Lead Committee members via the Whatsapp (Menlo Park, California, USA, www.whatsapp.com) message service, with a link to the questionnaire. A total of 26 members of the committee were present in the messaging group, which included two members from Tasmania and South Australia. The questionnaire remained open from 8 March to 30 April 2023, and a fortnightly reminder message was sent out after the initial invitation.
Ethical considerations
Ethical approval was obtained from the Cabrini Hospital’s Human Research and Ethics Committee (approval CHREC 05-01-03-23). Participation was voluntary.
Data entry
The audit questionnaire was entered into Qualtrics XM (Qualtrics, Seattle, WA, USA) by the data collector at each hospital site. A summary is attached in Table 1. All 168 data points were addressed by the data collector for each DAT within the OT. This was done directly into the online platform while inspecting the DAT. Each site audited one DAT within their OT.
Summary of audit questions.
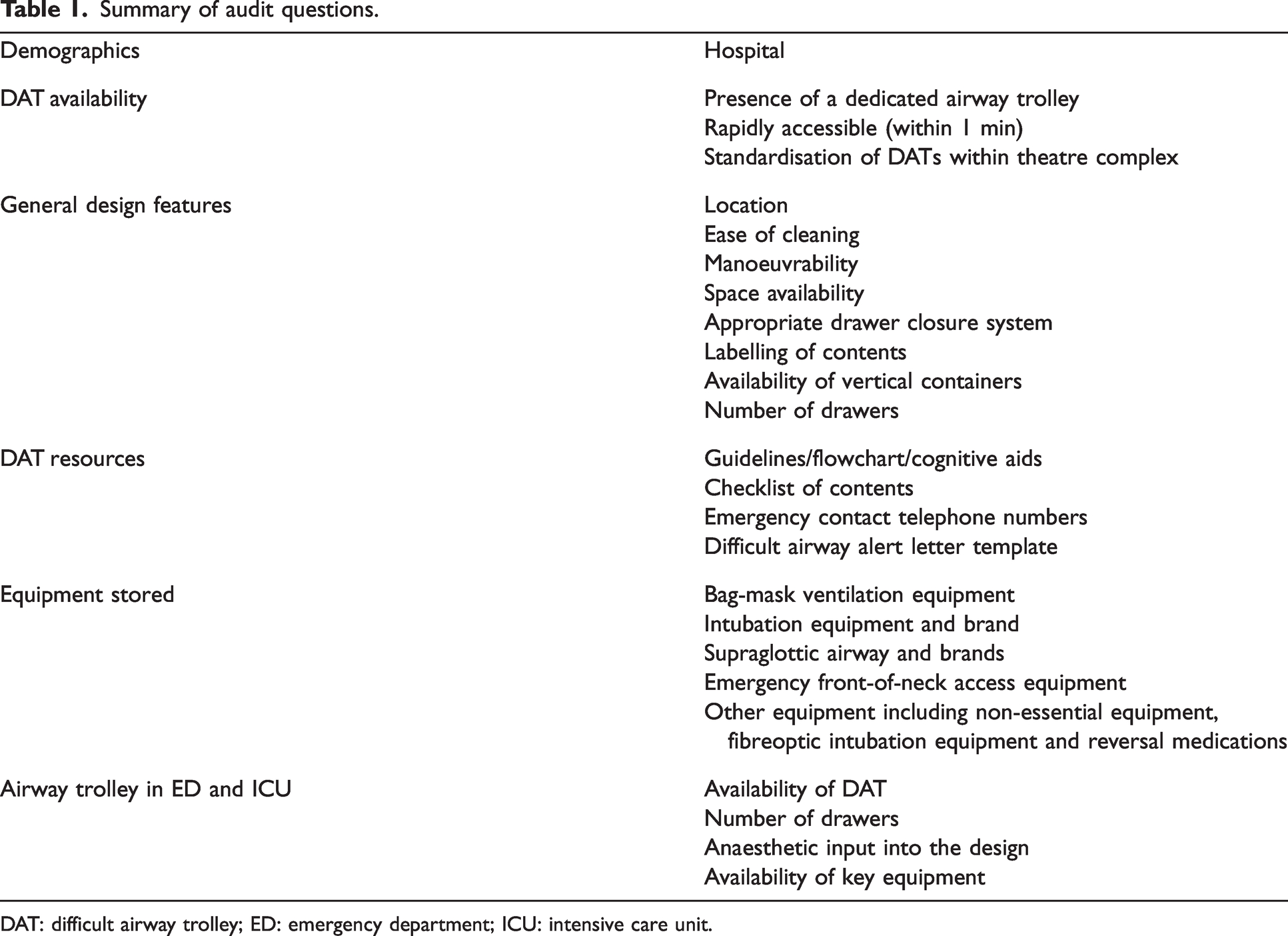
DAT: difficult airway trolley; ED: emergency department; ICU: intensive care unit.
Hospitals that participated in the audit.
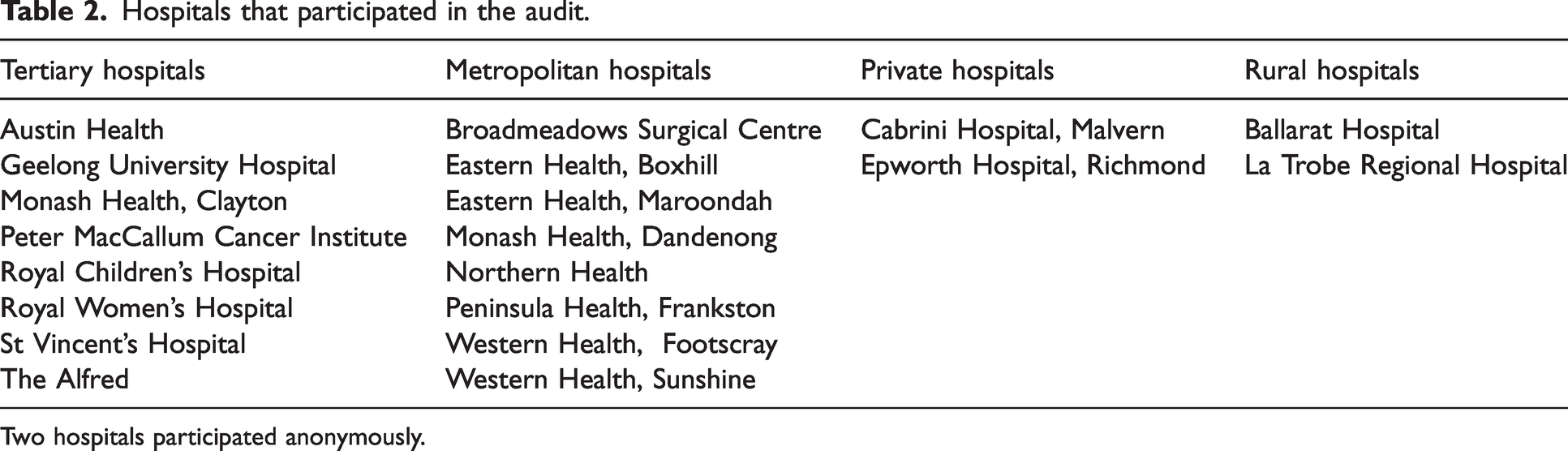
Two hospitals participated anonymously.
Compliance with overall design features, difficult airway trolley resources and type of cognitive aid available.
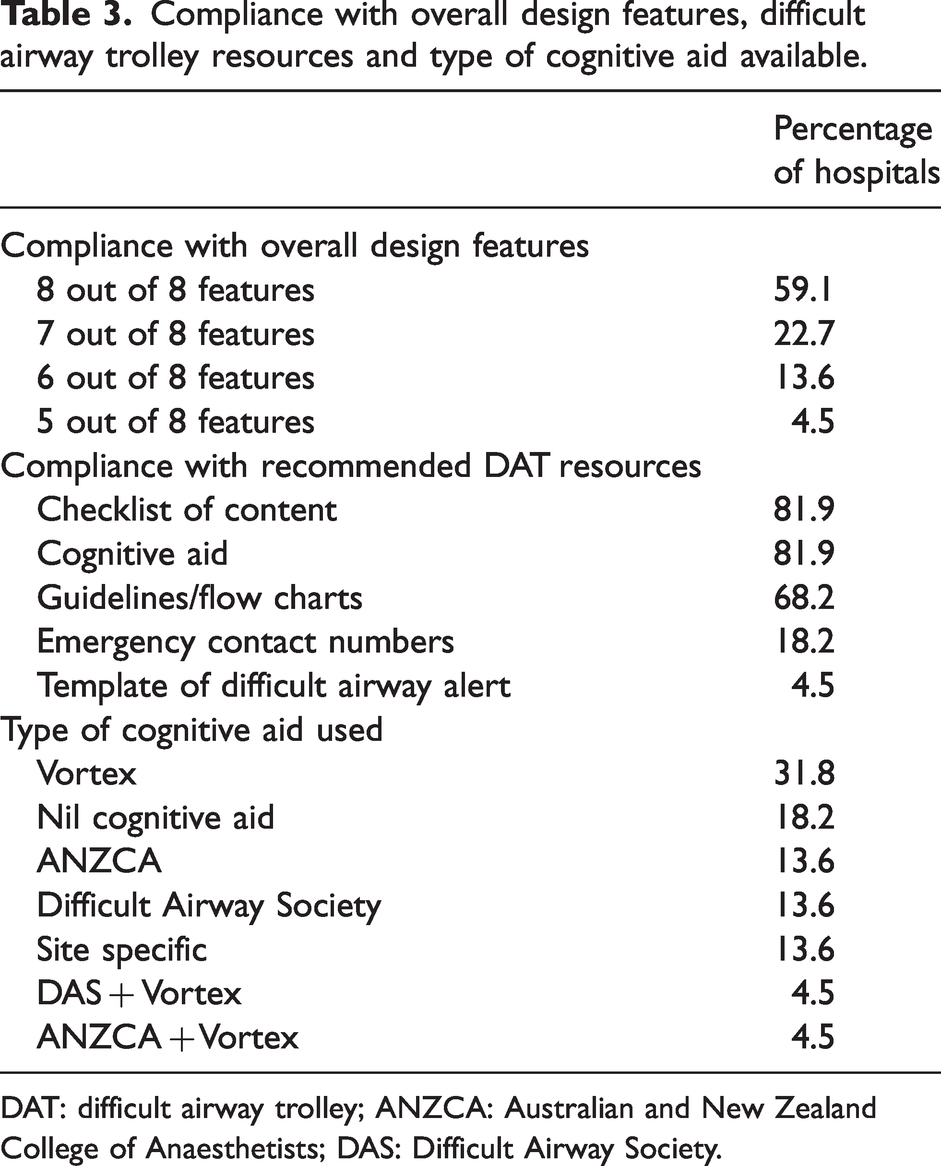
DAT: difficult airway trolley; ANZCA: Australian and New Zealand College of Anaesthetists; DAS: Difficult Airway Society.
Variation in key equipment brands carried.
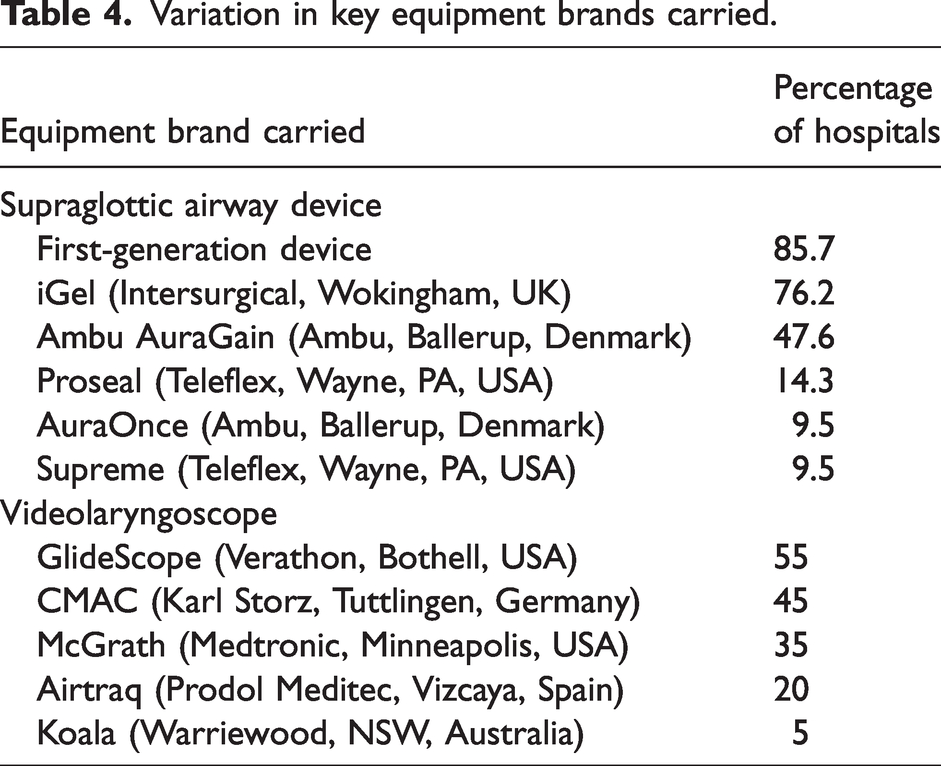
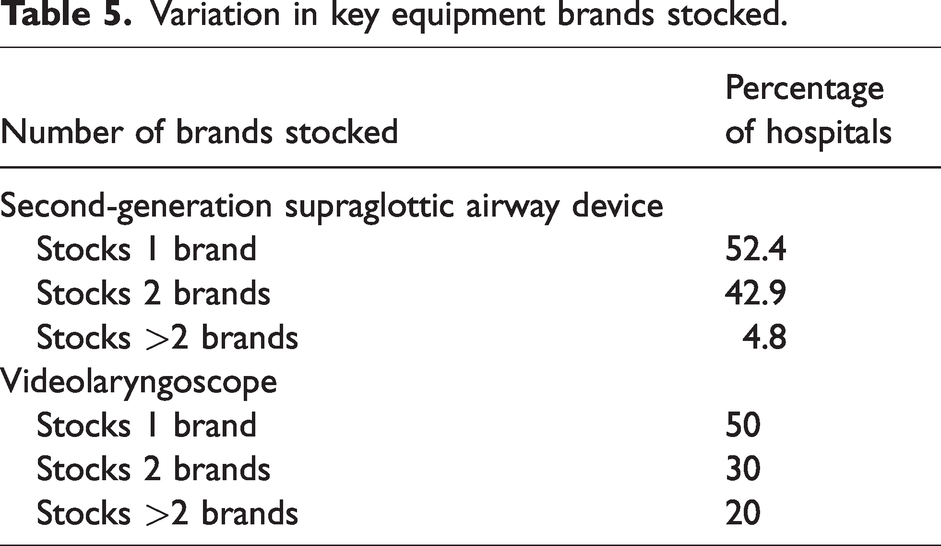
Variation in key equipment brands stocked.
Degree of standardisation with emergency department and intensive care unit difficult airway trolleys.
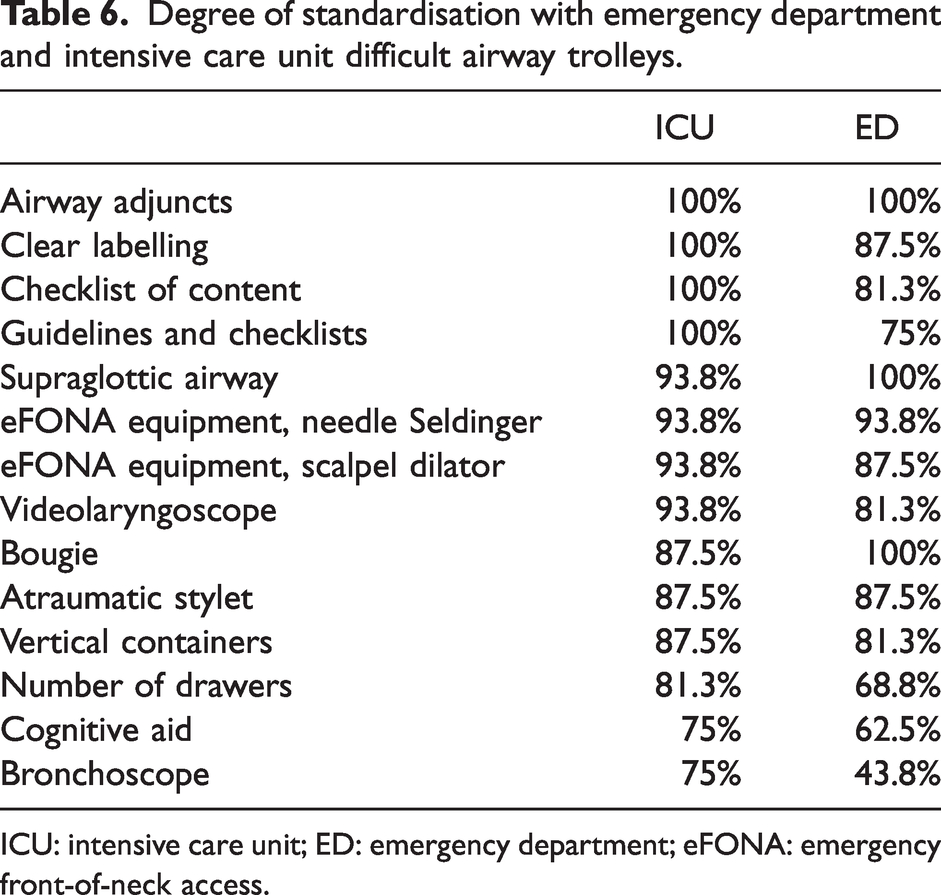
ICU: intensive care unit; ED: emergency department; eFONA: emergency front-of-neck access.
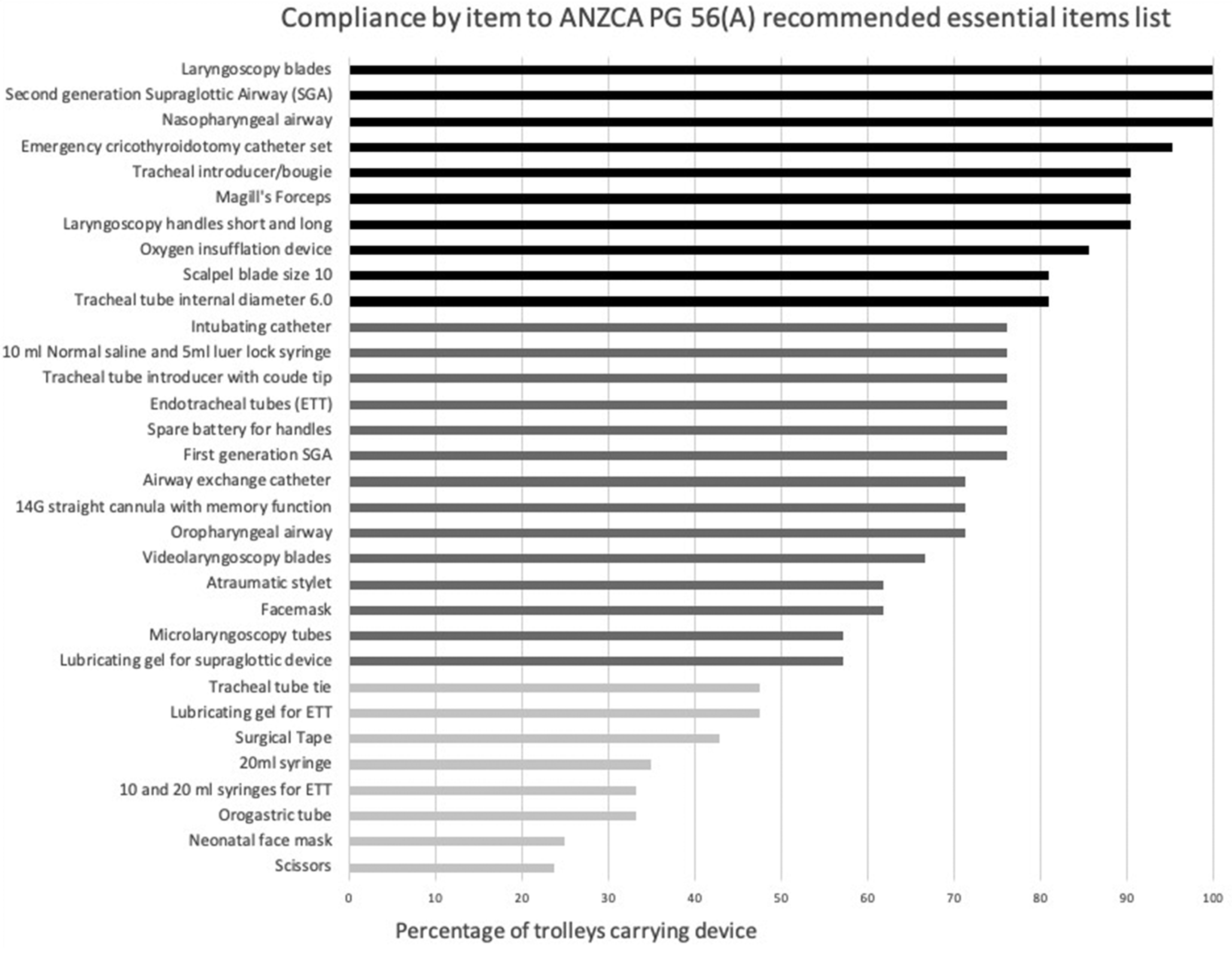
Percentage of difficult airway trolleys carrying essential equipment. A total of 21 hospitals were included in this analysis. Black indicates carriage by over 80% of trolleys, dark grey 50–79%, light grey less than 50%.
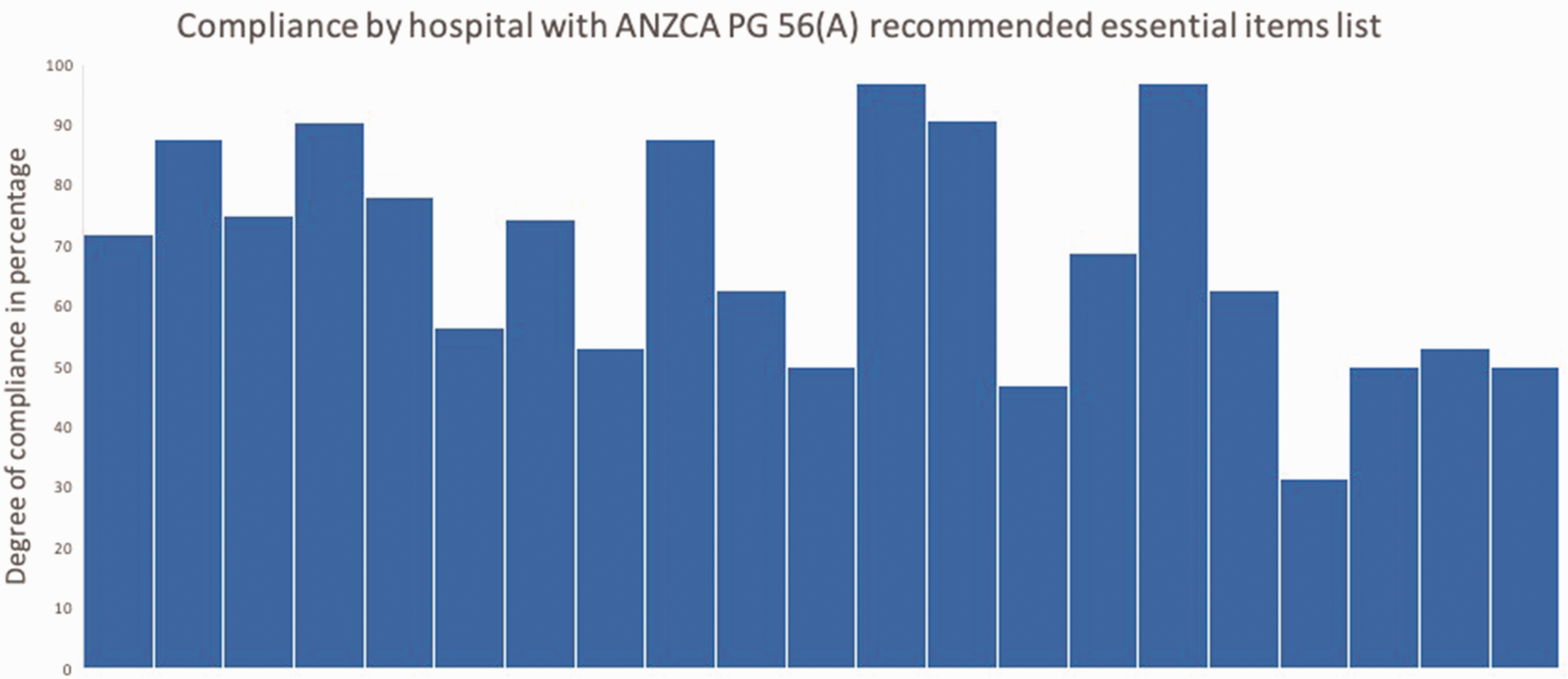
Compliance by the hospital. A total of 21 hospitals were included in this analysis. Each bar represents percentage of compliance with the ANZCA PG56(A) essential equipment list for a single hospital included in the analysis.
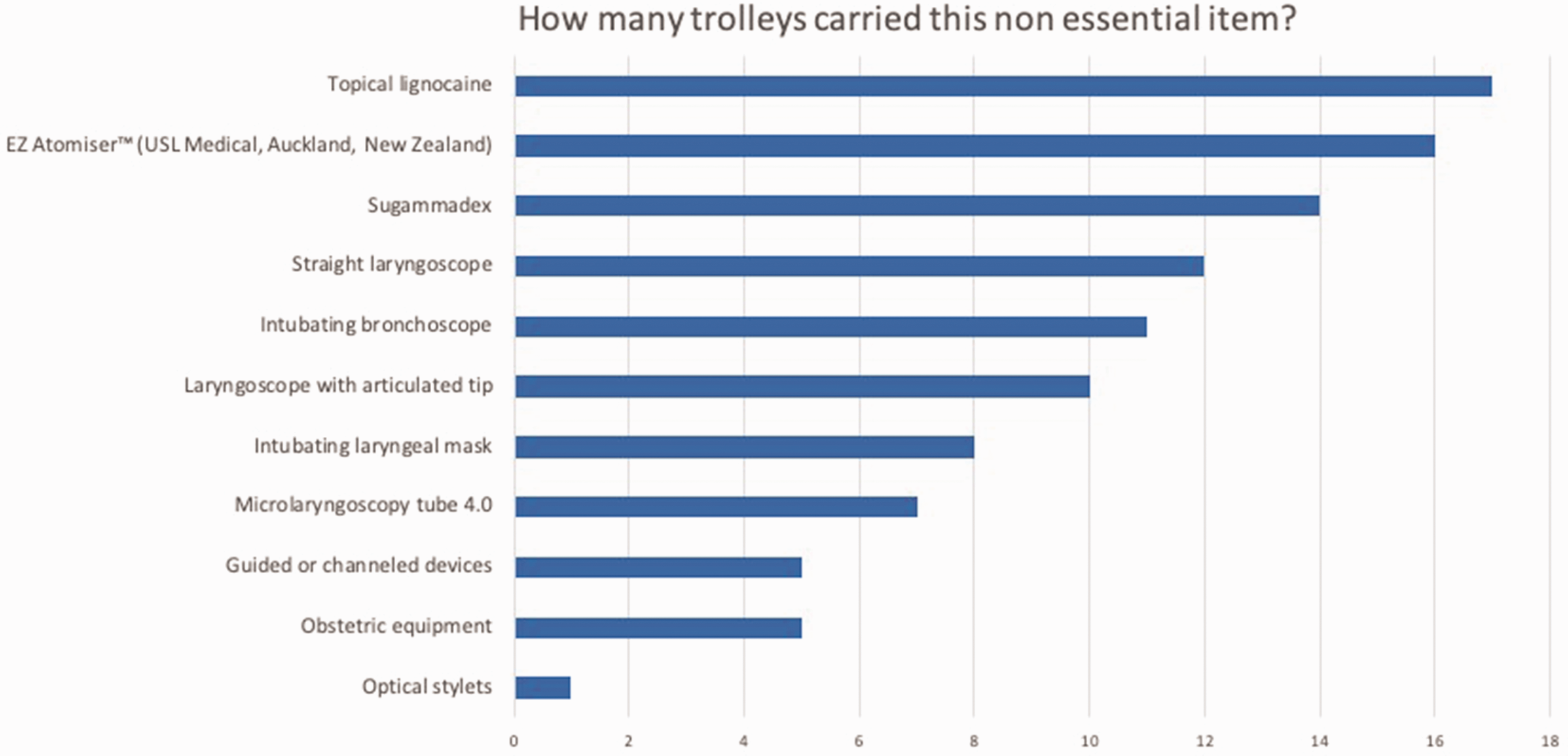
ANZCA PG56(A) listed non-essential items in difficult airway trolleys by popularity. Most of the 21 trolleys included in the analysis carried at least one item of non-essential equipment. On average, difficult airway trolleys carried four non-essential items, with some carrying up to eight.
Statistical analysis
Audit responses were exported from Qualtrics and analysed using Microsoft Excel (Washington, USA). The data analysis was predominantly descriptive and reported as percentages of positive responses. When applicable, a paired t-test was used to compare data sets. Missing data points were automatically assigned ‘no’ to minimise bias. We set the threshold compliance rate for essential items and design features at 80%, in line with national audit standards set by the Australian Safety and Quality Commission in Healthcare. 17
Results
A total of 24 airway leads responded from a possible 26, giving a participation rate of 92.3% (Table 2). Twenty-four hospitals audited a single DAT within their hospital’s OT. Of the 24 respondents, two were from interstate hospitals and their data set was excluded from all sections of the analysis. A total of 22 Victorian hospitals responded. Twenty-one were included in the analysis of trolley content. The Royal Children’s Hospital was excluded here because audit of trolley content was based on adult ‘essential equipment’ recommendations of the ANZCA PG56(A), which differ from paediatric recommendations.
Availability of the DAT
Of the 22 hospitals included in the analysis, 100% of OTs, EDs and ICUs had a DAT. The degree of standardisation within the OT complex was 100% for the hospitals. Eighty-six percent of respondents stated their DAT was rapidly deployable (within one minute).
We found the average compliance rate with the ANZCA PG56(A) essential equipment list in our sample to be 68.3%. Six hospitals met our compliance benchmark of 80%. Five hospitals demonstrated compliance of 50% or below. There were no significant differences between major tertiary centres and other hospitals in the compliance rate (P = 0.33).
Degree of standardisation in ED and ICU DATs
A total of 16 committee members provided data on the degree of standardisation between trolleys outside the OT with those inside the OT (Table 6). Anaesthetic input into the DAT setup within the ED was reported by 85.7% of hospitals compared with 81% reporting anaesthetic input into the DAT within the ICU. Across the domains of design and equipment we assessed, the ICU DATs reported a greater level of standardisation (P < 0.05) with the DAT in the OT (78.8%) than those from the ED (71.2%).
Discussion
This study demonstrated that DATs were available across the OT, ED and ICU in all hospitals audited, with particularly high ease of access in the OT. Compliance with ANZCA’s recommended design features and recommended resources was high (Table 3). Significantly better compliance with DAT recommendations was found compared with a smaller audit 10 years ago, when only 43% of audited sites had a dedicated DAT. 8 More than 80% of DATs in the current audit had at least one cognitive aid attached, compared with only 53.3% in a recent audit of Northern Territory DATs. 18
Average DAT compliance with all ANZCA-prescribed items was 68.3%. Only six hospitals stored greater than 80% of the ‘essential items’ (Figure 2). Most items with a poor rate of storage were ancillary equipment (that is ubiquitous in the OT environment), such as scissors (24%), syringes (35%) and surgical tape (43%). One exception was the neonatal face mask, recommended for ventilation via the tracheostomy stoma, for which the carriage rate was only 25%. Compliance with second and third-line rescue devices was relatively high, with greater than 80% of trolleys carrying laryngoscope blades and handles of all recommended sizes, first and second-generation SADs, a scalpel, size 6.0 endotracheal tube, emergency cricothyroidotomy equipment and an oxygen insufflation set (Figure 1).
Surprisingly low carriage rates were reported for oropharyngeal airway sizes 7 to 11 cm (71.4%), face masks of all PG56(A)-recommended sizes (61%), and videolaryngoscope blades of all sizes (66.6%) (Figure 1). This may be due to the questionnaire intentionally not distinguishing between non-carriage and incomplete sizing, our rationale being that extremes of size contribute to airway difficulty. 19 Second, theatres may keep some equipment separate from the DAT, such as the videolaryngoscope, due to their increased usage and footprint. Disappointingly, difficult airway letters for patients were especially underutilised in the DATs, with just a 4.5% carriage rate demonstrated, even though they are a highly effective and reliable method of disseminating critical airway information, 20 and are available in a Victorian Department of Health standardised format utilising the Queensland difficult airway alert letter template. 21
In terms of non-essential items, there were several findings of note. First, fewer non-essential items are now carried on the DAT, reflecting the simplification of content and reduction of clutter, consistent with current consensus.6,22 However, we found a considerable number of hospitals (36%) still carried items no longer recommended by the ANZCA PG56(A) guideline, notably intubating laryngeal masks. In addition, the most popular items outside of the prescribed list were the EZ 100 Atomizer(USL Medical, Auckland, New Zealand), topical lidocaine and sugammadex, and most hospitals carried these items (Figure 3). This we believe reflects a design trend of DATs in Victoria towards the more generalised use as a comprehensive trolley to cater to the vast majority of difficult airway situations rather than the more minimalist and focused ‘rescue’ trolley. 6
Five different videolaryngoscope brands were stored within the audited DATs, the most popular being Glidescope (Verathon, Bothell, USA) and C-MAC(Karl Storz, Tuttlingen, Germany), followed closely by McGrath(Medtronic, Minneapolis, USA) (Table 4). Evidence regarding the best videolaryngoscope for difficult airway scenarios is heterogenous but likely changes with individual clinician familiarity and experience.14,23 While some studies recommend stocking multiple brands to account for this, others argue for research and clinician education on the ‘best single device’ to avoid over-cluttering.14,24
We also identified a significant level of heterogeneity in DAT layout and equipment type carried (Tables 4 and 5). All DATs had between four and seven drawers. This was consistent with ANZCA’s recommendation, which prefers that four of the drawers are standardised for rescue techniques: facemasks, SADs, endotracheal intubation, and front-of-neck access. There was significant variation in videolaryngoscopes and SADs, as well as a wide array of cognitive aids. There is increasing consensus that the ideal DAT should be organised in a manner that serves as an extension of a specific airway management algorithm to facilitate rapid access to relevant equipment in high-stress situations.6,22,25 While the ANZCA PG56(A) recommends a consultative approach with local expertise, VMO anaesthetists work across multiple institutions.9,11 Therefore, we identified current variations in equipment, trolley structure, and cognitive aids as a safety risk.
Our data suggest a high level of standardisation within OT DATs in Victoria (Table 6). It also demonstrates a high level of consistency between OTs, EDs and ICUs, with over 80% of anaesthetic departments surveyed having input into their ED and ICU DATs. Within our criteria, there was a high standardisation between OT, ED, and ICU DATs. The ICU trolleys were designed more similarly to OT trolleys than ED trolleys, which could be accounted for by the better availability of bronchoscopy.
This study is a comprehensive questionnaire-based audit of the difficult airway trolley with a high participation rate (more than 90%) and inclusion of 22 major hospitals. This was the first study to delineate DAT design, resources, equipment compliance, standardisation, and heterogeneity across the state. Our use of a non-probabilistic sampling method theoretically limits the generalisability of the results. However, the sample of hospitals audited was comprehensive, and we believe that our findings are likely to be reflective of DATs across Victoria. Limitations inherent to our study design include reliance on participant self-reporting and recall, both of which are prone to bias. Data entry errors may also have occurred while completing the audit. Rural and private hospitals are under-represented in our study, thus limiting the applicability of our conclusions to smaller hospitals or other health centres. However, we believe there may be high generalisability to other Australian hospitals with a similar profile to our study participants.
This study found improved compliance with the ANZCA PG56(A) guideline with respect to the availability of the DAT, as well as its design, contents, and standardisation across locations within each hospital audited. There seems to have been significant improvement within the past 10 years if our findings can be extrapolated to previous Australian and New Zealand audits. This is possibly due to increased awareness of the need for better airway management from concerted efforts of the Victorian ANZCA Airway Lead Network, and multidisciplinary input into difficult airway guidelines such as the ANZCA PG56(A).
Supplemental Material
sj-pdf-1-aic-10.1177_0310057X241265722 - Supplemental material for A comprehensive audit of difficult airway trolleys in selected Victorian hospitals
Supplemental material, sj-pdf-1-aic-10.1177_0310057X241265722 for A comprehensive audit of difficult airway trolleys in selected Victorian hospitals by Yaodong Tang, Teresa Pham, William PL Bradley, and Fiona M Brewster and David J Brewster in Anaesthesia and Intensive Care
Footnotes
Author Contribution(s)
Acknowledgements
The author(s) would like to acknowledge the ANZCA airway leads of Victoria who helped complete the data entry.
Declaration of conflicting interests
Pierre Bradley was a co-author of the latest ANZCA PG56(A) guideline. Both David Brewster and Pierre Bradley are members of the Victorian ANZCA Airway Lead Committee. No other competing interests are declared.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.