
Abstract
Oesophageal intubations are more common than may be realised and can potentially cause significant patient harm even if promptly identified and corrected. Reports of morbidity due to unrecognised oesophageal intubation continue to present in coroner and media reports. Therefore, it would be helpful to identify mechanisms to prevent these events and implement strategies to avoid and identify incorrect endotracheal tube placement. This analysis of oesophageal intubations reported to webAIRS aims to provide an in-depth analysis of all events in which oesophageal intubation occurred. WebAIRS is a web-based, bi-national incident reporting system collecting voluntarily reported anaesthetic events across Australia and New Zealand, with more than 10,500 incidents registered. A structured search through the webAIRS database identified 109 reports of oesophageal intubation reported between July 2009 and September 2022. A common cause of oesophageal intubation was the misidentification of the larynx due to a poor laryngeal view. Desaturation directly attributed to the misplaced endotracheal tube occurred in 43% of all reports. The authors precisely defined early recognised oesophageal intubation and delayed or unrecognised oesophageal intubation. Most reports (74%) described early recognition of the misplaced intubation, of which 27% led to directly contributed to hypoxia. Cardiovascular collapse as a direct consequence of the late recognition of oesophageal intubation was described in five (18%) of these events. There was inconsistency in end-tidal carbon dioxide monitoring and interpretation of the resulting waveform. Findings show that oesophageal intubation continues to be an issue in anaesthesia. Incidents described confusion in diagnosis, human factors issues and cognitive bias. Clear diagnostic guidance and treatment strategies are required to be developed, tested and implemented.
Keywords
Introduction
Oesophageal intubations are more common than may be realised, with findings from a recent study reporting the incidence of these events to be one in every 18 emergency intubations. 1 Even when promptly recognised, oesophageal intubation is not benign; it has been linked to increased rates of severe hypoxaemia, pulmonary aspiration and cardiac arrest. 2 There are also reports of rupture of the stomach and damage to the oesophagus.3,4
Despite increased awareness, routine use of equipment to detect oesophageal intubation and the development of best-practice guidelines, there are still reports of patient morbidity and mortality due to late or unrecognised oesophageal intubation.3,5 This preventable cause of patient harm continues to occur, even in the hands of experienced anaesthetists, 3 and thus warrants all efforts in training, preparation and protocol to reduce it to a ‘never event’.
While patient harm due to oesophageal intubations was a common theme in the first Australian incident reports, it is unknown if they are still an ongoing issue in Australian and New Zealand anaesthetic care. 6 Recently developed consensus guidelines from the Project for Universal Airway Management group (PUMA) defined unrecognised oesophageal intubation as the unintended placement or migration of a tracheal tube into the oesophagus that is not promptly identified and addressed. 3 The authors of the guidelines have not defined a timeframe or marker for ‘promptly’ recognised versus ‘unrecognised’ oesophageal intubations. Designs for cognitive reminders have been developed;3,7 however, these have not been tested for their ability to reduce or eliminate oesophageal intubations, nor for their ability to facilitate better recognition and response times for when these instances occur.
With ongoing reports of unfortunate patient outcomes, it is essential to identify mechanisms that prevent oesophageal intubation, develop strategies to identify oesophageal intubations when they occur immediately and ensure available guidelines are true to life and followed.
WebAIRS is a web-based anaesthetic incident recording system used voluntarily by anaesthetists in Australia and New Zealand to report de-identified adverse events.8,9 Since 2009, more than 10,500 incidents in anaesthetic practice across Australia and New Zealand have been collected. The interrogation of such an extensive bi-national database provides an exciting opportunity to identify a larger number of otherwise rare adverse events, thereby providing the opportunity to share learning points from a vast collection of reports and learn from the experiences of our colleagues.
This analysis of oesophageal intubations reported to webAIRS aims to provide an in-depth analysis of all events in which oesophageal intubation occurred. Immediately recognised and delayed or unrecognised oesophageal intubations are clearly defined and analysed separately.
Methods
The functionality of the webAIRS system has been described in previous articles.8,9 In brief, basic demographic data, and narrative descriptions of the incident are reported in non-mandatory comment boxes and data tick boxes by anaesthetists who have been involved in a procedure in which an incident or near miss episode was experienced.
In this study, all incidents coded in webAIRS as an oesophageal intubation were reviewed. All incidents that appeared in a structure query language (SQL) search for the partial words ‘oesoph’ or ‘esoph’ and ‘intub’ were also evaluated for eligibility, and included if they described an oesophageal intubation.
The authors clearly defined immediate and delayed recognition of oesophageal intubation before commencing the detailed analysis. Included incidents were reviewed, categorised and investigated following the agreed definition.
Incidents were defined as an ‘immediately or early recognised oesophageal intubation’ when visualisation of the oesophageal intubation during the intubation attempt was described, or when oesophageal intubation was promptly noticed by the absence of a capnography trace.
Incidents were categorised as ‘unrecognised or delayed recognition of oesophageal intubations’ when the placement of the endotracheal tube (ETT) into the oesophagus went unnoticed, leading to at least one of the following:
hypoxia or haemodynamic instability before the treating anaesthetist identified the incorrect placement; the anaesthetist having started therapy for a presumed differential diagnosis (e.g. bronchospasm); the anaesthetist having moved on from verifying ETT placement to the next stage of the anaesthetic (e.g. turning on automatic ventilation etc.); or when a different team recognised the oesophageal intubation.
All incidents that described an oesophageal intubation were imported into an Excel analysis sheet, and a deductive detailed narrative analysis was performed independently by two authors (YE, TPF). Key analysis points align with the recent expert consensus statement, 3 including the use of end tidal carbon dioxide (EtCO2) monitoring, the use of videolaryngoscopy, and removal of the ETT when oesophageal intubation was suspected. Qualitative elements of the recommendations regarding verbal communication were not included in the analysis.
The findings of both authors were compared. Any differences in the analysis were reviewed by both authors again, discussed in detail and a consensus reached based on their agreed opinion.
Duplicated cases and incidents that did not involve oesophageal intubation were excluded from the detailed analysis.
Ethical considerations
WebAIRS data collection complies with current ethics requirements for the collection of de-identified quality assurance data in Australia, as outlined by the National Health and Medical Research Council in 2014. In addition, ethics approval has been sought and obtained from two hospitals in Australia: the Royal Brisbane and Women’s Hospital Human Research Ethics Committee (HREC/11/QRBW/311) and the Nepean Blue Mountains local health district (HREC/12/NEPEAN/18). Ethics approval in New Zealand was obtained from the Health and Disability Ethics Committee (MEC/09/17/EXP). Reporters at each site must comply with local institutional approval requirements. The reports are de-identified, voluntary and protected by qualified privilege in both Australia and New Zealand.
Results
The final detailed analysis involved 109 reports of oesophageal intubation. The SQL narrative search identified 381 reports, of which 255 were excluded as they mentioned the search words in different contexts (e.g. food bolus in the oesophagus). During the deductive narrative analysis, another 16 reports that did not describe an oesophageal intubation and one duplicate were identified. These reports were excluded from the detailed analysis (Figure 1). Twelve of these reports were related to bronchospasm, in which the reporters initially thought oesophageal intubation caused the incident. All 12 reports described the use of EtCO2 monitoring; 10 noticed a lack of or unsustained EtCO2 readings, and the anaesthetist removed the endotracheal tube in all 12 events.
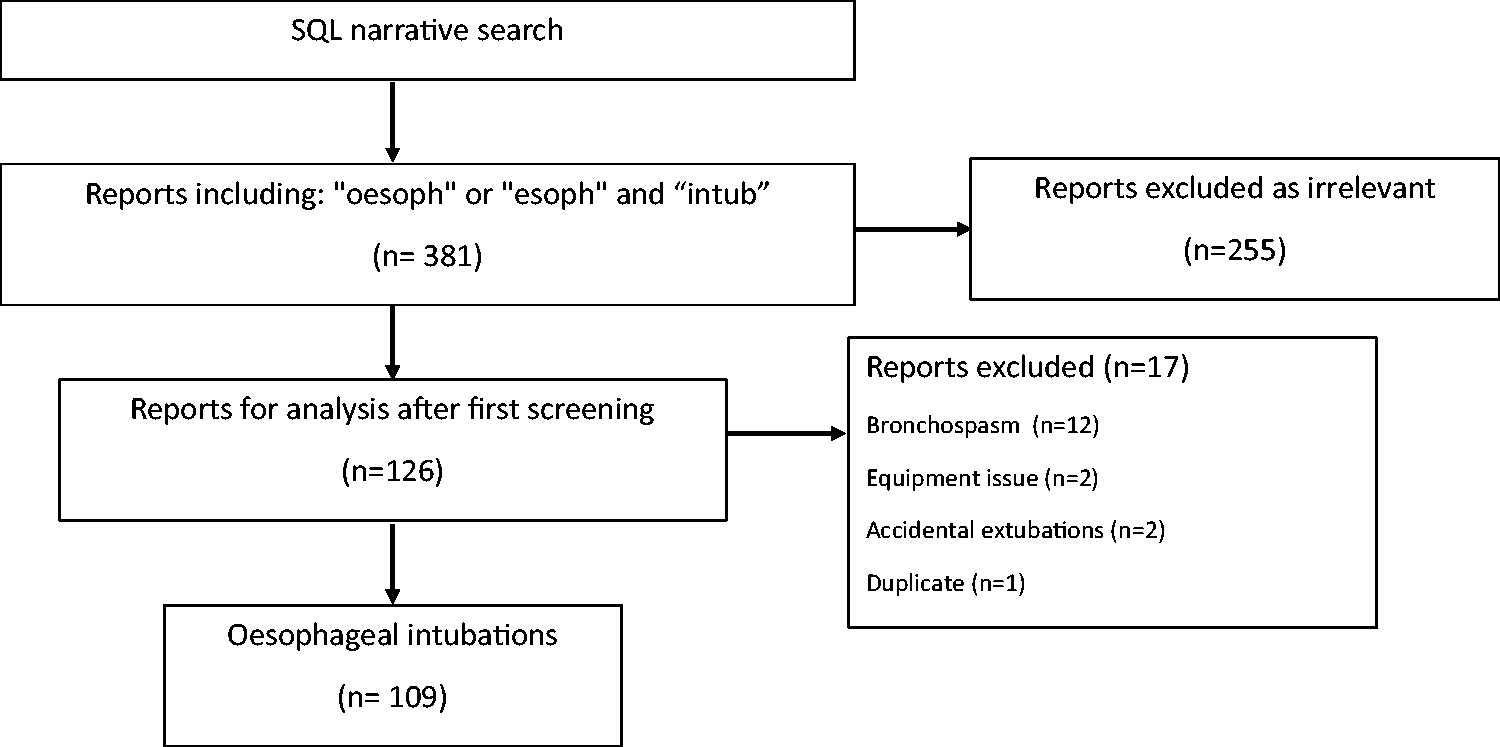
Search results. SQL: structured query language.
The reporters coded 25 of the 109 included incidents as oesophageal intubation; the remainder were coded in different webAIRS-specific subcategories, examples being difficult intubation, hypoxia, anaphylaxis, aspiration, laryngospasm, bronchospasm, or failed intubation.
Demographic data from the included incidents is represented in Table 1, and describes patients undergoing elective and emergency procedures across all ages, weight and American Society of Anesthesiologists Physical Status Classification ranges. The reporting anaesthetists considered more than half of the incidents preventable. Most oesophageal intubations occurred in operating theatres during daytime hours while under the care of a specialist anaesthetist. Nearly a quarter of the incidents involved patients undergoing general surgical procedures (Table 2).
Demographic data.
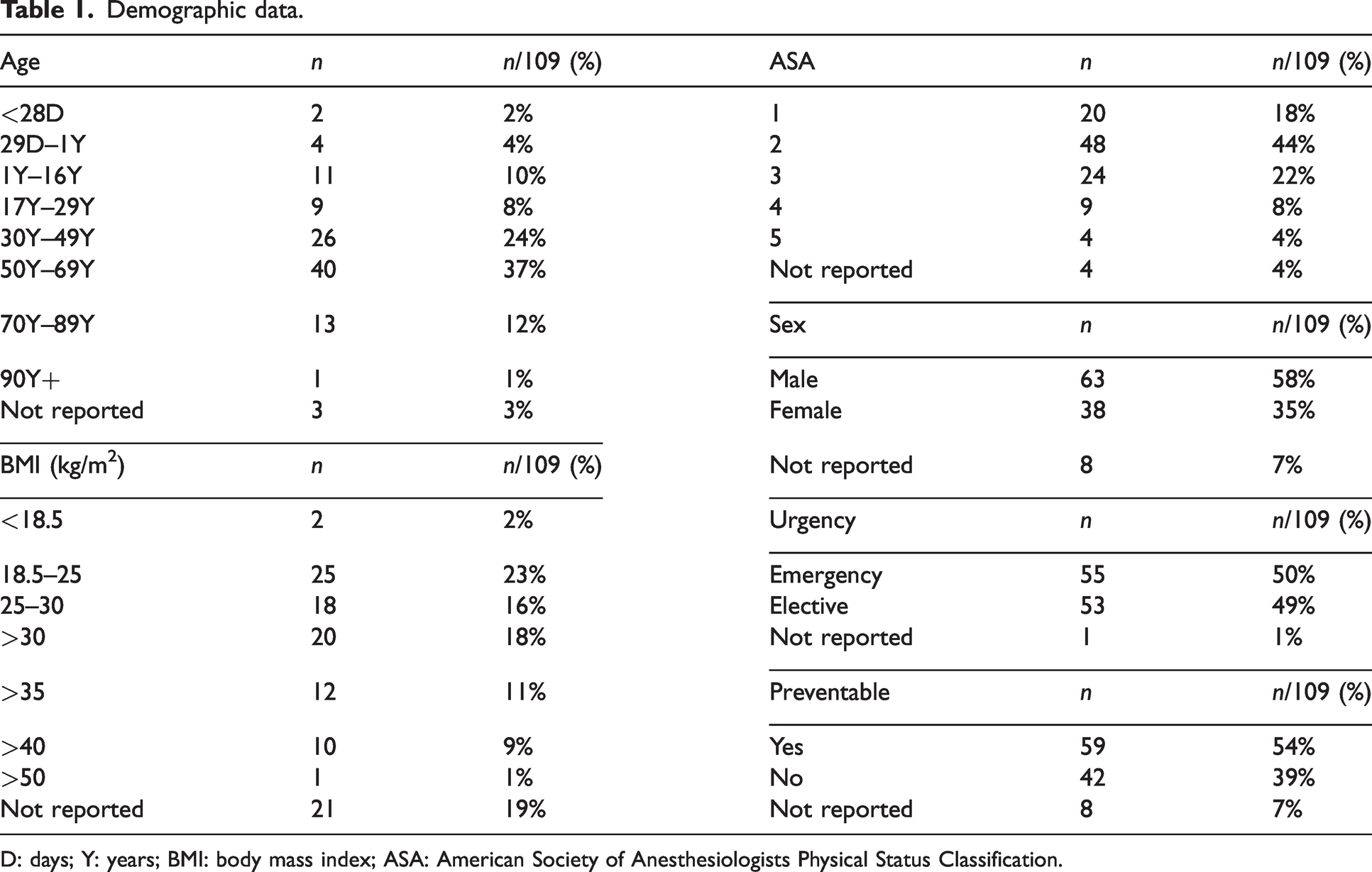
D: days; Y: years; BMI: body mass index; ASA: American Society of Anesthesiologists Physical Status Classification.
Surgical and anaesthetic data.
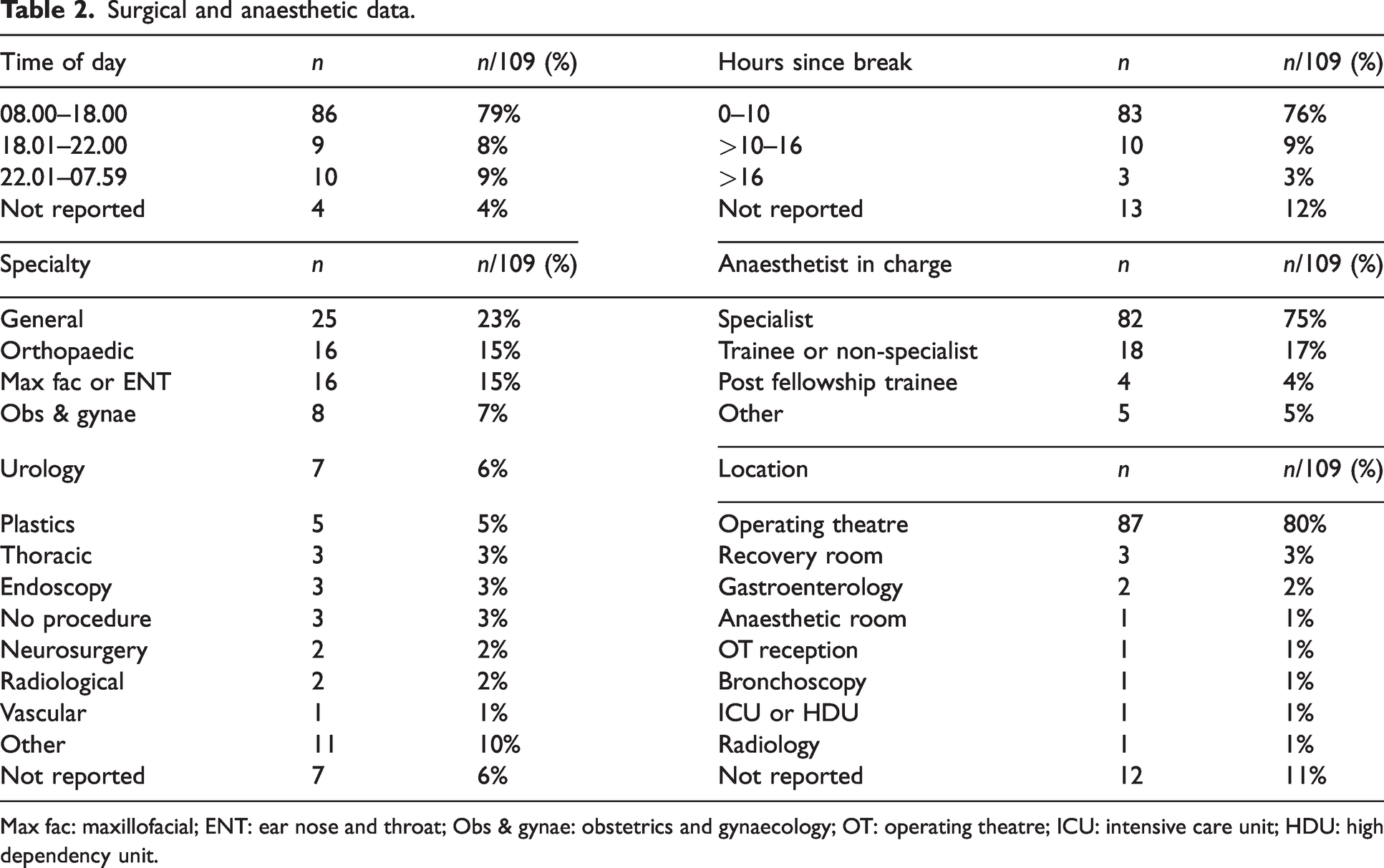
Max fac: maxillofacial; ENT: ear nose and throat; Obs & gynae: obstetrics and gynaecology; OT: operating theatre; ICU: intensive care unit; HDU: high dependency unit.
A common cause of oesophageal intubation was the misidentification of the larynx (n = 96, 88%), which was caused by poor laryngeal view in 47 (43%) of the incidents, by distorted anatomy or blood or vomit in the airway in 34 (31%) of the events, by limited operator experience in 28 (26%) of the reports or a combination of factors (Table 3). Technical delivery issues accounted for most of the oesophageal intubations (n = 108, 99%). These were incidents in which the endotracheal tube did not pass into the trachea (n = 99, 91%), due to misplacements of the bougie or flexible bronchoscope (n = 32, 29%) or during ‘blind’ intubation attempts without a view of the vocal cords (n = 21, 19%). Cricoid pressure was a contributing factor in 15 (14%) events, and cardiopulmonary resuscitation (CPR) during intubation was reported as a factor in four (4%) of the incidents. Many incidents described more than one cause for the delivery issues. Movement post intubation, causing oesophageal intubation, was described in nine (8%) incidents.
Causes of oesophageal intubation.
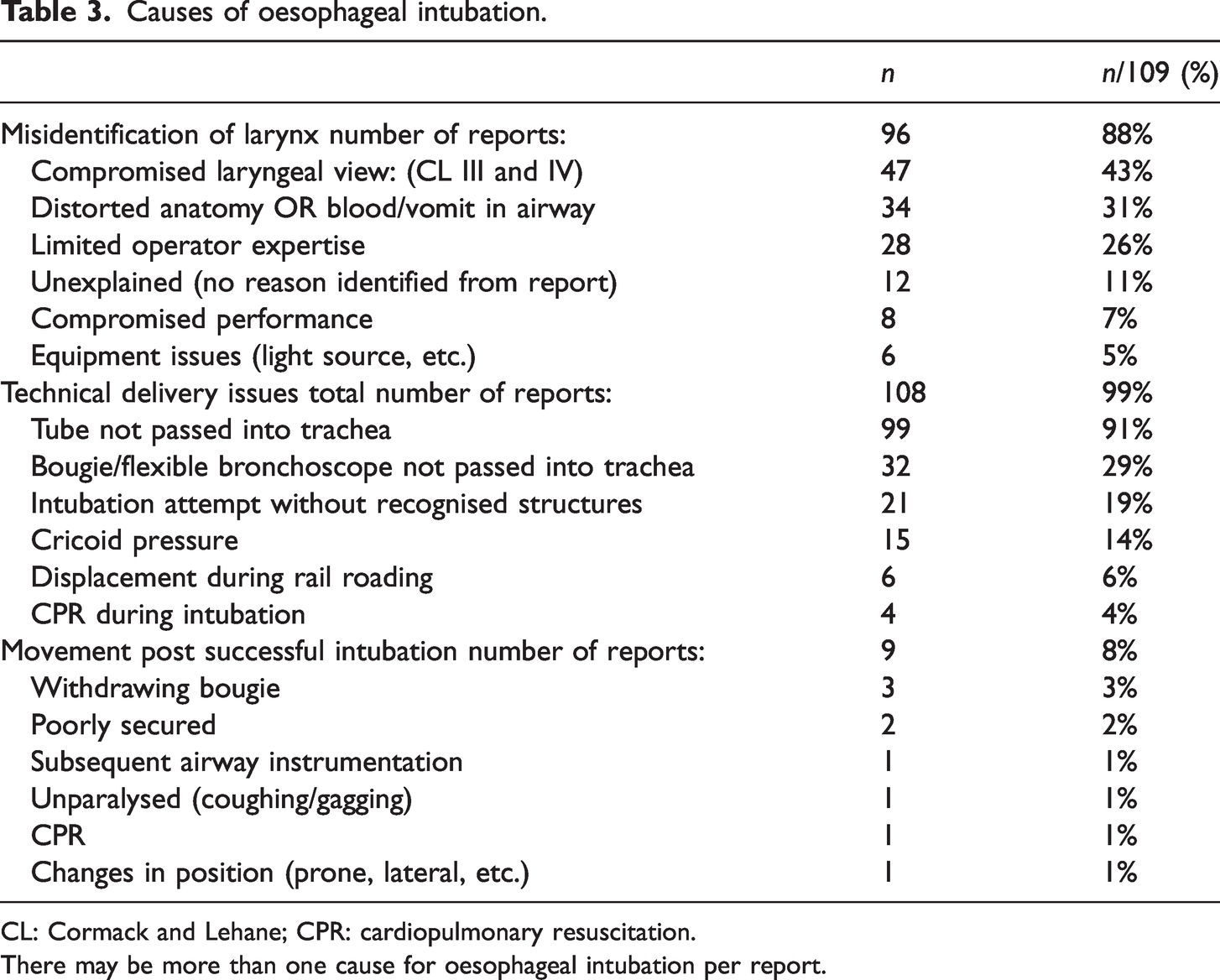
CL: Cormack and Lehane; CPR: cardiopulmonary resuscitation.
There may be more than one cause for oesophageal intubation per report.
The use of EtCO2 monitoring was either confirmed by a checkbox or described in the narratives in 102 (94%) incidents and not used in six (6%) incidents. These six incidents were all emergency intubations, two involved neonates, and one was a child under 4 years of age. Four incidents without EtCO2 monitoring occurred outside the operating theatre, either in the emergency department (ED) or intensive care unit (ICU).
One incident report did not provide information about the use of EtCO2 in their narrative or checkbox. Non-sustained EtCO2 was attributed to oesophageal intubation in roughly a third of the incidents. Only 16 incidents described the adherence to a minimum of four PUMA recommendations. Additional methods of diagnosing oesophageal intubation were mentioned in 41 (38%) incidents, with difficulty in ventilation and gastric distension reported most frequently.
Seventy-nine (72%) reporters described removing the endotracheal tube immediately when suspecting oesophageal intubation or lack of sustained EtCO2 was recognised, while five (5%) reporters described keeping the endotracheal tube in the oesophagus during subsequent airway management. The use of a videolaryngoscope during airway management was described in nearly half of all the incidents. A sub-analysis indicated that the use of videolaryngoscopy has increased since reporting to webAIRS had started in 2009, with 48 (44%) reports describing the use videolaryngoscopy before 2016 and 61 (56%) from 2016 onwards. In 33 (30%) of incidents oesophageal intubation occurred despite the use of a videolaryngoscope at the time of intubation.
A significant number of patients desaturated during the event and in 42 (39%) incidents, this was directly attributed to the oesophageal intubation. The authors described patient harm in half of all incidents (n = 54, 50%), defined as death (n = 4, 4%), unplanned admission to the ICU or high dependency unit (HDU) (n = 29, 27%), postponed or cancelled surgery (n = 9, 8%), prolonged hospital stay (n = 12, 11%), or iatrogenic injury or adverse events requiring additional treatments at the time of the incident (n = 26, 24%). Some patients experienced more than one event or significant injuries, even when the oesophageal intubation was recognised early.
Of the 109 included oesophageal intubations, 81 (74%) were identified immediately or early in the process, and 28 (26%) were delayed recognised or unrecognised oesophageal intubations.
Immediately or early recognised oesophageal intubations (n = 81)
Most reports of incidents that were categorised as early or immediate recognition of oesophageal intubation described using EtCO2 monitoring (n = 79, 98%). In 25 (31%) of these reports, the misplacement of the ETT occurred despite the use of videolaryngoscopy. The reporters mentioned the recognition of non-sustained EtCO2 in 26 (32%) events and removed the ETT in 64 (79%) when oesophageal intubation was suspected. A minimum of four PUMA recommendations were followed in 12 (15%) of these reports.
Additional indicators of a misplaced ETT were reported in 19 (23%) incidents and included a combination of various clinical assessments (Table 4). False confirmation of incorrect intubation by direct visualisation was described in two (2%) incidents and by fogging in the ETT in one (1%) incident.
Oesophageal intubation recognition.
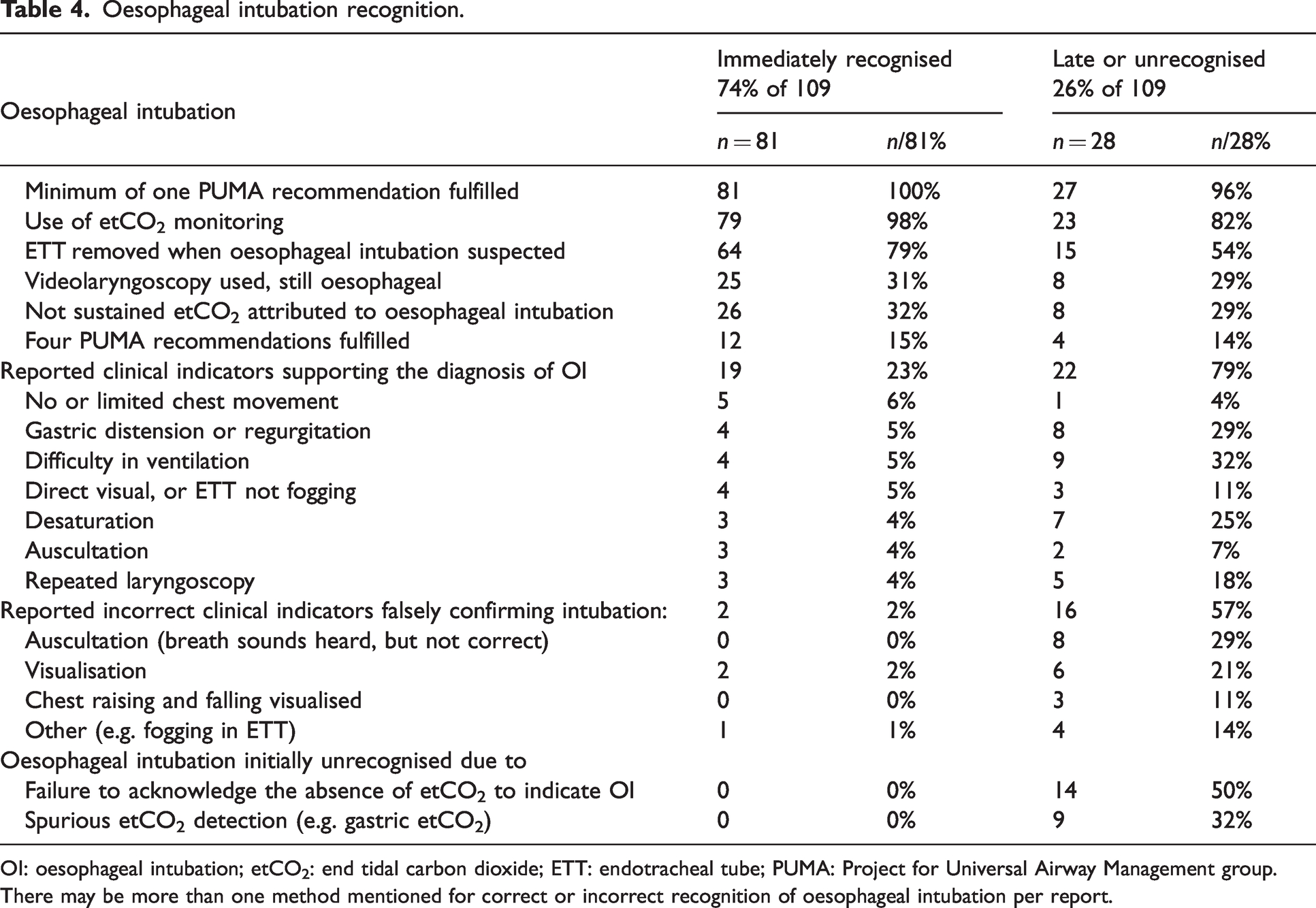
OI: oesophageal intubation; etCO2: end tidal carbon dioxide; ETT: endotracheal tube; PUMA: Project for Universal Airway Management group.
There may be more than one method mentioned for correct or incorrect recognition of oesophageal intubation per report.
Hypoxia directly attributed to the oesophageal intubation was reported in 22 (27%) of these events. Patient harm was described in 41 (51%) incidents, whereas in 39 (48%) there was no adverse effect on the patient, and patient outcome was not disclosed in one incident. Patient harm in this subgroup included a combination of ICU/HDU admission (n = 20), patient injury or other adverse events requiring additional treatment (n = 21), prolonged hospital stay (n = 5) and cancelled surgeries (n = 5). Three patients suffering from multiple comorbidities died.
Unrecognised or delayed recognition of oesophageal intubation (n = 28)
In this cohort, EtCO2 monitoring was mentioned in 23 (82%) reports and not used in five (18%). Videolaryngoscopy was used in nearly a quarter (n = 8, 24%) of the intubations which involved delayed recognition of oesophageal intubation. In half of the reports (n = 14, 50%) a failure to acknowledge the absence of EtCO2 to indicate a misplaced ETT was described. Spurious EtCO2 detection, falsely confirming correct intubation, was described in nine (32%) of the 28 incidents of unrecognised or delayed recognised oesophageal intubation. Auscultation (n = 8, 29%), direct visualisation of intubation (n = 6, 21%), chest rising and falling (n = 3) or fogging in the endotracheal tube (n = 4) were also described as clinical markers incorrectly indicating endotracheal intubation. On the other hand, in 22 (79%) of these incidents, a combination of clinical indicators, including desaturation (n = 7, 25%), difficulties in ventilation (n = 9, 32%), gastric distension (n = 8, 29%), repeated laryngoscopy (n = 5, 18%) supported the diagnosis of delayed oesophageal intubation.
Patient harm was described in 13 (46%) of the events, including ICU/HDU admission in six (21%) reports, cardiovascular collapse as a direct consequence of the late recognition of oesophageal intubation in five (18%) cases, prolonged length of hospital stay was mentioned in four reports, and surgery was cancelled in three. Hypoxia directly attributed to oesophageal intubation was mentioned in 20 (71%) reports, and one patient in this cohort died (Table 5).
Mentioned outcomes.
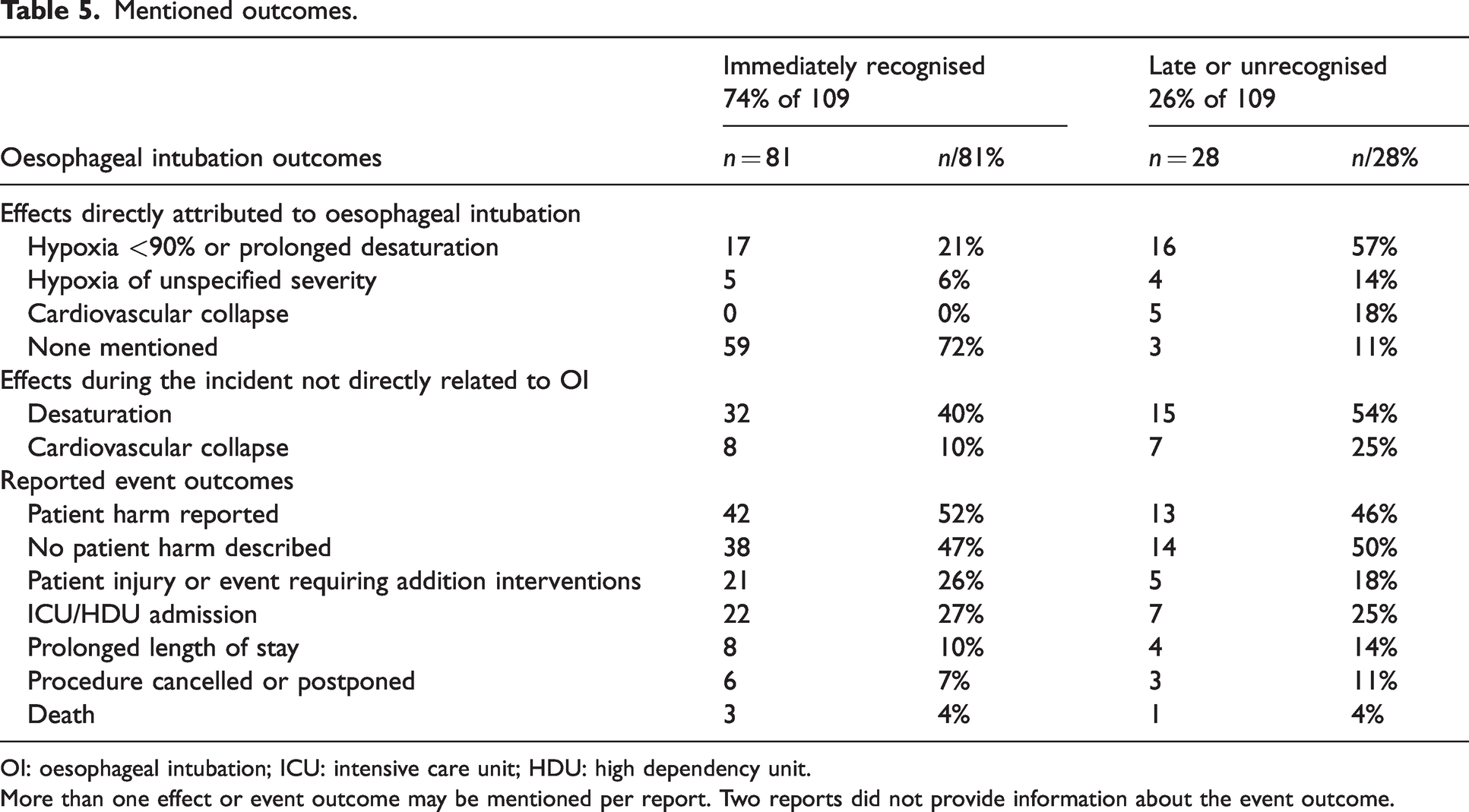
OI: oesophageal intubation; ICU: intensive care unit; HDU: high dependency unit.
More than one effect or event outcome may be mentioned per report. Two reports did not provide information about the event outcome.
Discussion
This analysis aimed to review and analyse oesophageal intubations reported to webAIRS and to cast light on some of the factors implicated in its occurrence, their management and influencing patient outcomes. The majority of the 109 oesophageal intubation events analysed in this study involved the misplacement of the ETT due to a poor laryngeal view. Even though most of the oesophageal intubations were recognised early in the process, the spectrum of complications arising from oesophageal intubation ranged from no harm to significant patient injury and mortality. Until recently, unrecognised oesophageal intubation had not been well defined. The absence of a clear definition adds to the challenge of investigating this type of event. The authors have defined recognised and unrecognised oesophageal intubation for this study and for future studies. While harm can result from immediately recognised oesophageal intubations (gastric insufflation, regurgitation, aspiration, oesophageal injury), until now, it has mainly been the unrecognised oesophageal intubations that were reported to be associated with substantial morbidity and mortality. The primary data source regarding these events was coroners’ reports and mainstream media publications. The frequency of these reports suggests that unrecognised oesophageal intubation is an ongoing and international problem. 3 Indeed, even its inclusion in the NHS Never Event list was brief, as this was rapidly suspended pending further clarification. As with other rare adverse severe events such as anaphylaxis or malignant hyperthermia, in which denominator data are absent, obtaining the actual frequency and relative risk of oesophageal intubation is challenging.
Recently developed consensus guidelines have provided several recommendations to reduce the occurrence of oesophageal intubation, improve the early recognition of oesophageal intubation, and create awareness of potential operator biases. 3 A number of these are discussed and linked to the findings of this analysis.
Strategies for the prevention of oesophageal intubation
Videolaryngoscopy
The authors of PUMA recommend the routine use of a videolaryngoscope wherever feasible to reduce the risk of oesophageal intubations. 3 The use of videolaryngoscopy for airway management has been mentioned in less than half of the reports, and included the routine use of videolaryngoscopy and videolaryngoscopy as a back-up device when attempts at conventional laryngoscopy failed. The low number of reports utilising videolaryngoscopy in this analysis may partly be explained by the lack of access to videolaryngoscopy for cases early in the data collection period (c. 2009). Reassuringly, there seems to be an upward trend in comparing the percentage of the reported use of videolaryngoscopy before 2016 (33%) with the use of videolaryngoscopy after 2016 (57%) in this cohort. The benefits of using videolaryngoscopy have been well described.16,17 Not only does its use improve the glottic view and reduces oesophageal intubation, but it also improves team dynamics, as all team members can view the intubation simultaneously. 3 Unfortunately, a significant number of incidents were reported in which the use of a videolaryngoscope was described, but nevertheless the ETT ended up in the oesophagus. These incidents serve as a reminder that oesophageal intubation might still occur despite the use of recommended advanced airway equipment. False reassurance of wrongly perceived correct intubation might lead to late recognition in some of these events.
Stepwise verbalisation of laryngoscopy
The recommendation is to verbally to mention and state each step of the laryngoscopy, encouraging the operator to acknowledge individual parts of the anatomy, and creating a shared mental model allowing the team to participate in the intubation. 3 The laryngeal view was described as difficult in many reports. Compromised laryngeal views, distorted anatomy, blood or vomit, or a combination of factors were mentioned in multiple events. Some of these led to attempted ‘blind intubations’, in which intubation was attempted without recognised anatomical structures. It needs to be tested if stepwise vocalising of the poor view would help to prevent oesophageal intubations in such instances. None of the reporters described verbalisation of the intubation process in their narratives. It is possible that this was simply not mentioned in the descriptions, or stepwise verbalisation might not yet be standard practice in Australian and New Zealand airway management.
Recognition of oesophageal intubation
EtCO2 monitoring
Anaesthesia has come a long way since the first Australian incident reports recommended using EtCO2 monitoring to avoid unrecognised oesophageal intubation. 6 The findings of the fourth National Audit Project (NAP 4) have also strongly recommended the use of EtCO2 monitoring in all instances of airway management. 2 Across Australia and New Zealand, the use of EtCO2 is mandated by the Australian and New Zealand Collage of Anaesthetists (ANZCA) requirements for anaesthetic monitoring. 7
While EtCO2 monitoring was described in most reports, there were six incidents in which no EtCO2 monitoring was used at some stage during airway management. Two of these incidents involved the airway management of neonates, which the scientific literature suggests has a high incidence of adverse events, even in experienced hands.10,11 Oesophageal intubation has been reported as a common complication.10,11 The paediatric and neonatal intensive care units (PIC-NIC) survey in the UK12,13 reported wide variation in neonatal intensive care practice, and found that the use of continuous waveform capnography in neonatal units in the UK has proved controversial, with some institutions using EtCO2 monitoring for all patients, while others believe that it is technically not possible. The incidents affecting neonates in this analysis all involved emergency airway resuscitation in which the anaesthetist had been called on to help paediatricians or ED doctors. One reporter specifically questioned the lack of monitoring on the operating theatre’s neonatal resuscitation trolley. The use of EtCO2 monitoring for confirmation of intubation and monitoring during ventilation of neonates in Australia and New Zealand may warrant further conversation and review.
‘No trace = wrong place’
The ‘no trace = wrong place’ campaign slogan promoted by the Royal College of Anaesthetists and the Difficult Airway Society 14 and adopted by ANZCA 7 aims to remind anaesthetists that the lack of EtCO2 indicates that oesophageal intubation is very likely. The authors of PUMA recommended that failure to satisfy the criteria for sustained exhaled carbon dioxide following passage of a tracheal tube requires oesophageal intubation to be actively excluded. 3 The default response should be to remove the ETT and attempt ventilation by way of the laryngeal mask or a facemask. In this analysis lack of sustained EtCO2 as an indicator of oesophageal intubation was mentioned in less than a third of the reports. The authors assume that some oesophageal intubations were recognised before ventilation started because most were reported as being recognised immediately or early in the process. In addition, the webAIRS narrative boxes are non-mandatory and voluntary, so it may be that some reporters did not mention non-sustained EtCO2, even though it might have been observed.
Immediate or early recognition of oesophageal intubation—EtCO2 monitoring
The overwhelming finding in this cohort is that nearly all of the reports describing immediately recognised oesophageal intubation used EtCO2 monitoring. A third of these noticed the lack of sustained EtCO2, and the majority removed the ETT when oesophageal intubation was suspected. Clinical indicators initially wrongly confirming correct intubation were only mentioned in three incidents, and reliance on additional methods to EtCO2 readings was mentioned in fewer reports (23%) compared with the incidents in which oesophageal intubation was not recognised or was recognised late (79%). All incidents described following at least one PUMA recommendation, but only a few reported following a minimum of four recommendations. It is possible that these were followed in a higher number of events but were not mentioned in the webAIRS narratives. Nevertheless, it is reassuring to note the successful application of etCO2 readings to the majority of immediately recognised oesophageal intubations, and the high number of reports describing the acknowledgement of unsustained etCO2 readings as an indicator of a misplaced ETT.
Unrecognised or delayed recognition of oesophageal intubation—EtCO2 monitoring
In five incidents, the lack of EtCO2 monitoring led to delayed recognition of oesophageal intubation. Two of these involved critically ill ICU patients. One of the reports described the unavailability of EtCO2 monitoring and the reliance on assessing breath sounds. Oesophageal intubation was recognised due to gastric distension, a decrease in oxygen saturation and difficulties in ventilation. The oesophageal intubation in the other ICU patient was only recognised due to the regurgitation of gastric contents in the ETT. This happened after the patient had already suffered from a cardiovascular collapse and CPR had been initiated. The progress of this patient is discussed in the section on deaths. The incident describing an unrecognised oesophageal intubation in the ED involved a child suffering from asthma. Again, significant desaturation finally led to the delayed recognition of oesophageal intubation after the team was initially wrongly reassured by identifying breath sounds. Two incidents of unrecognised oesophageal intubation happened in the operating theatre. In one incident EtCO2 monitoring was accidentally not connected, setting an important reminder for thorough pre-anaesthetic machine checks. The other one involved an unresponsive neonate after a caesarean section who required intubation during rescue attempts. Repeat laryngoscopy identified the misplaced tube after initially false reassurance of correct intubation by auscultation. Re-intubation, leading to successful ventilation, led to a positive outcome. These incidents serve as an important reminder of the necessity of EtCO2 in all areas where airway management might be performed. These incidents also describe the unreliability of clinical parameters in distinguishing endotracheal intubation from oesophageal intubation, leading to potentially catastrophic outcomes.
On the other hand, in 14 reports, the anaesthetist described the absence of EtCO2 readings in their narratives but did not immediately acknowledge that this might have indicated oesophageal intubation, leading to delayed recognition in each of the events. Many initially described false confirmation of intubation by different methods, including visualisation, auscultation, observation of chest movement or fogging in the ETT. Ten of these 14 events resulted in desaturation, and three patients suffered from a cardiovascular collapse as a direct consequence of the initially undetected oesophageal intubation. Potentially harmful unnecessary procedures were described, including a finger thoracotomy. Various cognitive biases that might lead to patient harm in airway management have been described in the literature.3,15 The reported incidents in this analysis provide a good example of possible confirmation bias, in which the operator focuses on information supporting the desired diagnosis while not considering a different diagnosis. 15
In nine reports, spurious detection of EtCO2 was described but not considered an oesophageal intubation by the reporters. The data submitted do not allow determining the quality of the trace, but it seems likely that these incidents describe events with initially false confirmation of the tube position. While a completely absent trace is highly specific for oesophageal intubation, an abnormal trace might be less explicit for some. In most of these events, bronchospasm was the working diagnosis until oesophageal intubation was identified. The authors of PUMA contribute similar events to another bias in anaesthetic airway management, described as ‘anchoring’, in which there is a focus on one diagnosis with hesitation to consider alternative diagnoses.3,15
Management of oesophageal intubation—removing ETT
Most reporters mentioned removing the ETT when oesophageal intubation was suspected. The ETT was not removed in five reports, and oxygenation attempts through the misplaced ETT continued, even though the reporters mentioned a lack of or spurious EtCO2 readings. This resulted in significant haemodynamic instability and hypoxia in three of these incidents, while the treating anaesthetist desired to rule out oesophageal intubation with other methods. Interestingly, in the other two events, the reporters described the conscious decision of leaving the ETT in the oesophagus as a conduit for regurgitated gastric content, thereby successfully avoiding aspiration in their patients. In both reports, the treating anaesthetist correctly identified the ETT as misplaced in the oesophagus and abandoned using it for ventilation, but found it very useful in preventing aspiration or airway soiling and thereby supporting subsequent tracheal intubation attempts. Leaving the ETT in the oesophagus during these intubation attempts also helped to prevent repeated oesophageal intubation.
Bronchospasm
There were 12 incidents of bronchospasm in which the treating anaesthetist attributed spurious or lack of EtCO2 readings to oesophageal intubation and consequently removed the ETT, as recommended by the guidelines. All these incidents were subsequently identified by both the reporters and the analysers as events of severe bronchospasm, some possibly anaphylaxis. Most patients suffered from significant hypoxia during the following airway management attempts, some required ICU admission, one front-of-neck access was described, and several surgeries had to be cancelled. While these incidents are excluded from the detailed analysis of oesophageal intubations, they describe an important conundrum. Causes of exhaled carbon dioxide detection despite oesophageal intubation are commonly described3,5 and mentioned in incident and closed claims analyses.5,6 However, severe bronchospasm causing a lack of exhaled EtCO2 readings are only mentioned anecdotally. 18 The authors of the PUMA consensus guidelines mention that severe bronchospasm is extremely unlikely to result in an inability to satisfy the criteria for sustained exhaled carbon dioxide. 3 Unfortunately, the information in the narratives does not provide details about the quality of the EtCO2 trace nor the number of ventilatory breaths attempted before ETT removal. As these types of incidents were not the main focus of this analysis and are incidental findings during the narrative analysis, more of these events may be described in the webAIRS database. A targeted webAIRS search and analysis of incidents in which bronchospasm was mistaken for oesophageal intubation and reported to webAIRS may follow in a future article, and will hopefully provide deeper insight.
Outcomes of oesophageal intubation
Significant harm due to oesophageal intubation despite immediate recognition
Two incidents of oesophageal injury were described in this cohort. Both times, the oesophageal intubation was recognised immediately and corrective measures taken. In one incident, a bougie as an aid for intubation was used. There was no evidence at the time of the event to suggest any airway or oesophageal trauma. However, a few days later, the patient was found to have subcutaneous emphysema and a mediastinal collection. Further investigations identified a significant oesophageal injury requiring extensive surgical repair leading to a prolonged hospital stay and potential permanent harm. The second incident described an oesophageal tear, probably caused by the oesophageal intubation with an ETT. Also, there were no indications of injury at the time of the event. The patient presented the next day with subcutaneous emphysema, requiring a feeding tube and further surgical management. It is essential to utilise strategies to avoid intubation-related iatrogenic oesophageal injuries, including using videolaryngoscopy to increase first-pass success. If a stylet is used, it is essential to ensure that the tip does not protrude beyond the edge of the endotracheal tube. Using a bougie requires gentle, skilful handling and immediate assessment of the bougie post-intubation to identify blood as an indicator for iatrogenic injury.
Haemodynamic instability due to unrecognised or delayed recognition of oesophageal intubation
Five reports described the delayed recognition of oesophageal intubation leading to directly attributed cardiovascular haemodynamic instability. The first one described an unwell premature neonate who was prepared for transport to a tertiary centre. During attempts to secure the airway, the oesophagus was intubated, leading to immediate significant bradycardia. Several factors were likely to have contributed to this haemodynamic instability, including prematurity, patient pathology and oesophageal intubation. Another reporter described ongoing EtCO2 readings of only a small height and small tidal volumes post intubation, assuming they were successful. The anaesthetist, who was teaching a medical student at the time, attributed the low readings to the significant hypotension post intubation until finally realising the ETT was misplaced. The third case described airway management in the ED, where the reporter noticed that EtCO2 readings were trailing off after intubation. This was initially thought to represent a decreasing cardiac output and managed as possible bronchospasm. Following the loss of cardiac output, a tension pneumothorax was assumed, leading to bilateral finger thoracostomies. The patient required CPR, until flexible bronchoscopy confirmed misplacement of the ETT in the oesophagus. Fortunately, resumption of spontaneous circulation occurred quickly after oxygenation, and the patient did not suffer any neurological sequelae at the time of reporting. The fourth report described oesophageal intubation by a junior doctor in an anticoagulated patient with a post-tonsillectomy bleed under consultant supervision. Both anaesthetists assumed that the placement of the ETT was correctly in the trachea and attributed the ventilation issues to a machine problem. They switched to a different ventilation device, which was more time-consuming than expected. The patient suffered significant hypoxia leading to bradycardia but recovered after ventilation was restored. The final report in this group of patients was a patient in the ICU who arrested post intubation, and this scenario is described below in the section on deaths. These incidents describe a range of different scenarios. Only one patient required intubation for an elective procedure in the operating theatre. The reporter mentioned the distraction of teaching as a contributing factor. The other incidents described urgent intubations in various settings, including the neonatal unit, ICU, ED and the operating theatre. A significant cognitive load in a stressful situation might have contributed to the human factors leading to delayed recognition of the misplaced intubation.
Deaths
Four deaths were recorded in this cohort, all involving severely unwell patients with complex medical issues. One was a multi-trauma patient with substantial injuries who required an ETT exchange during emergency surgery. This proved complicated and resulted in multiple rescue intubation attempts, of which one was an immediately recognised oesophageal intubation. The second incident described a patient who suffered an out-of-hospital cardiac arrest on the background of a significant complex medical history. One attempt at securing the airway during CPR resulted in an immediately recognised oesophageal intubation due to extensive gastric regurgitation in the ETT. The third patient in this cohort equally required intubation during CPR and had one immediately recognised oesophageal intubation identified by the excessive amount of gastric content in the ETT. Based on the information provided, the authors are unable to declare oesophageal intubation as the main contributor to the demise of these patients. All three of these suffered from significant comorbidities, required high doses of inotropic support and were acutely unwell.
The last incident in this cohort described the unrecognised oesophageal intubation in a severely ill patient in the ICU, which was recognised after the patient deteriorated into cardiac arrest. The operators initially assumed an equipment issue when non-sustained EtCO2 readings were observed and then changed to another ventilation device without EtCO2 monitoring. The patient rapidly deteriorated after the oesophageal intubation, suffered from a cardiac arrest requiring CPR and could not be revived. This patient was described as significantly unwell, and it is not inconceivable that an oesophageal intubation, which was unrecognised for some time, could trigger a cascade of deterioration in a patient of sufficient fragility.
Limitations
WebAIRS is a voluntary database, and there is no nationally mandated reporting of adverse anaesthetic events. Therefore, analyses of incidents rely on anaesthetists to report these. Incidents that are not perceived as significant may not be entered. Most oesophageal intubations are promptly recognised and corrected and are unlikely to be reported as adverse events. Therefore, many immediately recognised anaesthetic oesophageal intubations not causing patient harm may not be captured in webAIRS. The entry fields in webAIRS are not mandatory, and detailed information is not always provided. As the data and reporter details are de-identified it is impossible to collect additional information about the incident, patient or hospital details. Similar to other incident reporting systems, it is difficult to collect accurate denominator data, precluding absolute risk calculations or reliably determining causation.
Conclusions
The findings of this analysis show that oesophageal intubation continues to be an ongoing issue in anaesthesia. This is despite significant advances in patient safety initiatives, including advanced equipment and airway management guidelines and education. Patients continue to come to harm, requiring additional treatments and undergoing preventable, unnecessary invasive interventions, leading to ICU admissions or prolonged hospital stays. It was noticeable that several PUMA recommendations and airway management strategies, now considered a standard of care, were not fulfilled in several incidents. This may be due to the nature of voluntary incident reports in which not every detail of each event is provided, but it might also be an insight into current anaesthetic practice in Australia and New Zealand. At a bare minimum, EtCO2 readings must be available and used in every instance when airway management is performed. Multidisciplinary team education sessions across all specialities who perform airway management are required. The focus needs to be twofold: on technical aspects to avoid oesophageal intubation in general and on their immediate recognition, should they occur nevertheless. The second focus needs to be on non-technical aspects, including human factors and team recognition of human biases and their management. Clear diagnostic guidance and treatment strategies are required to be developed and tested. It is time to make oesophageal intubations in anaesthetic practice a relic of our history.
Footnotes
Author Contribution(s)
Acknowledgements
The author(s) would like to thank the large number of anaesthetists across Australia and New Zealand who are reporting incidents to webAIRS in the interests of patient safety. The authors would like to acknowledge the contribution of all members of ANZTADC, past and present, and the administrative assistance provided by ANZCA staff. Special thanks to A/Prof Ellen Louise Davies, Dr Simon Macklin, Dr Tim Basevi, Mr David Endlich and to the ANZTADC Publication Committee for their contributions to the editing and review of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the search, authorship and/or publication of this article.