
Abstract
The New Dunedin Hospital (NDH) is New Zealand’s largest health infrastructure build. Here we describe the use of a simple simulation-based hospital design exercise to inform the appropriate lift car size for critical care intrahospital transfers in the NDH. The intensive care unit (ICU) user group tested a series of entries and exits of simulated complex patient transfers in mocked-up lift cars of three different dimensions. Time taken to enter and exit the lift were recorded, reflecting the relative difficulty of transfer. Qualitative assessments were made of ease and perceived safety of transfer. These simulations demonstrated that recommended standard patient lift cars, often proposed for critical care transfers, could not physically accommodate all complex ICU transfers. A size of 1800 mm wide (W) × 3000 mm deep (D) had the physical capacity to permit all simulated ICU transfers, but with staff and patient risk. As lift car size increased to 2200 mm W × 3300 mm D, the simulation demonstrated reduced transfer times, smoother entry and exit, improved access to the head end of the bed, and reduced risk of disconnection or dislodgement of lines and airway support. The resultant clinical recommendations for the dimensions of a critical care lift car surpass current international health architecture guidelines and may help to inform future updates. The NDH project benefited from an objective assessment of risk, in language familiar to clinicians and healthcare architects. The outcome was an upsizing of the two ICU-capable lifts.
Keywords
Introduction
The New Dunedin Hospital
The New Dunedin Hospital (NDH) will be New Zealand’s largest single health infrastructure project to date. It is a two-stage hospital rebuild. The ambulatory building will include outpatients, day procedures, and planned radiology. The larger Inpatient Acute Services Building, with over 400 beds, will span 11 floors. Key acute services (emergency department, operating theatres, intensive care unit (ICU), maternity, and helipad) are stacked vertically in this main building.
Clinical engagement structure
A co-design approach with clinical users, non-clinical users, and consumers began in 2016 and continues today. Over fifty of these consultation groups met regularly with healthcare planners and architects. This consultation structure enabled the project to gather feedback and request expert opinion.
An overarching group of clinicians and consumers, the Clinical Leadership Group (CLG), provided clinical oversight across user groups. The CLG also acted as an advisory body for broader design questions from the project design team, the lift strategy being one example of this.
The draft New Dunedin Hospital lift strategy
In June 2020, the CLG welcomed the request to review the Draft Vertical Transport Strategy (‘lift strategy’). This presented preliminary modelling of lift numbers, lift car sizes and lift control systems for the larger inpatient building.
The strategy for the inpatient building was a bank of public lifts on the west of the building (the ‘public-facing’ side) and a separate bank of staff/patient lifts on the eastern side for staff and patient movements. Two of these were proposed to be oversized for critical care transports. Separate logistics lifts are also located on the eastern side.
The CLG provided feedback on several aspects of the lift strategy. This article relates to lift car sizes only.
In the absence of national New Zealand (or Australian) standards in this area, the draft lift car sizes presented to the CLG were based on the British Health Technical Memorandum 08-02 and Singapore 1.3 MEP (Table 1 and Figure 1).
Initial proposed lift car and shaft requirements for consultation, Draft New Dunedin Hospital Vertical Transport Strategy, June 2020.
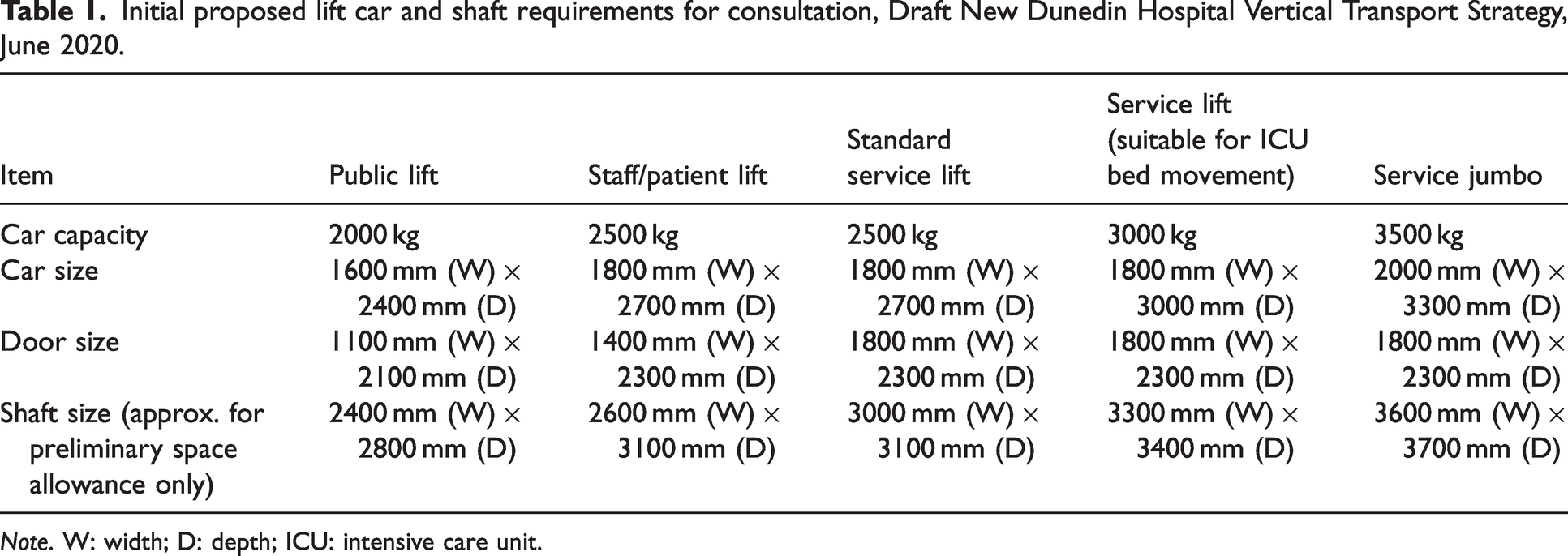
Note. W: width; D: depth; ICU: intensive care unit.
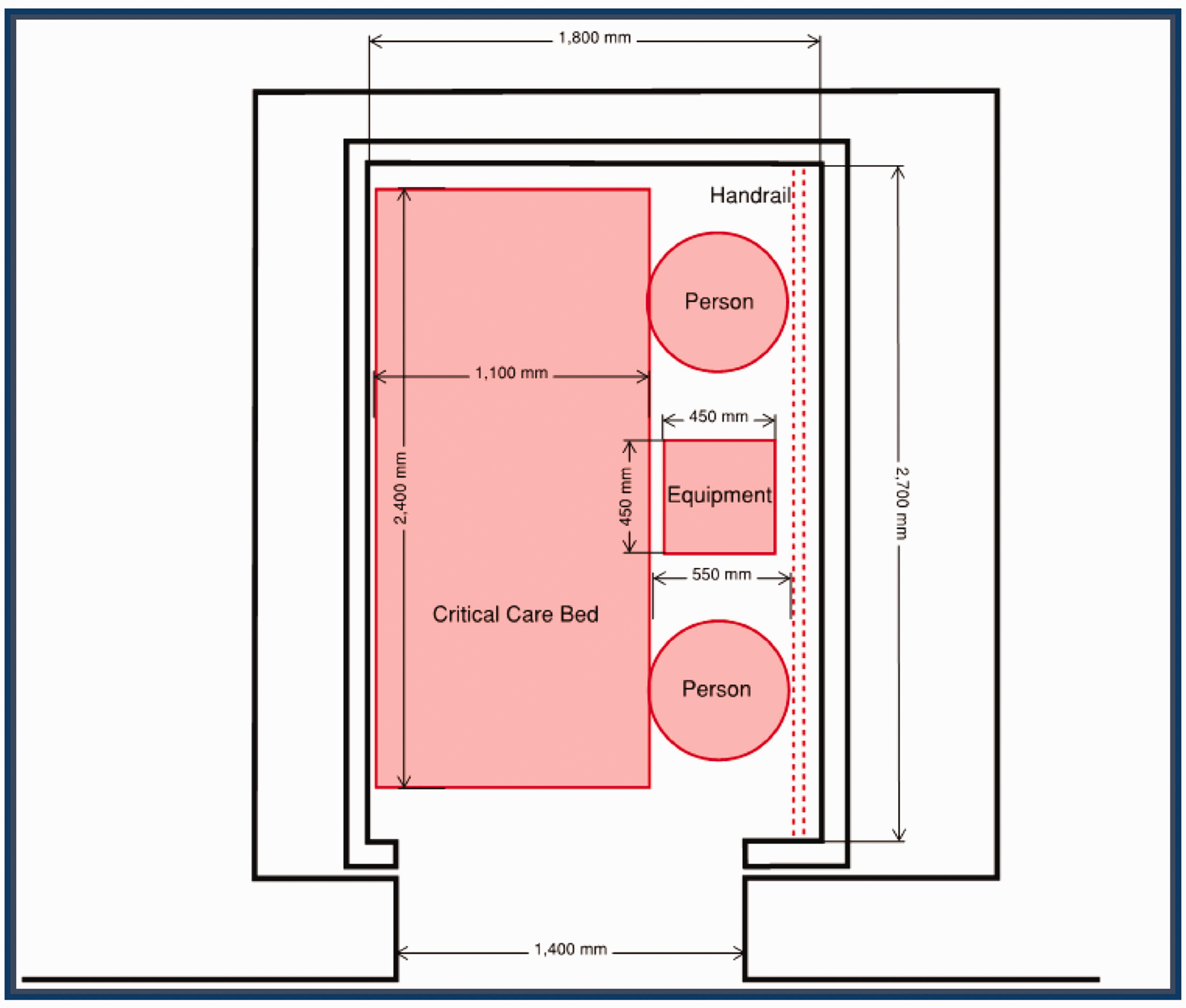
Sample lift car dimensions taken from New South Wales Engineering Services Guideline (2016) to demonstrate lift car dimensions and spatial allowances for equipment.
Clinical consultation on lift strategy
The CLG were concerned that lift car sizes for complex, ICU or bariatric transfers (‘Service lift jumbo service (suitable for ICU bed movement)’ in Table 1) were too small for safe clinical transfer.
Intensive care unit representatives on the CLG were well aware that intrahospital transfer is a known significant risk for ICU patients. Inadequate space, poor access to the patient and difficulty accessing elevators are contributory factors. 1 Longer durations of intrahospital transfer, and higher patient acuity are associated with increased transport-related complications. 2
Given that the CLG was challenging international healthcare design standards, there was a high burden of proof required. There was no published evidence on the direct impact of lift car sizes on ease or safety of transfer for these complex patients.
The CLG requested that the ICU user group use simulation to recommend the minimal and optimal critical care lift car dimensions to the NDH project team.
Methods and materials
Simulation set up
Simulations were carried out on a single day in the Dunedin Public Hospital ICU Phase 2 area. This was a refurbished patient care area not yet open to patients. A Laerdal Annie QCPR manikin and staff actors were used to simulate patients.
Standard ICU beds (Hill Rom® Care Assist® ES 1020 mm × 2286 mm) were used for all scenarios except Scenario 4 (Arjo Citadel Plus bariatric bed, 1180 mm × 2400 mm, or 1340 mm × 2500 mm extended). All beds were manually pushed, without power assist. The Hamilton T1 transport ventilator was used for all ventilated scenarios except Scenario 7 (Hamilton C6 ventilator). Real ICU equipment was used, relevant to each scenario.
An ICU standard room, with sliding doors, was selected as the lift ‘car’. Elevator sizes were taped on the floor of this ICU room:
Proposed staff/patient lift 1800 mm wide (W) ×2700 mm deep (D), with a door opening of 1400 mm. Proposed ICU/service lift 1800 mm W × 3000 mm D (the largest proposed for patient movement), with a door opening of 1800 mm. ICU jumbo lift 2200 mm W × 3300 mm D with a door opening of 1800 mm.
The first two lift car sizes were those proposed in the draft strategy. The third, the largest lift simulated, was proposed by the ICU user group, and was based on recent Australasian hospital builds they were familiar with.
Door opening sizes (in mm) were marked where smaller than the car width:
Staff/patient lift 1400 mm Service/ICU lift and jumbo lift 1800 mm.
Trolleys and shelving units were used to simulate elevator walls (Figures 2 and 3).

ICU standard room, with sliding doors, selected as the lift ‘car’. Lift car sizes and door openings taped on the floor. Mobile trolleys used as lift ‘walls’.
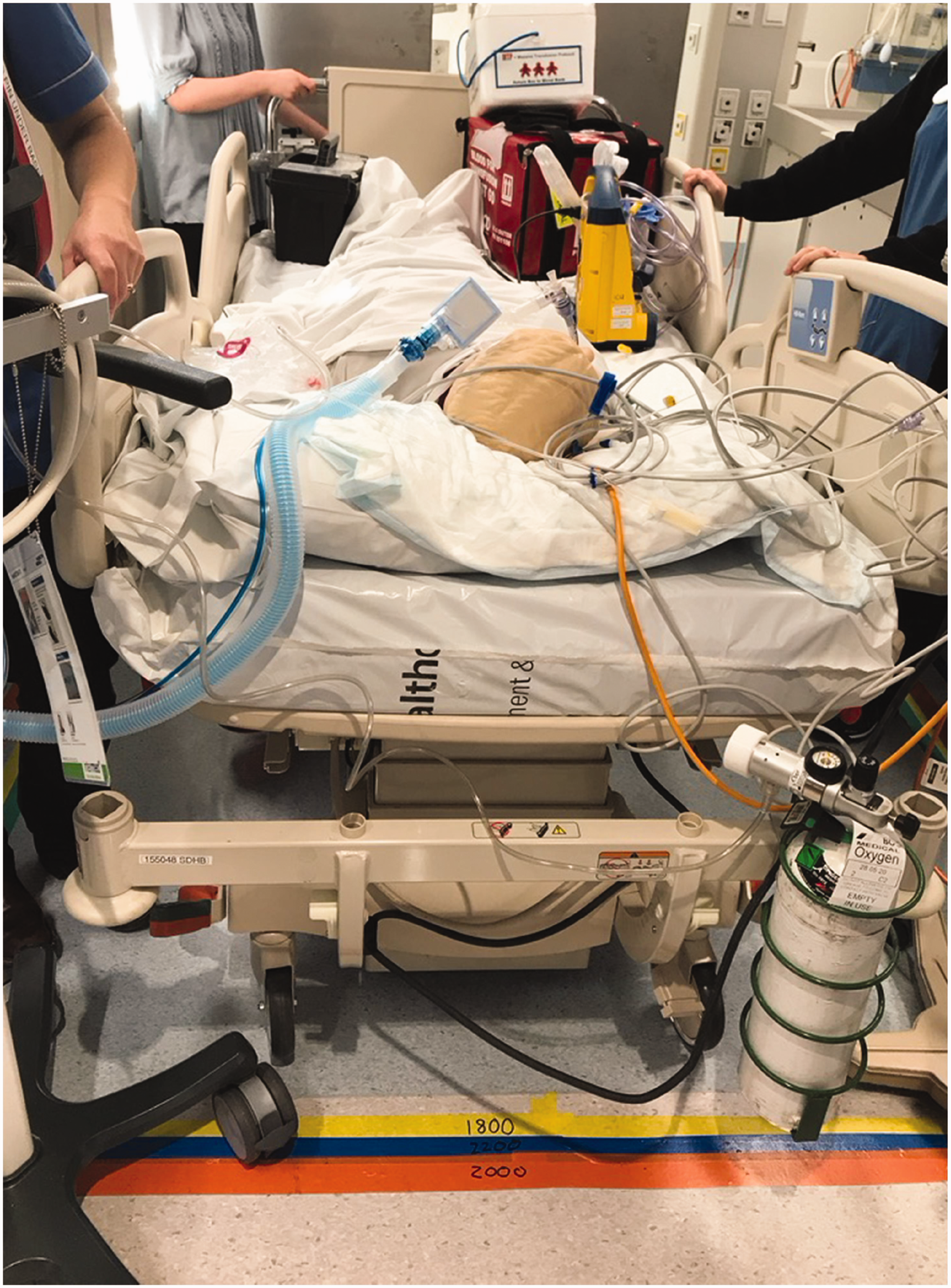
Sample scenario (ICU trauma patient with traction bed) showing use of real staff and equipment.
To provide a standardised start point, all scenarios began with the foot of the bed 2000 mm from the central opening point of the ‘lift’ doors, along a corridor. The team pushed the bed towards the lift and negotiated a 90° turn (in the 2300 mm wide corridor) into the lift. Once all equipment and staff were inside the lift and the door fully closed, the entry scenario ended. Exit scenarios were measured from the moment of full opening of lift doors to when the head of the bed crossed the original starting point.
Simulation team
The simulation participants consisted of an ICU senior medical officer (SMO), two ICU senior nurses, an anaesthetic SMO, an ICU registrar, an orderly, a medical student and, for Scenarios 5 and 8, an obstetric SMO. Each participated in every simulation where their simulated role would normally be present.
The observers were a further ICU SMO (timekeeper/observer), an ICU nurse educator, an ICU associate charge nurse manager, the charge midwife manager, and a clinical project manager from the NDH project team.
Other than the orderly and the medical student, all participants and observers had extensive experience in ‘standard’ simulation: testing clinical systems and human performance but not in simulation for healthcare design.
Prebrief
The objectives and design of the simulation were explained to the participants by the lead observer (an ICU SMO). They were encouraged to standardise their behaviours within each scenario where possible. They were familiarised with the simulation set up and given time to consider how they would approach moving the patient. Participants were reassured that this simulation was focusing on the built environment and not on their individual or team performance.
Scenarios tested
Nine scenarios were simulated (Table 2). Each scenario was performed once for each of the three different lift sizes, preceded by a ‘practice run’ for each scenario to orientate any new members of the team. There was no specified order in which the different sizes for each scenario were tested.
Simulation scenarios, staff and equipment.
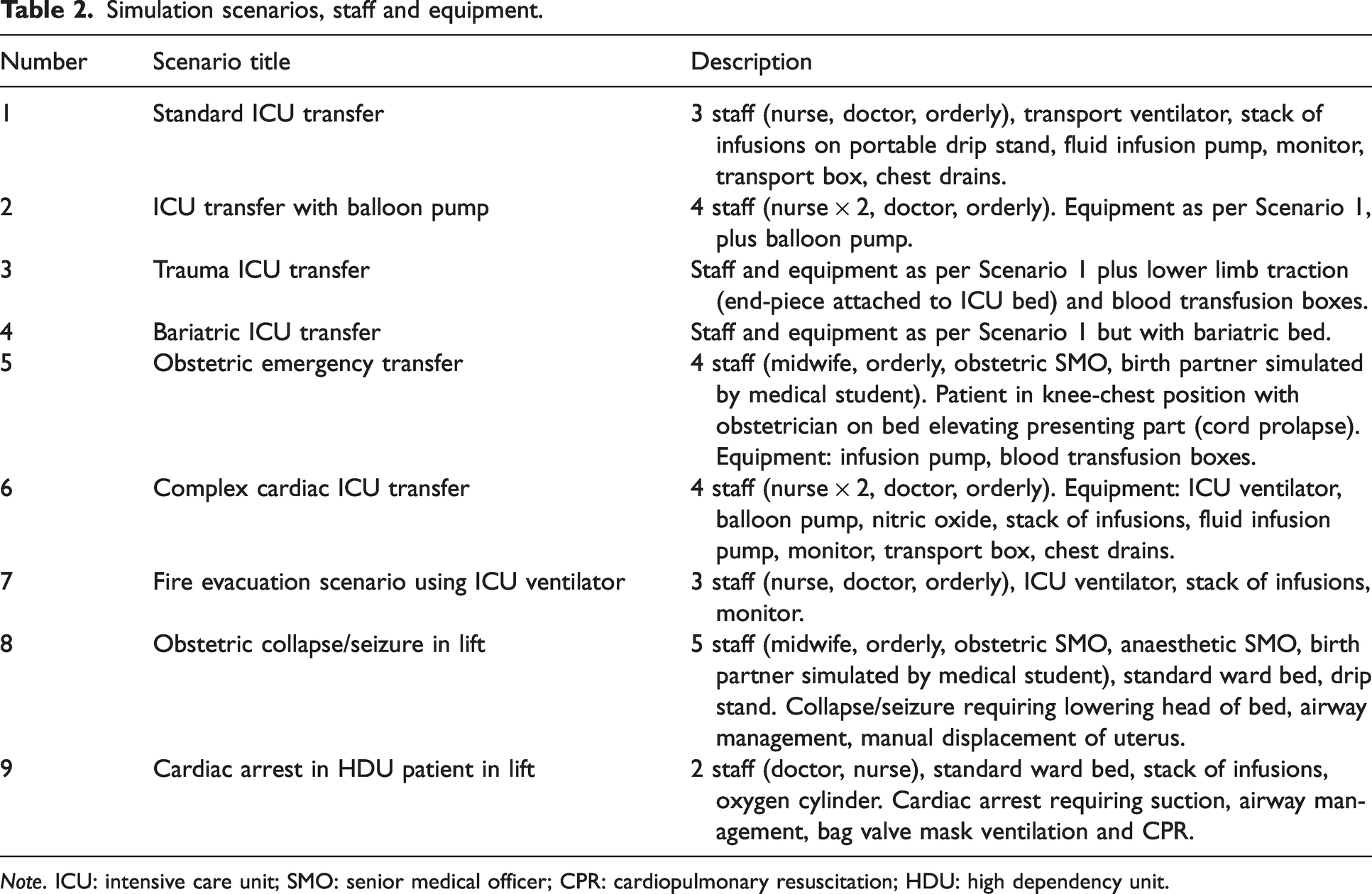
Note. ICU: intensive care unit; SMO: senior medical officer; CPR: cardiopulmonary resuscitation; HDU: high dependency unit.
Quantitative outcomes
For the transfer scenarios (1 to 7) time taken to enter and exit the lift were also recorded. This was felt to reflect the relative difficulty of each transfer. Time started when the team started pushing the bed from the standardised starting position. Time stopped when the full scenario team and equipment were inside the simulated lift car, and the doors closed. For exit scenarios, time started when the lift doors were fully open, and stopped when the head of the bed crossed the original starting point.
In addition, for Scenarios 8 and 9 (simulated emergencies within the lift), time to effective clinical intervention was measured. Time began at the point where the lift doors were closed and an observer then declared the clinical emergency. For Scenario 8 (obstetric collapse/seizure), effective intervention was defined as the time to lower the head of the bed, initiate basic airway management and manual displacement of the uterus. For Scenario 9 (high dependency unit (HDU) patient with cardiac arrest) this was defined as the time to achieve effective bag mask ventilation and initiate cardiopulmonary resuscitation.
Qualitative outcomes and debrief
For all scenarios (1 to 9), qualitative assessments were made of ease and safety of transfer. After each scenario there was a 5-min informal debrief with the participants by the lead observer, an ICU clinician experienced in hospital systems simulation. Once all scenarios were completed, there was a combined team debrief with all members of the team, again led by the lead observer. Open questions were used such as ‘How did that go?’, or ‘Did you encounter any difficulties?’, guiding participants and observers to comment on the following predetermined themes:
Whether the transfer scenario could be accommodated within the marked lift size. Whether significant rearrangement of equipment or personnel was required to do this. Any actual or potential clinical incidents. Ease of access to patient’s head for airway management. Other lessons learned.
Results
Transfer Scenarios 1 to 7: Entry and exit times
Entry and exit times for each scenario and lift size are presented in Table 3. Several of the scenarios were not possible in standard patient lifts. Entry and exit times were consistently shorter using the largest size of lift.
Entry and exit times for transfer scenarios.
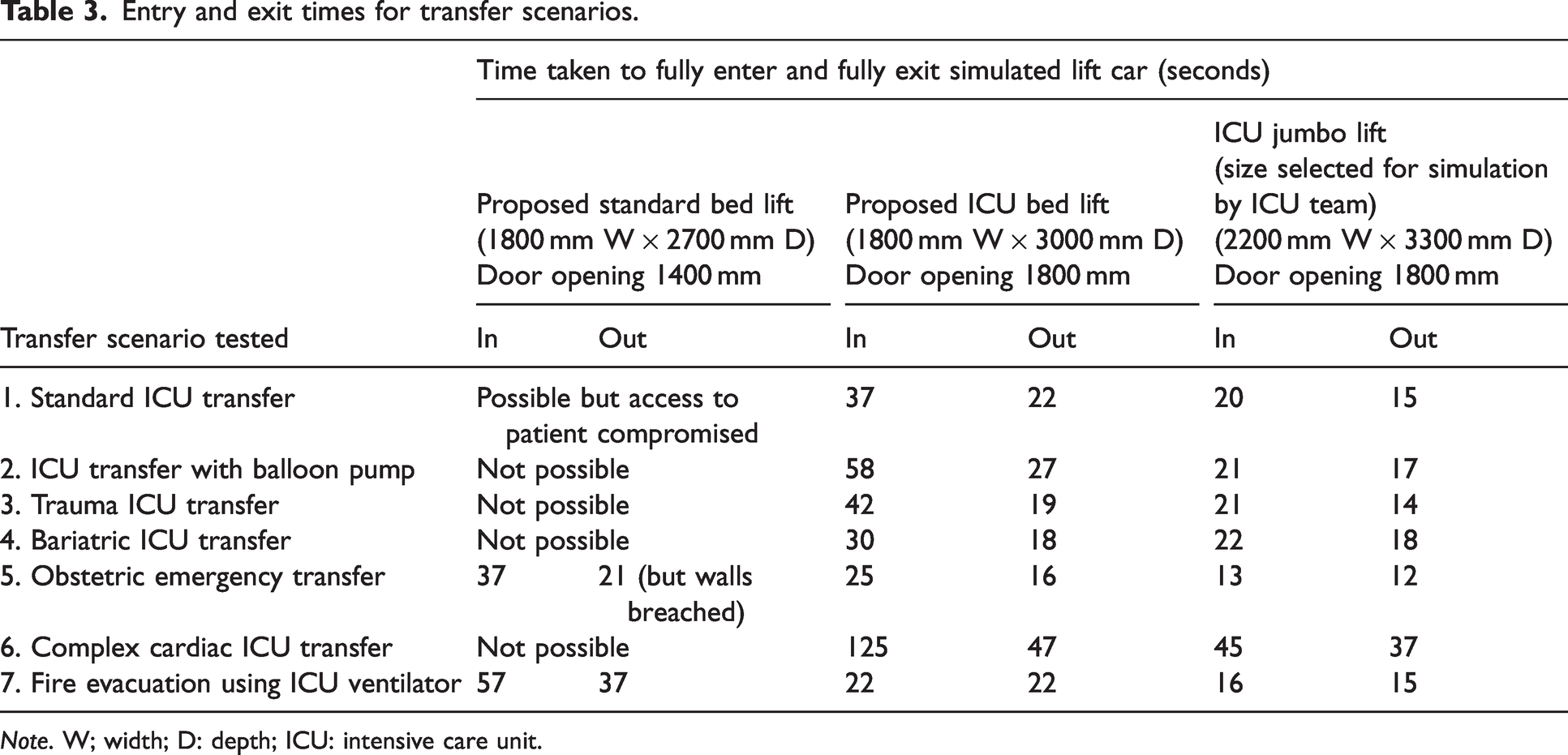
Note. W; width; D: depth; ICU: intensive care unit.
Transfer Scenarios 1 to 7: Qualitative findings – ease and safety, critical incidents, other lessons learned
1) Standard ICU patient transfer
It was possible to transfer an ICU patient in a standard staff/patient lift with difficulty, however, the head of the patient could not be accessed. With the ICU/service lift, it took time and manoeuvring of the bed and infusion pumps to get the ventilator into the lift, with risk of disconnection.
With the ICU jumbo lift, the patient and equipment were wheeled straight in.
2) ICU transfer with balloon pump
It was not possible to manoeuvre the bed, staff and equipment for this transfer into a standard staff/patient lift. Using the ICU/service lift required moving the balloon pump to get the ventilator and infusion pumps into the space, risking dislodgement or disconnection of lines and airway support.
With the ICU jumbo lift, the patient and equipment were pushed straight in.
3) Trauma ICU transfer
The ICU traction frame was too high (around 2100 mm) to fit into ICU side rooms so was not tested in the simulated lift. Proposed NDH lift car heights would accommodate this. A traction bed was, instead, simulated with the extended end-piece attached to an ICU bed.
It was not possible to get the extended bed, transport ventilator and infusions into the standard service lift. It was possible to get into an ICU/service lift, with some difficulty. The ICU jumbo lift allowed direct entry and exit, and access to the patient’s airway.
4) Bariatric ICU transfer
This bariatric bed (non-extended) was slightly wider than a standard ICU bed, but was heavier, more difficult to push and had motors attached to the end (these motors were not used in this scenario). Transfer times and ease of movement were similar to Scenarios 2 and 3, noting that the bed was used in its non-extended form.
Transfer was not possible in the standard patient/staff lift, difficult in the ICU/service lift, and straightforward in the ICU jumbo lift.
5) Obstetric transfer
Emergency obstetric transfers may require manoeuvres such as bimanual compression or elevation of the presenting part (simulated here). A staff member may need to get on to the patient’s bed to facilitate treatment. In the standard patient/staff lift this scenario was difficult, requiring repositioning of the drip stand to close the door, causing delay. The doors (1400 mm door opening) were an additional obstacle, with the bed and drip stand hitting the door on the way out.
The ICU/service lift was adequate but the ICU jumbo lift enabled a quick and smooth transfer. Routine transfers from the labour ward or theatres to the postnatal ward should allow a birth partner, infant in cot, midwife and orderly to travel in the same lift.
6) Complex cardiac transfer
This was not possible in the standard patient/staff lift. The ICU/service lift was not suitable for this type of patient transfer: entering the lift required over 2 min of juggling equipment. Lines and tubing were pulled, and under tension. The simulated lift walls were breached twice. Equipment was scraped along the walls both on entry and exit.
This transfer was easier and safer in the ICU jumbo lift, although there was still some manoeuvring required.
7) Fire evacuation
In this scenario, multiple ICU patients may need to be evacuated, using standard ICU ventilators (rather than smaller transport ventilators) and staff/patient lifts. This was barely possible in the standard staff/patient lift. The simulated walls were transiently breached, and there was insufficient access to the patient. The narrow door opening (1400 mm) was an additional obstacle. The ventilator was accidentally disconnected and lines were pulled.
This transfer was easier in the ICU/service lift. The ICU jumbo lift transfer was considerably quicker and easier, with the patient and equipment wheeled straight in.
Emergency scenarios (8 and 9): Time to achieve effective intervention (Table 4)
Emergency scenarios (8 and 9): Qualitative findings – ease and safety, critical incidents, other lessons learned
8) Obstetric collapse/seizure in lift
In the standard lift, it was not possible to get to the head of the bed to manage the patient’s airway. This was possible in the proposed ICU lift, but required either removing the drip stand on the corner of the bed, or a staff member climbing over the corner of the bed.
Time to achieve effective intervention for emergency scenarios in lift (see Methods for definition of effective intervention).
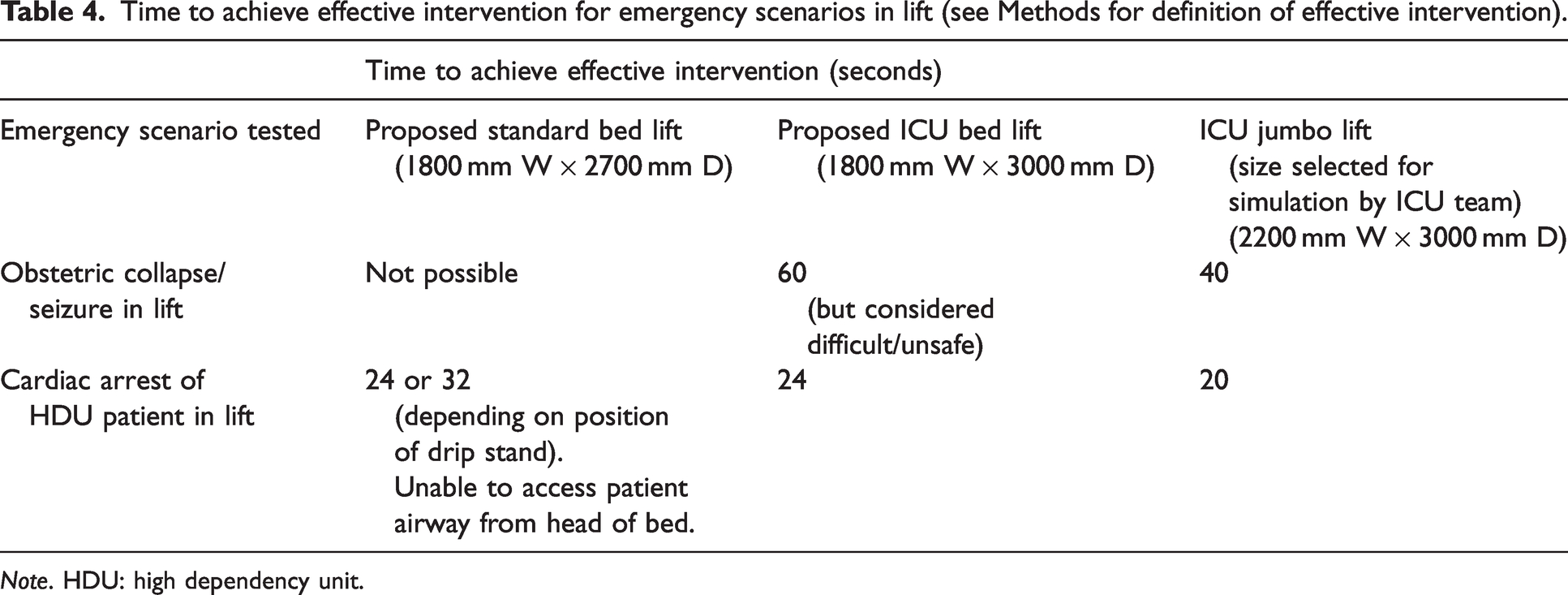
Note. HDU: high dependency unit.
In the jumbo lift, access was straightforward.
9) Cardiac arrest of HDU patient in lift
Access to the patient’s airway from the head end of the bed could not be achieved in the standard bed lift, even with the removal or rearrangement of equipment.
In the proposed ICU lift, it was possible to access the patient’s airway and perform chest compressions in a similar time frame to the jumbo lift.
Discussion
Key findings
Internationally recommended standard patient lift car sizes of 1800 mm W × 2700 mm D with a door opening of 1400 mm, also routinely proposed for critical care transfers, could not accommodate several simulated complex ICU transfers. These included complex cardiac, bariatric, and trauma ICU patients. The lift car size of 1800 mm W × 3000 mm D with a door opening of 1800 mm (originally proposed for ICU patient bed movement in the NDH) enabled all simulated ICU transfer scenarios to take place. However, this was associated with more clinical risk and longer transfer times than the largest sized lift. Using a larger simulated lift size of 2200 mm W × 3300 mm D with a door opening of 1800 mm (‘ICU jumbo’ in this exercise) accommodated all transfer scenarios. In addition, across all scenarios, it allowed for reduced transfer times, smoother entry and exit, improved access to the head end of the bed, and reduced simulated clinical risk of disconnection or dislodgement of lines and airway support. This was also the only size simulated that safely accommodated effective management of an obstetric collapse.
Limitations
Limitations relate to the intentional simplicity and rapid setup of this simulation: it was designed to answer a design question in a pragmatic way. The setup, participants and observers all utilised existing resources. This meant that repeat scenarios were not possible and there was no dedicated mock-up. Whilst the majority of the team were experienced in simulation for healthcare systems, no one had applied this to hospital design before.
Intrahospital transport is a known hazard
Moving critical care patients in lifts is a frequent part of many intrahospital transports (IHTs). Intrahospital transports are associated with a wide range of complications, many of which occur frequently and have negative effects on patient stability and outcomes. 2 A recent metanalysis of over 12,000 critical care intrahospital transfers found a pooled frequency of all adverse events of 26.2%. The incidence of life-threatening critical events or death was low, at 1.47% and 0% respectively. 3
There is no direct research on how the provision of clinical care in lifts or elevators contributes to complications during IHT. However, there are findings from existing literature that can be extrapolated in support of optimising the ease and reducing the duration of lift transfers, particularly for the critical care cohort.
Complications during IHT can be classified into four broad categories: adverse medical or clinical changes, mechanical problems, environment-related difficulties, and patient and staff management issues. 2
As with the simulated ICU patients here, higher patient acuity is associated with more frequent and serious IHT-related outcomes. 2 The Australian Incident Monitoring Study reported serious adverse outcomes in 31% of IHT incidents in ICU patients, concluding that intrahospital transport was an important risk to ICU patients. 1 Specific risk factors associated with adverse events during IHT include emergent/urgent indications for the trip, the presence of mechanical ventilation, transport for diagnostic procedures, number of infusion pumps, duration of the overall process, and sedation requirement.4 –6 Unanticipated loss of airway can be catastrophic in the setting of respiratory failure. 7
Not unexpectedly, these simulations showed that as lift car size increased there was a reduction in time taken to fully enter and exit the simulated lift car. This time saving may be clinically important – a number of studies have reported that duration of IHT is a significant factor in increasing complications during and/or after transport. 2 In one study of 125 ICU transports, patients without waits at the destination had a 28% lower incidence of adverse events. 8
Relevant to providing ICU-level care in a restricted space, limited space and inadequately sized rooms have been reported as an environmental reason for transport delays that worsen complications. 1 Inadequate space has been linked, for example, to difficulty in accessing patients, the inability to see monitors, and staff inability to leave a room when necessary due to tight spaces and congestion. 9
Difficulty in accessing elevators was reported as one reason for transport-related complications in the Australian Incident Monitoring Study. 1
Challenging healthcare architecture/design standards
Hospital design is guideline- and standard-based. In the NDH project, as with many others, if there is a clinical recommendation to ‘exceed’ a guideline, this must be benchmarked against similar facilities, and demonstrate meaningful clinical risk reduction.
In Australasia the base guidelines for healthcare design are the Australasian Health Facility Guidelines. These do not include guidance on lifts, and New Zealand has no guidelines for provision of lifts in hospitals. Therefore guidance must be sought internationally.
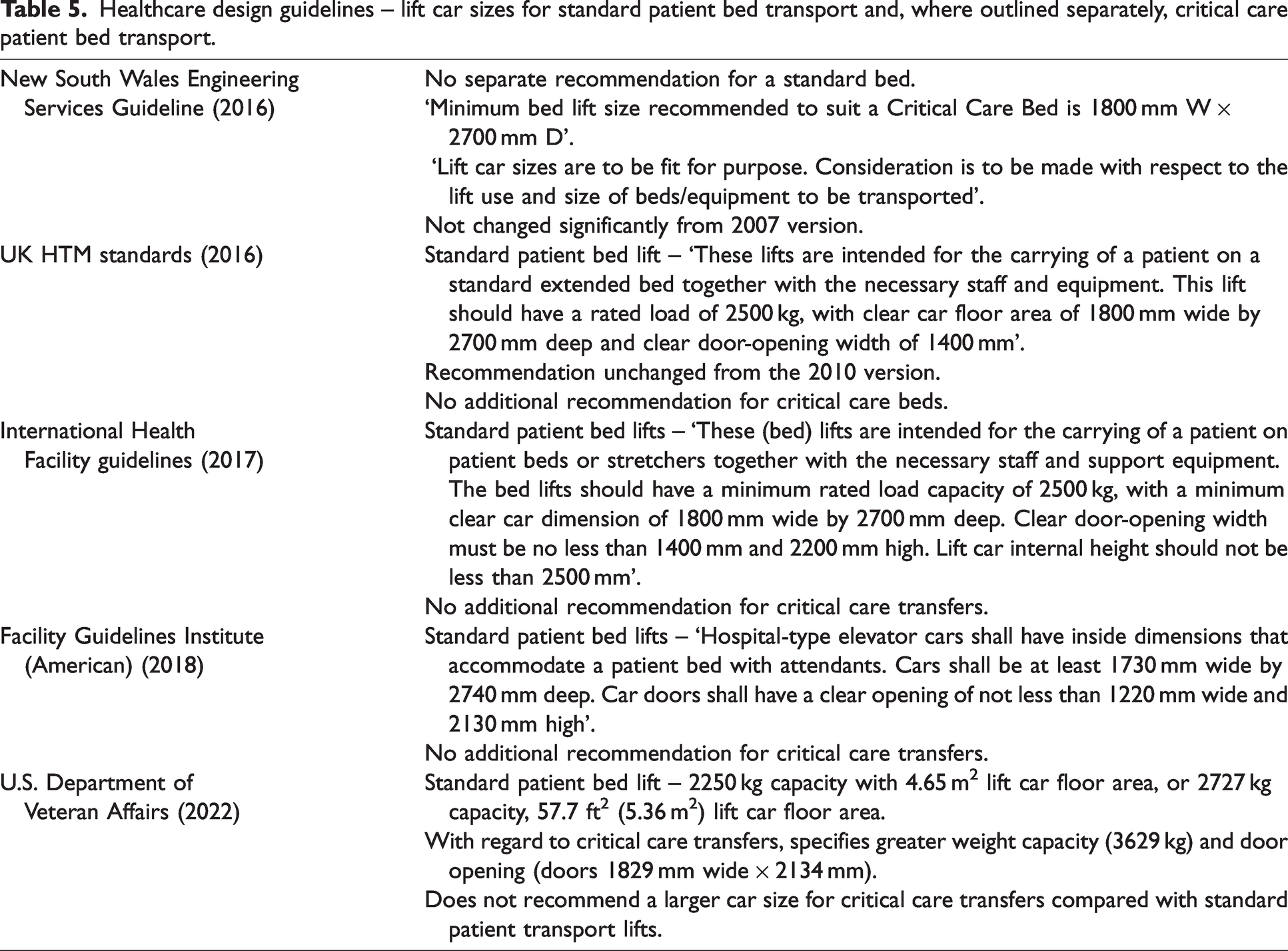
Interestingly, no international healthcare design guideline (Table 5) gives a strong or clear recommendation that a critical care lift must be any larger than a standard bed lift (sized 1800 mm W × 2700 mm D). These recommendations have not changed in over ten years.
Healthcare design guidelines – lift car sizes for standard patient bed transport and, where outlined separately, critical care patient bed transport.
The implications for increasing lift size are potential capital and operational costs. The NDH quantity surveyors estimated that, at the time of discussions with potential suppliers, the average cost premium for a jumbo lift (2000 mm × 3300 mm, weight 3500 kg) versus a standard patient/staff lift (1800 mm × 2700 mm, weight 2500 kg) was approximately NZ$300,000 each, excluding goods and services tax (GST). This does not account for the increase in floor area (approximately NZ$7000/m2 excluding GST). In terms of operational costs, the NDH electrical engineers estimated an energy premium upwards of 15% when using the jumbo lift compared with the standard sized lift. Maintenance costs were unlikely to differ significantly between the two sizes.
Design endorsement for the New Dunedin Hospital
The findings from the ICU simulation were endorsed by the CLG for the NDH and raised as a clinical risk with the NDH programme director. The CLG recommended two ICU-capable jumbo lifts.
Following further conversations with the project team, and in line with the jumbo lift installed at the recently built Waipapa Christchurch Hospital Acute Services building, a final size of 2000 mm W × 3300 mm D (door opening 1800 mm) was progressed for two ICU-capable jumbo lifts.
Conclusions
These simulations demonstrated that the internationally recommended standard patient lift car size of 1800 mm W × 2700 mm D with a door opening of 1400 mm, often proposed for critical care transfers, could not accommodate all complex ICU transfers. A size of 1800 mm W × 3000 mm D with a door opening of 1800 mm physically permitted all simulated ICU transfers but with residual staff and patient risk. As lift car size increased further to 2200 mm W × 3300 mm D the simulation demonstrated reduced transfer times, smoother entry and exit, improved access to the head end of the bed, and reduced simulated risk of disconnection or dislodgement of lines and airway support.
These outcomes may seem like common sense to clinicians familiar with intrahospital transport. However, without evidence linking lift car size to safety and feasibility of clinical transfer, healthcare design will continue to rely on existing (and often historical) standards.
Relating to the NDH project, particularly relevant with its vertically stacked structure of high acuity units, our CLG found this simulation to be a powerful contribution to the co-design process. Rather than relying on clinical anecdote or opinion, the use of this relatively simple simulation exercise provided an objective and fair assessment of risk, in language familiar to project management.
Findings were included in the NDH project’s final NDH Vertical Transport Design Report and led to an upsize of the NDH lift car sizes for complex, ICU and bariatric transfers.
Footnotes
Author Contribution(s)
Declaration of conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.