
Abstract
Regional anaesthesia is an essential tool in the armamentarium for paediatric anaesthesia. While largely safe and effective, a range of serious yet preventable adverse events can occur. Incidence and risk factors have been described, but few detailed case series exist relating to paediatric regional anaesthesia. Across Australia and New Zealand, a web-based anaesthesia incident reporting system enables voluntary reporting of detailed anaesthesia-related events in adults and children. From this database, all reports involving paediatric regional anaesthesia (age less than 17 years) were retrieved. Perioperative events and their outcomes were reviewed and analysed. When offered, the reported contributing or alleviating factors relating to the case and its management were noted. This paper provides a summary of these reports alongside an evidence review to support safe practice. Of 8000 reported incidents, 26 related to paediatric regional anaesthesia were identified. There were no deaths or reports of permanent harm. Nine reports of local anaesthetic systemic toxicity were included, seven equipment and technical issues, six errors in which regional anaesthesia made an indirect contribution and four logistical and communication issues. Most incidents involved single-shot techniques or a neuraxial approach. Common themes included variable local anaesthetic dosing, cognitive overload, inadequate preparation and communication breakdown. Neonates, infants and medically complex children were disproportionately represented, highlighting their inherent risk profile. A range of preventable incidents are reported relating to patient, systems and human factors, demonstrating several areas for improvement. Risk stratification, application of existing dosing and administration guidelines, and effective teamwork and communication are encouraged to ensure safe regional anaesthesia in the paediatric population.
Keywords
Introduction
Regional anaesthesia offers many advantages to the paediatric population, providing excellent analgesia, reducing opioid consumption and related adverse effects. In the neonatal population, avoiding general anaesthesia may reduce the incidence of apnoea, respiratory compromise and potential effects on developing neurons. 1 , 2 With a range of developmental stages, having effective and consistent peripheral modes of analgesia can ensure comfort is achieved regardless of communicability. Intentional motor blockade and vasodilation with local anaesthesia can optimise surgical conditions intraoperatively, and reduced mobility may be preferred postoperatively if intricate procedures are performed in patients with limited compliance. Several databases prospectively collect outcome data relating to paediatric regional techniques, 3 , 4 and from these reports of permanent harm are exceedingly rare. There is a relatively low incidence of transient sequelae (2.4 per 10,000) from regional anaesthesia. 3 Regardless, avoidable adverse events occur and can complicate the perioperative course. Reports of minor and severe adverse events related to paediatric regional anaesthesia feature in the web-based anaesthesia incident reporting system (webAIRS) database and draw together some common themes, providing valuable learning. This paper aims to review and analyse these incidents, discussing specific contributing factors. Suggestions for practice change based on available evidence and consensus guidelines will be provided.
Methods
WebAIRS is a voluntary de-identified anaesthesia incident reporting system established in Australia and New Zealand in September 2009. 5 Registered anaesthetists and departments may add reports about anaesthetic incidents anonymously. An overview of the first and second 4000 incidents was published in 2017 and 2021, respectively, and de-identified data collection methods were described in detail. 5 , 6 Data are collected in compliance with the National Health and Medical Research Council 2014 recommendations for de-identified quality assurance data. In addition, multi-centre ethics approval is maintained by the Royal Brisbane and Women’s Hospital Human Research Ethics Committee (HREC/11/QRBW/311) and the Nepean Blue Mountains Local Health District (HREC/12/NEPEAN/18). In New Zealand, ethics approval has been obtained from the Health and Disability Ethics Committee (MEC/09/17/EXP). In addition, reporters at each site must comply with local institutional approval requirements. The reports are confidential and protected by qualified privilege in both Australia and New Zealand. 6
Incidents affecting paediatric patients less than 17 years of age were extracted from the first 8000 reports to webAIRS. Additionally, incidents which did not directly categorise by patient age were scanned and added to the analysis if the written narrative described an age which fitted the inclusion criteria of less than 17 years. Following this, incidents that reporters coded to have regional anaesthesia as part of their management were extracted, and their narratives reviewed. A targeted word search in all narrative sections to identify incidents that resulted in local anaesthetic systemic toxicity (LAST) was separately performed and added to the analysis. Search words included: ‘toxicity’, ‘seizure’, ‘LAST’, ‘systemic’, ‘Intralipid’®. Only incidents caused directly or indirectly by regional anaesthesia were included in this report (Figure 1).
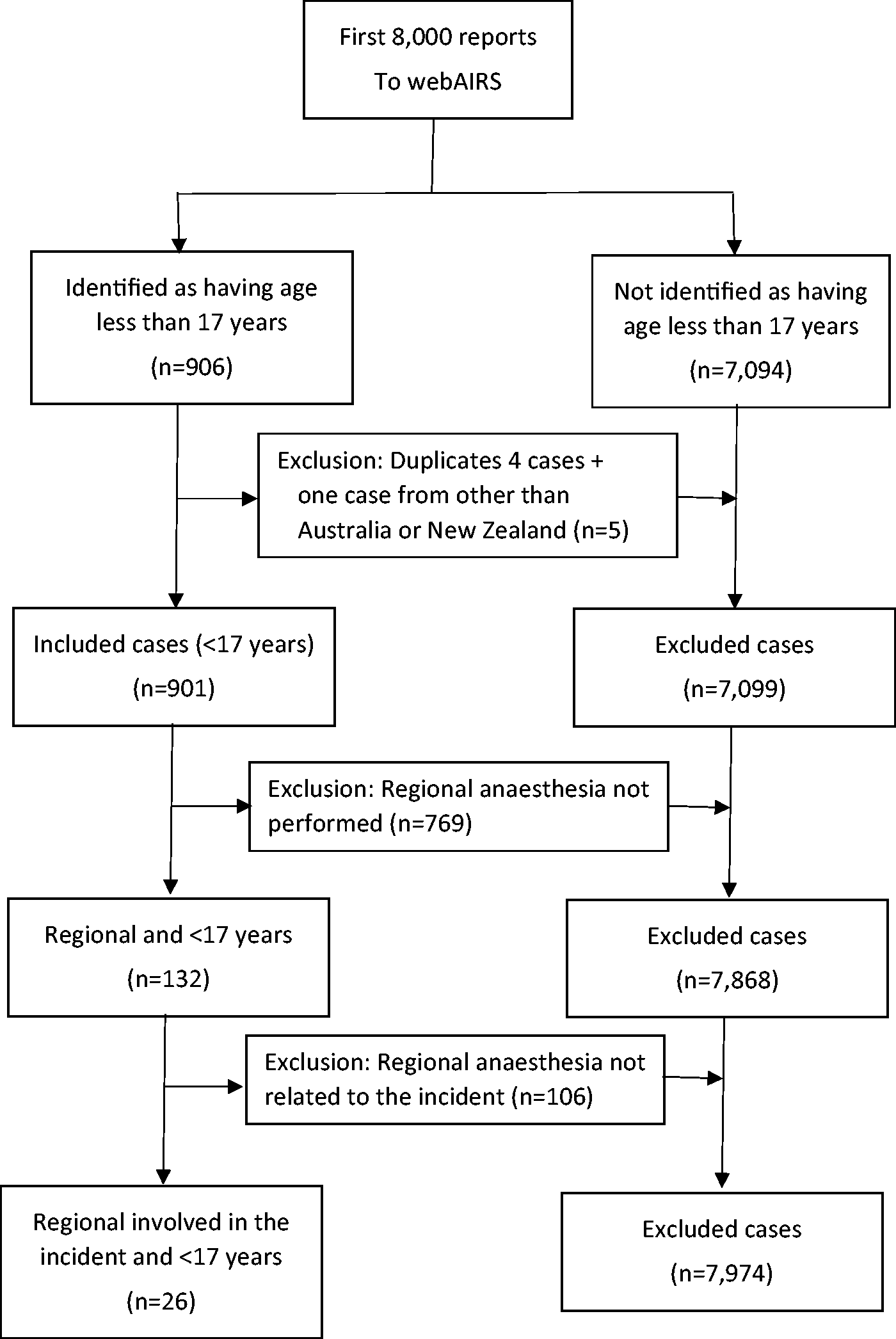
Inclusion flowchart for incidents related to regional anaesthesia.
Results
Of the 8000 incidents reported to webAIRS, 899 involved patients less than 17 years old. The reporters did not state the age in 207 reports, but it was possible to determine the age was less than 17 years in seven additional reports from the narrative sections giving an initial total of 906 reports. After excluding four duplicates and one incident reported from outside Australia or New Zealand, 901 paediatric incidents remained.
From these 901 reports, incidents coded by the reporter to have included regional anaesthesia were extracted. Additionally, a narrative review across the remaining paediatric incidents was performed and one report was added to the review resulting in 132 reports. These reports were reviewed and all incidents unrelated to regional anaesthesia were excluded (n = 106).
Incidents were categorised into common themes. Eight incidents involved technical (Table 1) and equipment issues (Table 2), nine incidents resulted in LAST (Table 3), four incidents involved planning, logistics and communication (Table 4), and five incidents led to medication-related errors (Table 5). All incident data were reviewed in detail by the authors; the description and analysis are included in the following discussion.
Technical issues.
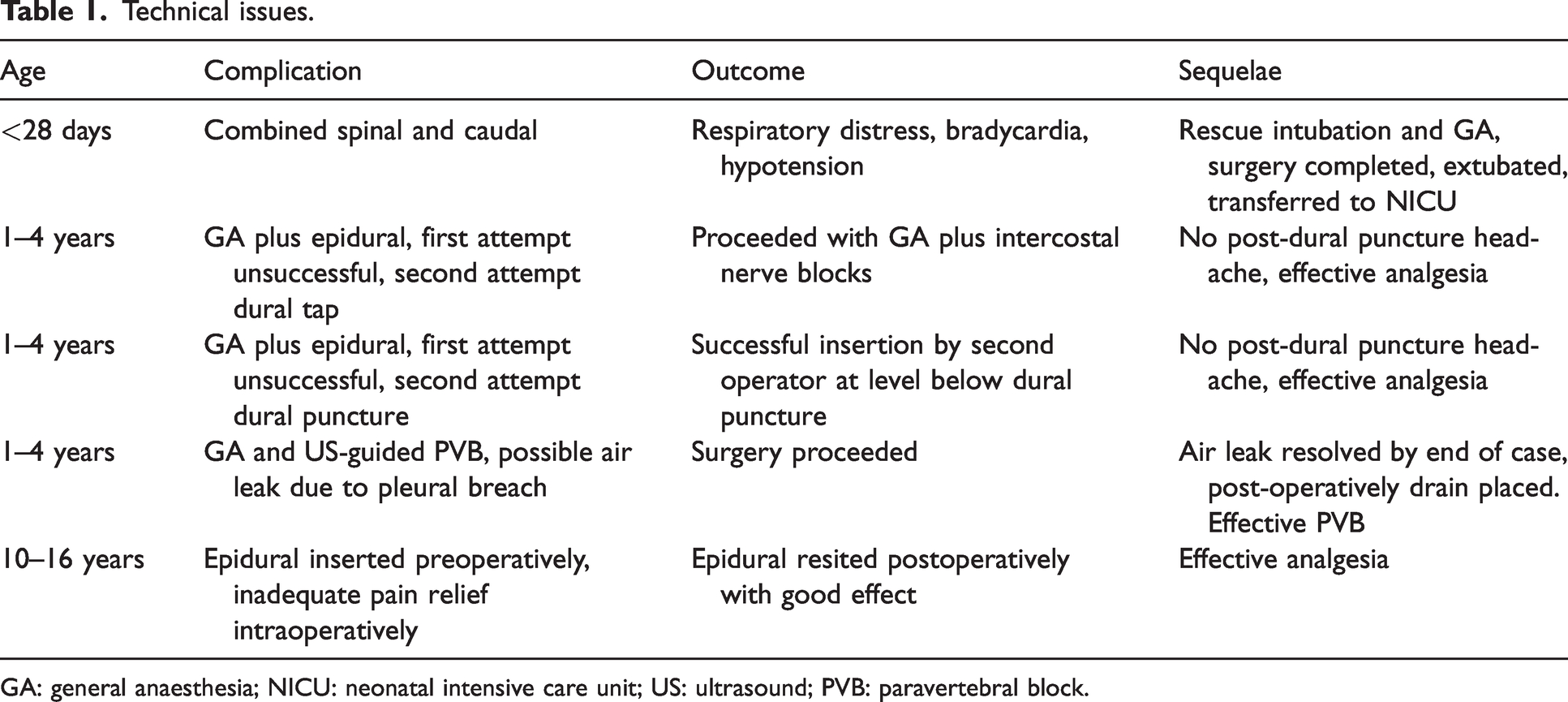
GA: general anaesthesia; NICU: neonatal intensive care unit; US: ultrasound; PVB: paravertebral block.
Equipment issues.
GA: general anaesthesia.
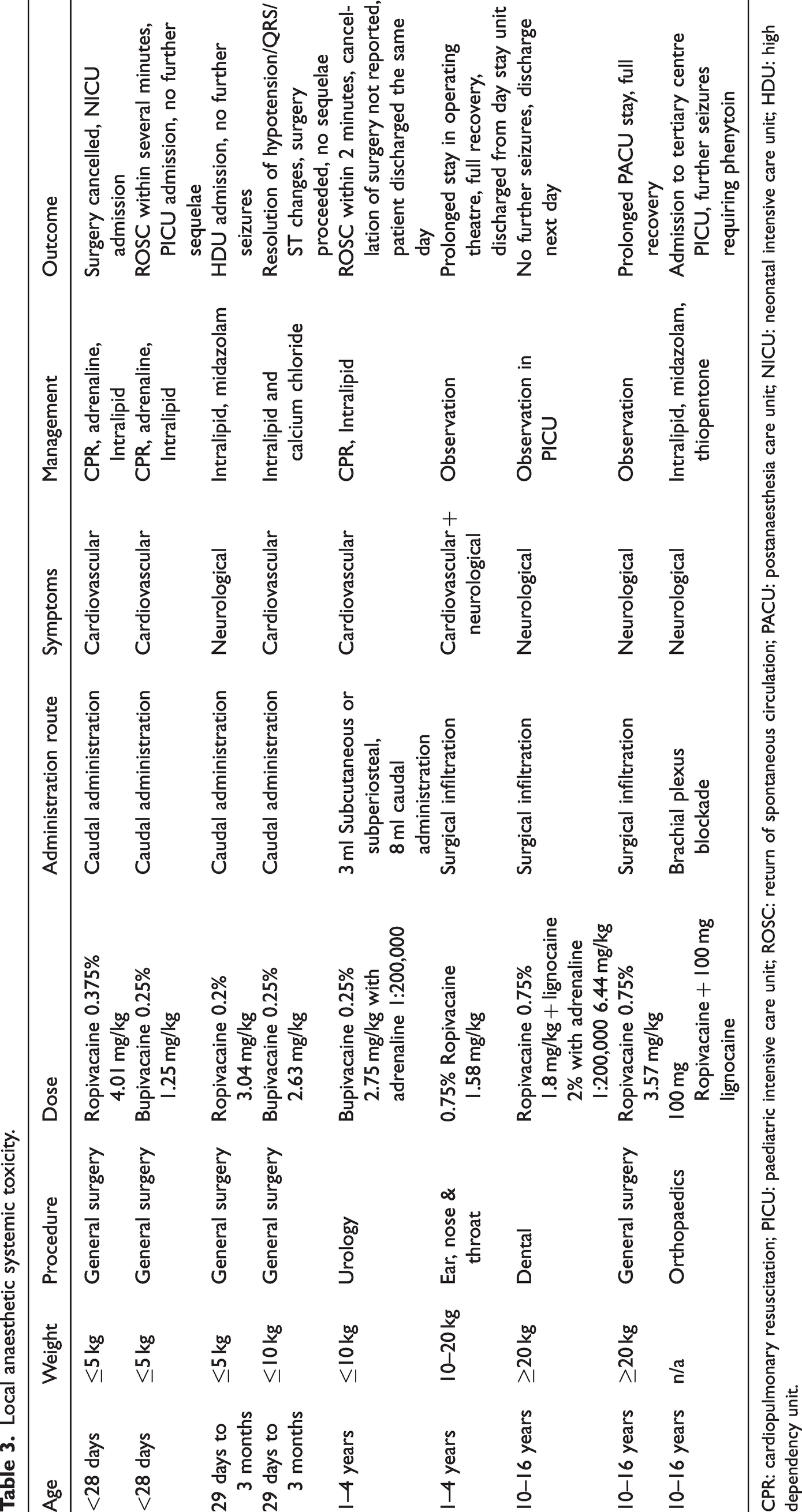
Local anaesthetic systemic toxicity.
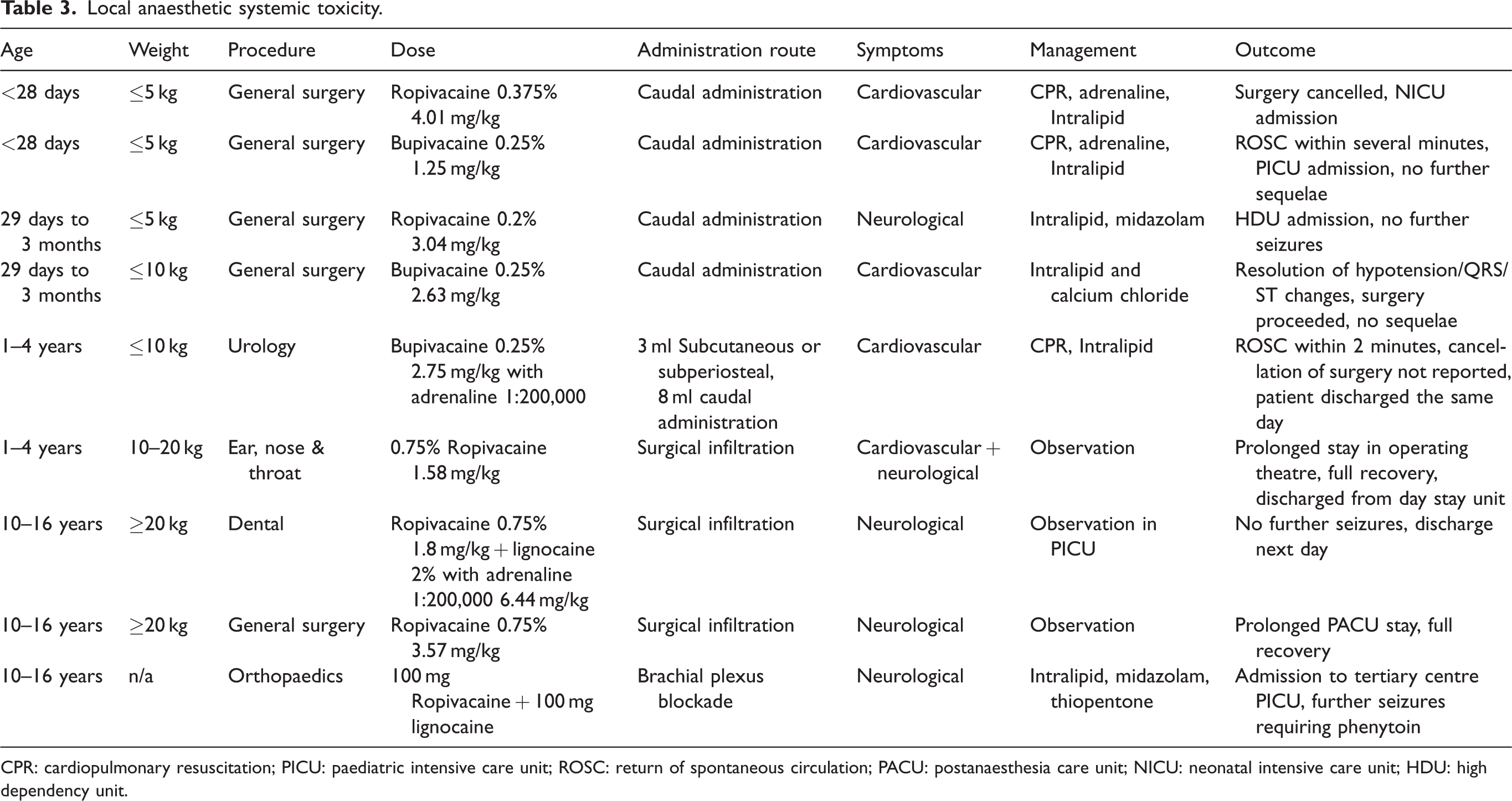
CPR: cardiopulmonary resuscitation; PICU: paediatric intensive care unit; ROSC: return of spontaneous circulation; PACU: postanaesthesia care unit; NICU: neonatal intensive care unit; HDU: high dependency unit.
Planning, logistics and communication.
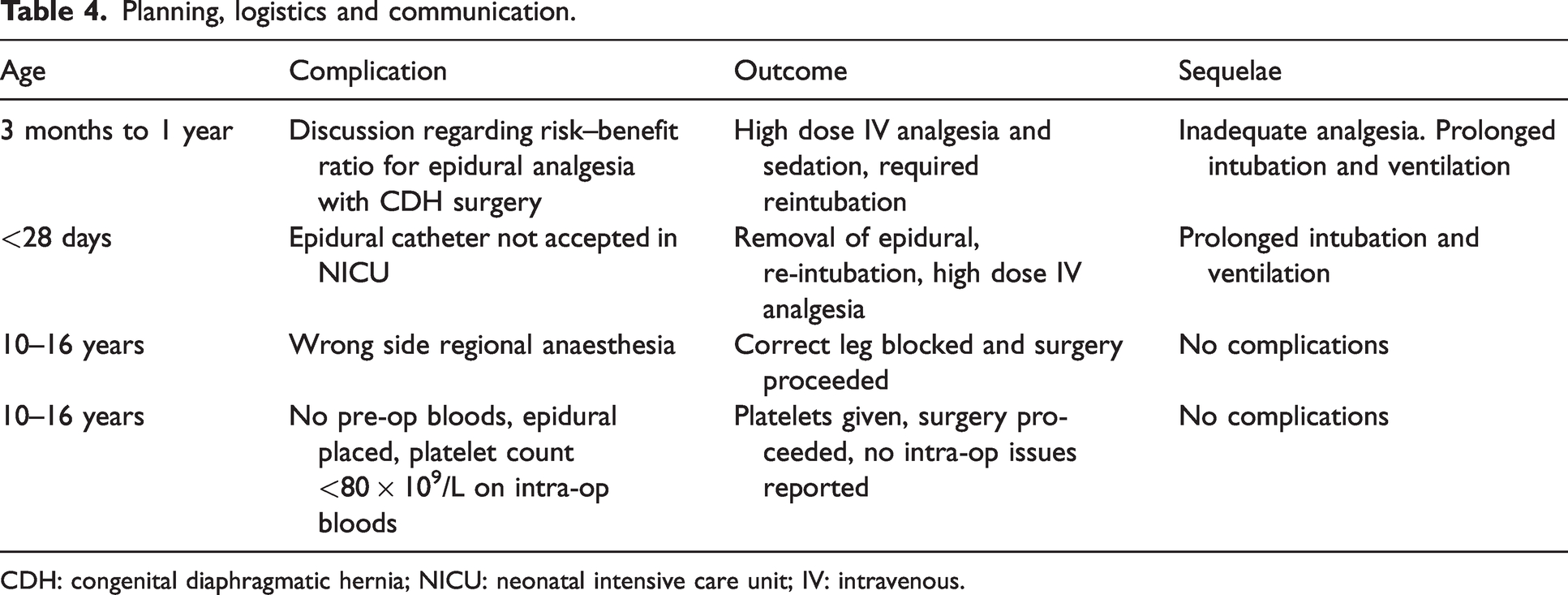
CDH: congenital diaphragmatic hernia; NICU: neonatal intensive care unit; IV: intravenous.
Incidents in which regional anaesthesia indirectly contributed to error.
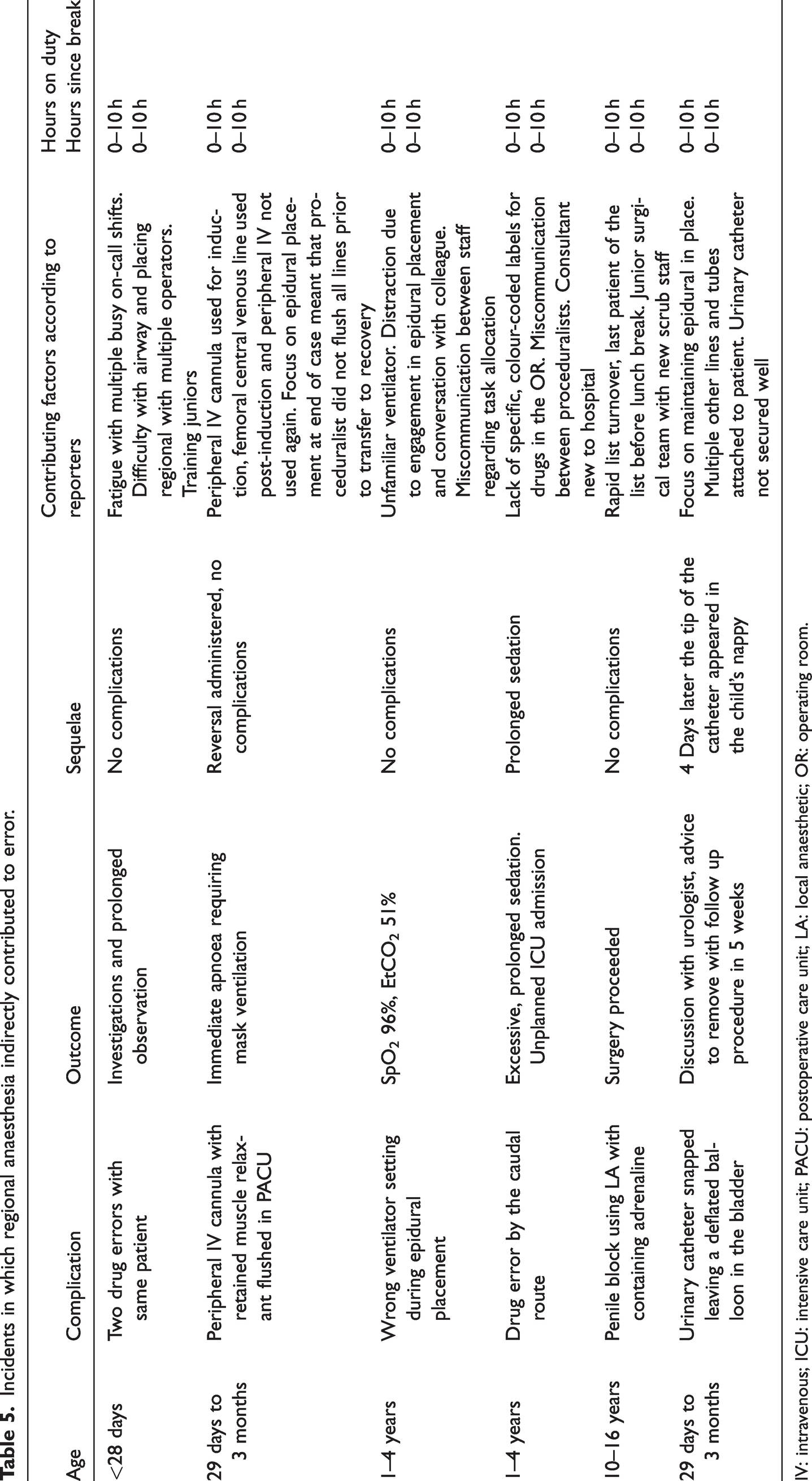
IV: intravenous; ICU: intensive care unit; PACU: postoperative care unit; LA: local anaesthetic; OR: operating room.
Discussion
WebAIRS is a voluntary incident reporting system, and the denominator is not routinely collected. Previous sub-audits have reviewed numerator and denominator data using the webAIRS platform 5 , 6 suggesting an anaesthetic incident rate of 0.25%, or one in 400 anaesthetics. It should be stressed that this is the voluntary reporting rate rather than a true measure of incidence. In comparison, the Anaesthesia Practice In Children Observational Trial (APRICOT), reporting paediatric perioperative respiratory and cardiac events, described an incident rate of one in 19 anaesthetic procedures. 7 Although there are only 26 reports in this series it is the narratives that yield an insight into how these incidents evolved and allow the analysers to examine lessons that might be learned from these data.
Multi-centre registries such as the Pediatric Regional Anesthesia Network (PRAN) contribute to cumulative knowledge on the safety of paedatric regional anaesthesia and promote standardised care. Data from all performed regional anaesthetic techniques are prospectively collected across several tertiary paediatric institutions in North America. In 2012 PRAN published the complications of paediatric regional anaesthesia in 14,917 patients and reported zero incidence of LAST. 8 A subsequent publication including 100,000 paediatric patients identified seven cases of severe LAST (seizures or arrest) and 11 cases of mild symptoms. 3 Given the findings of our enquiry and the likelihood of underreporting, the development of such a resource in Australasia would be of great value.
Technical issues
Reported incidents ranged from minor to unexpected and unusual events. The first incident described the events following a combined single shot caudal plus spinal in a neonate for an awake general surgical procedure. The patient was a premature neonate with multiple comorbidities, including apnoea of prematurity and chronic lung disease requiring oxygen therapy. Anaesthesia was initially routine with 0.2 mL/kg of 0.5% bupivacaine injected intrathecally followed by 0.9 mL/kg of 0.2% ropivacaine plus 1 mL normal saline caudally (equating to a total of 2.7mg/kg local anaesthetic). Shortly after the caudal injection, the neonate displayed signs of respiratory distress leading to hypoxia, bradycardia and hypotension, requiring face-mask ventilation and subsequent intubation. The surgical procedure was then performed under general anaesthetic. The patient was extubated post-procedure to their preoperative oxygen supplementation, with no further sequelae. The reporter surmised that the combined regional technique contributed to this event. They hypothesised that injection of the caudal local anaesthetic caused extension of spinal anaesthesia through compression of the dura.
Combined caudal with spinal anaesthesia is a novel technique for awake neonatal anaesthesia. 9 , 10 More commonly described is the placement of a caudal catheter for additional local anaesthetic administration at the time when the spinal anaesthesia recedes, rather than a simultaneous single-shot injection. 10 A simultaneous single-shot caudal plus spinal technique may pose additional risk 11 of adverse events, particularly related to dosing. The described incident may demonstrate ‘epidural volume extension’, a concept more commonly described with adult neuraxial anaesthesia. 11 The compressive effects of a volume of injectate in the epidural space may cause cranial extension of spinal injectate. Although dosing recommendations to either space are contested, a dose reduction for spinal anaesthesia in the presence of epidural anaesthesia is suggested for adults. 11 Extrapolating to infants and this incident, it is possible that the patient may have experienced ‘high spinal’ anaesthesia due to maximum spinal anaesthetic dosage and maximum caudal anaesthetic dosage. However, the differential diagnoses include the possibility of intrathecal spread of epidural drug, possible subdural injection or even LAST. Further research and experience are required to describe the safety of this technique and appropriate drug dosages.
There were four further incidents reported in which minor technical issues contributed: two involved attempted epidural catheter insertion with accidental dural puncture in pre-school aged children. Another patient with cerebral palsy and scoliosis had an epidural sited pre-surgically for a complex orthopaedic procedure. Intraoperatively the epidural was not providing the expected level of analgesia and was resited postoperatively with better results. The final case involved an ultrasound-guided paravertebral block in a pre-school aged patient. The surgeons noted a breach of the parietal pleura on thoracoscopy, with localised air leak. This resolved by the end of the case and the patient received a pleural drain.
The above incidents demonstrate recognised complications and highlight the potential challenge of regional anaesthesia in young paediatric patients, children with abnormal musculoskeletal anatomy, and less frequently utilised techniques in paediatric anaesthetic practice. It is reassuring that none of the patients were reported to suffer from severe sequelae, and adequate pain control was still achieved with a regional technique in all cases.
Equipment issues
A 20 gauge Abbocath intravenous catheter was sheared during single shot injection into the caudal space. The authors provided limited information about the specific cause of this incident and categorised this as a medical device malfunction. A 15 mm segment of the catheter remained lodged within the sacral hiatus. Guidance from the neurosurgery team was sought, and their advice was to leave the fragment in place. Limited information was reported for this incident and the overall outcome. Literature for the treatment of this complication is scarce and conflicting for both adults and children. Some case studies describe surgical removal of sequestered epidural catheters without complications. 12 Other case reports have advised to leave the catheter in situ, provided it is not positioned intrathecally. 13 , 14 The consequences of an in situ catheter for a developing child are largely unknown, but are postulated to be infection, fibrosis, catheter migration and nerve injury. In all case reports urgent neurosurgical opinion and cross-sectional imaging (computed tomography) were obtained to locate the fragments and dictate the next course of action. Lenox et al. 12 suggest as a general rule, that catheters retained within the skin but outside the epidural canal can be easily removed. For catheters within the spinal canal, a multidisciplinary discussion involving anaesthetists, neurosurgeons and the family should weigh the pros and cons of operative intervention versus a more conservative approach. 12 The authors suggest that preventative strategies, such as meticulous handling of the catheter and avoidance of removing and reintroducing the needle through the cannula may prevent micro and macroscopic shearing of plastic fragments.
Another incident describes a chemical burn in a child whose back was prepped for the regional anaesthetic using chlorhexidine and alcohol. Following epidural siting, a diathermy plate was affixed to the patient’s back and the patient was positioned supine for surgery. At the completion of surgery, the diathermy plate was removed, and marked redness and blistering were found at the site. This was thought to be a chemical burn caused by prolonged contact with chlorhexidine.
Chlorhexidine-related burns are well described in paediatric literature, but most involve small infants in whom the risk of serious injury is high.
16
Unfortunately, this minor mishap in an older child resulted in significant harm and serves as a reminder of the risks of everyday surgical preparation. The key tenets of burn risk reduction are well described and should be applied to all children:
17
application of the minimum amount of chlorhexidine solution; removal of excess solution from soaked materials near skin; monitoring prepped skin frequently to detect cutaneous adverse effects.
Local anaesthetic systemic toxicity
Local anaesthetic systemic toxicity is an uncommon, potentially fatal critical incident. There are unique considerations in the paediatric population, and descriptions of such events to this date are limited. In the webAIRS dataset, the authors identified nine possible LAST cases, four of which presented with cardiovascular instability and four with neurological signs. One incident involved both manifestations. All cases involved single injection techniques.
Cardiovascular instability
Cardiovascular instability was defined as significant hypotension or arrest requiring cardiopulmonary resuscitation (CPR). All cases in this series were patients younger than one year of age or less than 10 kg in weight, representing our most fragile paediatric population. Three of the incidents involved neonates, two of whom were ex-premature. All of these incidents involved caudal anaesthesia, the most commonly performed regional technique in the paediatric population. 3
Three of these patients suffered cardiac arrest (two with ventricular tachycardia/fibrillation, one asystolic) requiring CPR. Reporters described additional technical challenges such as extravasation from an intravenous cannula during resuscitation, requiring endotracheal administration of resuscitation drugs and intraosseous needle placement. Fortunately, based on the narratives, all events resolved quickly requiring a maximum of two doses of adrenaline and promptly administered lipid emulsion. The surgery was cancelled in two of the three incidents, with both patients requiring prolonged intubation and ventilation in the paediatric intensive care unit (PICU).
The fourth patient presenting with cardiovascular instability featured hypotension with QRS and ST segment changes. These resolved with calcium and lipid administration. Surgery proceeded uneventfully for this child, and reporters described no significant change in expected outcome.
Paediatric regional anaesthesia is most often performed under general anaesthesia or sedation, with a history of safety supporting this approach. 3 However, lack of direct patient feedback through reported symptoms means that neurological signs and symptoms may be missed, and cardiovascular signs may be the first presentation of LAST. Similarly, awake preverbal or non-verbal children are unable to communicate sensations such as circumoral tingling and tinnitus, complicating early detection and diagnosis. Observed seizure activity with awake regional techniques may yield a quicker diagnosis. 18 Highlighted in this series is the inherent difficulty with procedures in small, frail infants, particularly during a crisis. Reassuringly, management was prompt, followed established guidelines, and was successful resulting in no documented permanent sequelae.
While regional database studies have not demonstrated a significant correlation between American Society of Anesthesiologists physical status classification and the risk of LAST, 3 the incidents described here all feature infants with medical comorbidities. Infants and neonates also have an inherent propensity to drug toxicity due to physiological immaturity. The overall incidence of LAST in paediatric patients has been estimated to be between 0.7 and six per 10,000, with the highest risk in infants less than 6 months old and with a neuraxial approach. 3 , 4 , 19 Paediatric pharmacology literature identifies several high-risk groups for the development of LAST. 20 Neonates have less than half the amount of alpha-acid glycoprotein of adults, resulting in a higher free fraction of local anaesthetic in plasma.20,21 Neonatal and infant hepatic metabolic pathways are also immature, contributing to slow clearance. The result is an increased risk of LAST in children under one year of age. Prematurity, cardiac, renal, and hepatic dysfunction reduce metabolism and protein binding, further adding to this risk.
Specific studies of bupivacaine suggest that neonates and infants are more susceptible to central nervous system (CNS) toxicity than adults, 20 thus lower plasma concentrations may produce LAST in this group. Accordingly, a lower maximum dose has been recommended in a recent consensus document. 21 A study in healthy adult volunteers demonstrated that higher plasma concentrations of ropivacaine are tolerated compared with bupivacaine, and cardiovascular signs and symptoms are less pronounced. 22 While based on an adult population, this suggests that ropivacaine has a greater safety margin with regard to toxicity than bupivacaine. Controlled studies comparing ropivacaine and bupivacaine have demonstrated equivalent potency, although ropivacaine demonstrates a shorter duration motor block. 23
Neurological sequelae
A range of neurological symptoms was seen in five incidents. Three patients presented with seizures in the postanaesthetic care unit (PACU).
The first report describes a neonate who received 3 mg/kg of ropivacaine by caudal epidural injection while under general anaesthetic. While awake in the recovery room, approximately 45 minutes after the caudal injection, the baby began to seize. A total of four seizures occurred, each around 30 seconds duration. Two doses of lipid emulsion and a dose of midazolam were administered during this time, with successful termination of seizure activity. Investigations were normal and no further seizure activity occurred. A second case involved an upper limb block in a young patient taking antidepressant medication. While in the recovery room, the patient lost consciousness, desaturated and seizure activity occurred. The patient was treated with lipid, midazolam and thiopentone. Further seizures occurred overnight, requiring a phenytoin load (initially avoided due to contraindication in LAST). All investigations including EEG were normal and the patient was reported to be neurologically intact between episodes. Follow-up of the patient revealed ongoing seizures in the community.
An adolescent undergoing dental surgery under general anaesthesia received local infiltration of 1.8 mg/kg ropivacaine and 6.4 mg/kg lignocaine with adrenaline. Two hours post-procedure, the patient had three seizures lasting less than 5 minutes each. This patient was admitted to the PICU for observation, with no further sequelae. The fourth case was a young patient undergoing laparoscopic surgery who received 3.6 mg/kg of ropivacaine during surgical infiltration. In the PACU the patient was notably confused, and the reporter documented the possibility of local anaesthetic CNS toxicity. This patient was observed for two hours, with slow resolution.
The remaining LAST incident presented intraoperatively with combined cardiovascular and neurological symptoms. This incident involved a young patient undergoing an ear, nose and throat procedure. At the completion of surgery, the patient received local infiltration of 1.6 mg/kg ropivacaine 0.75%. The patient became tachycardic and apnoeic with fixed pupils lasting about 5 minutes. Following this, emergence from anaesthesia was prolonged, with apnoea for over 40 minutes. The reporter described the patient as neurologically appropriate following emergence and recovery was uneventful. Lipid was available but not given.
Clinical signs can be non-specific and differential diagnoses broad; physiological derangement related to the patient, surgery or anaesthetic technique should be excluded. Postoperative neurological signs can occur due to reversible or transient sequelae such as emergence delirium, drug toxicity, syncope, metabolic and cerebral pathology or manifestations of mental health conditions. In young patients, surgery may be the first encounter with medical services. Anaesthesia may uncover a new diagnosis, for example, epilepsy, given the propensity of commonly used agents to reduce seizure threshold. The perioperative process may challenge patients with mental health conditions, given the high levels of stress associated with this time. The initial diagnosis of LAST may affect treatment possibilities in the short-term (i.e. choice of anticonvulsants). In all cases, further history, investigations and appropriate specialist consultation were sought by the reporters. All patients were managed safely, did not suffer serious sequelae, and were followed up thoroughly by the treating anaesthetist.
Current American Society of Regional Anesthesia (ASRA) and European Society of Regional Anaesthesia (ESRA) guidelines recommend that paediatric doses should not exceed 1 mL/kg for both 0.2% ropivacaine (2 mg/mL) and 0.25% bupivacaine (2.5 mg/mL). 21 , 24 Inconsistent dosing was a feature of the incidents reported to webAIRS, with many of the reported cases receiving doses above those recommended. Large database studies 24 also report a wide variation in dosing practice, with 25% of patients receiving local anaesthetic doses higher than recommended. This was most common in the youngest patients and with the use of ropivacaine, and given our similar findings, indicate an area for targeted practice review. 24
Careful administration is equally important. Two patients who received caudal bupivacaine developed the signs of LAST following negative aspiration and during a deliberate pause midway through administration of the dose, highlighting the false-negative potential of a dry aspirate. Nevertheless, these cases highlight the value of slow and incremental injection of local anaesthetic as the intended full dose was not delivered. Test doses are widely promoted for neuraxial anaesthesia and are associated with a reduced complication rate. 24 The use of ultrasonography to confirm anatomy and correct placement of caudal anaesthesia provides added safety. 25 Compared with non-ultrasound guided techniques for paediatric regional anaesthesia, a Cochrane review has shown higher success rates, lower early postoperative pain scores, prolonged duration of analgesia and shorter block procedure times with use of ultrasound. 26 Surgical infiltration features in three cases, and while considered relatively benign, in these incidents involved high concentrations and high volumes. Communication between surgeon and anaesthetist is encouraged to cross-check appropriate dosing.
On a positive note, one reporter described the benefits of an in situ simulation of a LAST crisis a week prior to this incident. The clinical management, including location and dosing of lipid, was described as rapid and effective due to familiarity with the process. A growing body of evidence supports the benefits of integrated simulation education in improving procedural performance, medical knowledge, adherence to life support protocols and teamwork and communication skills (Figure 2). 18,27,28
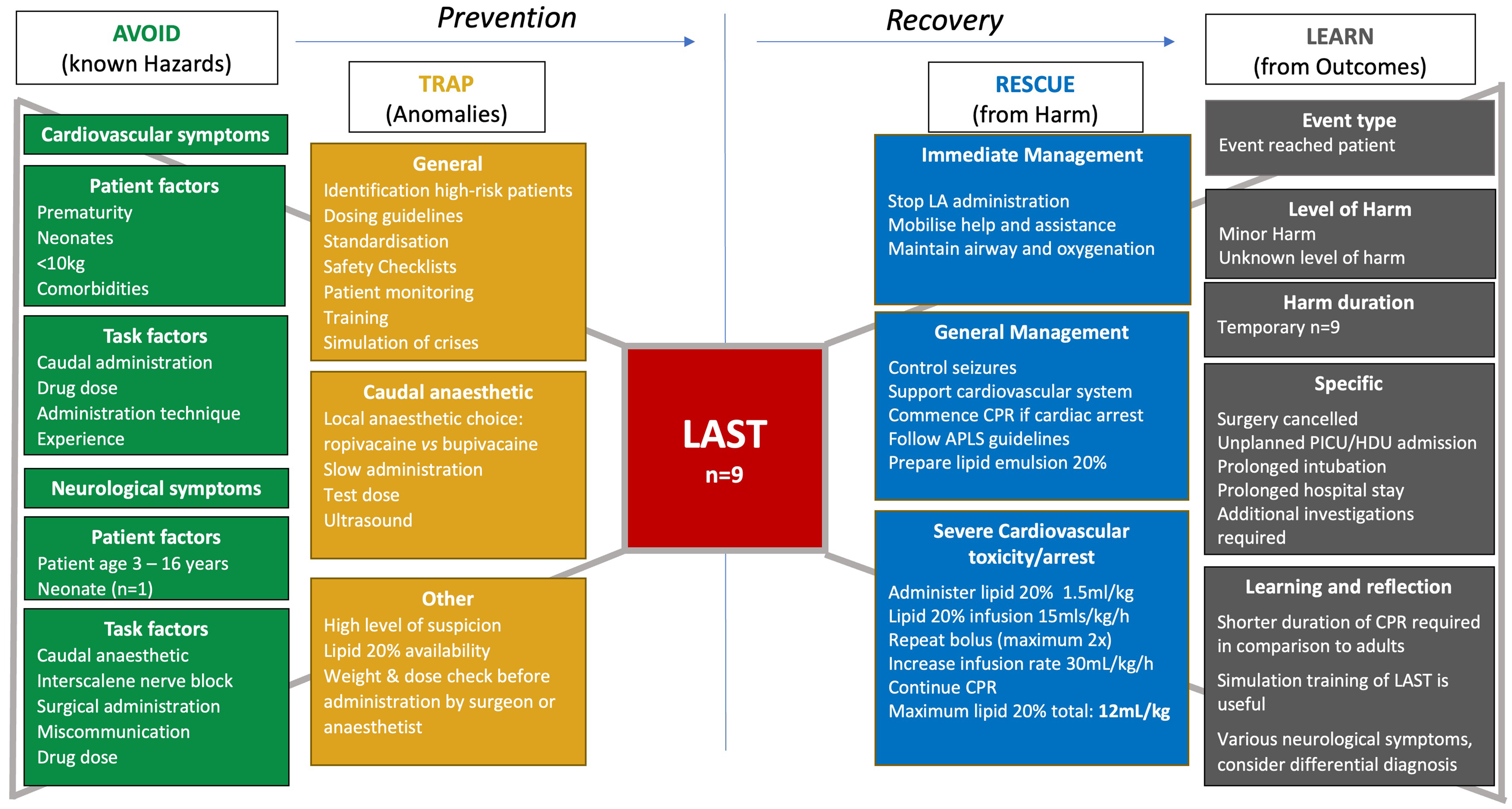
Local anaesthetic systemic toxicity bowtie diagram. LA: local anaesthetic; APLS: advanced paediatric life support; PICU: paediatric intensive care unit; HDU: high dependency unit; CPR: cardiopulmonary resuscitation; LAST: local anaesthetic systemic toxicity.
Planning, logistics and communication
Miscommunication can lead to unexpected changes in management and patient progress. One reporter described issues with complex pain management in a high-risk neonate. An epidural catheter was requested postoperatively to facilitate respiratory wean following open congenital diaphragmatic hernia (CDH) repair. The overall risk–benefit ratio for this regional technique was contested between the involved medical teams. It was argued that insertion of the catheter would necessitate intubation and ventilation. Ultimately, the patient did not receive an epidural catheter but required re-intubation and ventilation for high dose sedative analgesia for 5 days postoperatively. The reporter noted that the outcome for this patient was affected by lack of regional anaesthesia. Contributing factors included incomplete preoperative discussion regarding surgical and anaesthetic plans. Pre-procedure epidural catheter placement was not considered as a result, possibly leading to insufficient analgesia for this patient.
Regional anaesthesia in neonates remains a challenge from a technical perspective, requiring the skill of an experienced paediatric anaesthetist. Dosing is a challenge given that the volumes required for effective analgesia may approach toxic limits. Literature evaluating epidural analgesia in neonatal CDH surgery is limited. A small retrospective study describes an association between epidural analgesia and reduced ventilator days in patients with low-risk CDH. 29 Only limited clinical information was available in this report; so the authors cannot exclude additional clinical factors (such as severity of CDH) contributing to this outcome. This incident emphasises the importance of informed multidisciplinary planning to ensure the best analgesic modality is offered preoperatively to optimise patient outcome.
Familiarity with paediatric regional analgesia across departments and institutions may vary. Another reporter describes the issue of disposition in a neonate with caudal epidural analgesia for a general surgical procedure. A perioperative analgesia plan was communicated between the patient’s family, the treating anaesthetist and neonatal intensive care unit (NICU) clinicians. Postoperative extubation and analgesia by caudal epidural infusion were planned and performed. Unfortunately, the patient was not accepted to the NICU postoperatively due to the presence of the caudal epidural analgesic infusion. Transfer to the PICU was attempted but was not possible due to capacity issues. Unfortunately, the catheter had to be removed and the neonate required high dose intravenous opioid administration, requiring re-intubation and ventilation for over 48 hours. In this case, despite exposure to the risks, the full benefit of neuraxial anaesthesia was limited, and the neonate was exposed to repeated intubation and prolonged ventilation.
Both incidents describe the potential value of regional anaesthesia in neonates. However, lack of familiarity with management and monitoring can limit the scope of these modalities. Ongoing training and provision of resources from anaesthesia and pain services relevant to regional analgesic techniques is needed to increase comfort with management in less experienced environments. Important information may be lost during handover between teams and departments during high stakes interventions, with complex patients and when personnel are unfamiliar or infrequently interact. To mitigate this, formal, standardised pre and postoperative handovers between NICU, anaesthesia and surgical teams are proposed. Standardisation has reduced errors in handover reports, time to delivery of analgesia and antibiotics; and the incidence of respiratory and haemodynamic interventions postoperatively. 30 In the authors respective hospitals, cognitive aids and dedicated handover time with senior staff have helped to identify common goals and expectations from the outset of theatre admission and ensure a shared plan exists for postoperative care. This process raises the opportunity for questions and concerns to be addressed for our most high-risk patients.
‘Stop-before-you-block’
There were two cases in which preoperative assessment was incomplete and led to avoidable incidents. The first was an elective orthopaedic lower limb procedure under general and regional anaesthesia. The supervising consultant and trainee visualised the sonoanatomy and successfully administered local anaesthetic. The surgeons then entered the room to mark the limb and it was discovered that the wrong site had been anaesthetised. On reflection, the reporter mentioned the lack of pre-surgical marking, failure to perform a pre-block ‘time-out,’ and the perioperative team not ‘speaking up’ when the block was incorrectly performed as contributing factors.
Diligent use of the World Health Organization surgical safety checklist involving all perioperative team members is part of the process to reduce wrong-site events and other patient or surgery-specific risks. 31 Surgical site marking should occur prior to the patient entering the operating theatre. A patient ‘sign-in’ process should occur prior to the administration of anaesthesia, reviewing the correct operative site and procedure with the consent documentation, with the patient or caregiver present to confirm this.
Specific to regional anaesthesia, a ‘stop-before-you-block’ process is recommended by expert groups and anaesthesia training bodies for all unilateral techniques. 32 This final check is completed with the anaesthetist, their assistant and other available theatre staff. This is performed alongside consent documentation, with visualisation of the surgical site marking just before needle meets skin.
Active followership and ‘speaking up’ may be limited in the theatre environment for a range of reasons. Lack of a shared mental model, limited psychological safety and differing cultural norms around communication feature commonly. Solutions to dismantle the above include surgical briefing at the commencement of the day. Team introductions and a discussion around clinical objectives and delegation of tasks has been shown to improve team awareness and behaviours including mutual respect.27,33 Team training and rehearsal of non-technical skills through multidisciplinary simulation may also enhance information sharing and teamwork. ‘Speaking up’ is a complex interaction with potentially high stakes for the speaker and the receiver. Active effort positively to reframe and encourage ‘speaking up’ by using a positive receiver response can strengthen team function and ultimately improve patient safety. 34
The second report describes a complex patient with cerebral palsy, respiratory and musculoskeletal comorbidities for major lower limb surgery. This patient had undergone an elective preoperative assessment with a plan for epidural catheter insertion under general anaesthetic. After induction, blood tests were taken, and an epidural was performed. On checking the blood results intraoperatively, it was noted that the patient’s platelet count was less than 80 × 109/L. The patient was monitored and followed up postoperatively with no neurological sequelae. The reporter of this incident cited the lack of appropriate preoperative investigations as a key contributing factor to this event.
Logistical issues may complicate preoperative assessment. Major paediatric operations are performed in a small number of tertiary centres across Australasia, requiring some patients to travel large distances for clinical assessment and treatment. Clinical notes and investigations may not be easily accessible by referral centres, and additional laboratory investigations may be missed. Prior to major operative procedures in a medically complex patient, thorough medical assessment including investigations are prerequisite to optimise and plan safe care. Preoperative investigations may need to be repeated by the treating anaesthetist and their importance is highlighted here. 35
Regional anaesthesia indirectly contributing to error
There were six incidents in which the performance of regional anaesthesia was reported to contribute to medication-related errors or case complexity. Four of these cases describe accidental administration of the wrong drug, wrong dose, or by the wrong route. Another case describes the failure to initiate mandatory ventilation, and the final case involves damage to an indwelling urinary catheter. Contributing factors mentioned by the reporters included distraction due to multiple competing priorities (specifically, the placement or monitoring of the regional anaesthesia), cognitive overload, fatigue due to prolonged and repeated on-call commitments, inadequate communication and inadequate experience.
The first case involved failure to flush an intravenous cannula. When the cannula was flushed in the PACU the patient became apnoeic and desaturated, requiring rescue ventilation and administration of reversal agent. The reporter mentioned epidural catheter placement at the end of an unexpectedly extensive procedure as a contributing factor to the oversight to flush the cannula.
The second incident involved two drug errors in a neonate. In this incident, the reporter mentioned a failed spinal anaesthetic which resulted in stress and an alternative anaesthetic technique as a contributing factor. In the third incident, a 10 mL syringe containing 150 μg of clonidine was administered caudally instead of the planned local anaesthetic. Just prior to this incident there was a failed caudal injection resulting in changeover of the proceduralist. The second operator accessed the caudal space successfully but administered the contents of the wrong syringe, which was prepared on the same tray. The fourth report describes the administration of local anaesthetic with adrenaline for a penile block. Surgical staff with limited experience were involved in preparing and administering the local anaesthetic. No harm resulted from this incident. The remaining case involved regional blockade under general anaesthesia, in which, following intubation, epidural placement commenced without initiating mandatory ventilation. Apnoea was identified early and managed prior to clinical deterioration.
Medication errors are an unfortunately relatively common and predominantly preventable adverse event in anaesthesia. In the paediatric population weight-based dose variation contributes to complexity. 36 , 37 Similar database studies, such as Wake Up Safe, 37 have highlighted the frequency of such errors and the need for organisational systems change. Suggested methods involve the standardisation of anaesthesia environments, drug labelling and concentrations to minimise variability and reduce the cognitive load of the anaesthetist in situations in which competing priorities may complicate routine tasks.
In the final incident, a urinary catheter was snapped into two pieces during the transfer of a patient. One piece was retained in the patient’s bladder. The patient’s management was described as complex, requiring multiple connected drains and lines including an epidural catheter. The reporter commented their focus was to maintain the epidural in place during transfer. After consultation with the urology team, the remaining fragment of urinary catheter was planned to be cystoscopically removed with a later procedure. It passed naturally, however, and was found in the nappy a few days later. Patient transfer is a high-risk moment, and close attention is required from the entire team to avoid iatrogenic harm. The importance of a pre-transfer screen of the patient with effective teamwork and delegation of tasks to avoid fixation is highlighted here. 15
The addition of regional techniques may generate stress for the anaesthetist and surrounding team. Issues include time pressure associated with list turnover, technical difficulties, mentoring junior trainees, and limited experience of the wider team while simultaneously monitoring the anaesthetised patient. Such distractions are human factors which can contribute to harm or uncover latent safety threats. Therefore, the authors recommend the introduction of a second experienced anaesthetist during the performance of regional techniques to share the cognitive load and consequently reduce the stress experienced by the procedural anaesthetist (and operative team).
Limitations
WebAIRS is a voluntary, de-identified incident reporting system. Data are collected by tick-boxes and non-mandatory narrative fields. Quality of data depends on depth of information provided by reporters, which can be incomplete and cannot be retrieved retrospectively. While incident reports are a valuable source of information, they have general limitations. Reports can be subjective and influenced by the views and experiences of the reporter; and can be affected by reporter bias or selective recall. While the authors of this paper aim to provide an objective, useful overview of the incidents, hindsight bias may affect the presentation of information. This paper presents only a snapshot of paediatric regional anaesthesia incidents. As no denominator data are available, it is impossible to provide accurate measures of risk for any identified hazards.
Conclusion
Final reported outcomes from these incidents ranged from no harm to minor harm, but clinical presentations were dramatic generating valuable discussion. Caudal anaesthesia is commonly performed in children and was featured in a significant fraction of reported incidents. Technical difficulties and complications in small, frail patients emphasise the value of specialist paediatric anaesthetists in dedicated referral centres. Lack of familiarity with techniques and management of regional anaesthesia led to avoidable incidents. Standardised initiatives such as surgical safety checklists, ‘stop-before-you-block’, and interdisciplinary handover tools have improved patient safety, but are not always used. Variation in dosage and administration technique for local anaesthesia contributed to several events. Despite this, regional techniques can be an elegant and beneficial complement to paediatric anaesthesia. Indeed, the lack of regional anaesthesia in some reports has led to prolonged intubation and ventilation and potentially longer hospital stays. Several reporters highlighted the role of human factors such as distraction and fatigue contributing to the incidents. Meticulous technique, teamwork, clear communication and obsessive vigilance are essential attributes for paediatric anaesthetists and are required to care for our smallest patients.
Footnotes
Author Contribution(s)
Acknowledgements
The authors would like to thank the large number of anaesthetists across Australia and New Zealand who are reporting incidents to webAIRS in the interests of patient safety. The authors acknowledge the contribution of all members of the Australia and New Zealand Tripartite Anaesthetic Data Committee (ANZTADC), past and present, and the administrative assistance provided by ANZCA staff. Special thanks to Dr Martin Culwick, director of ANZTADC, and to Linda Culwick for their contributions to the editing and review of this manuscript.
Declaration of conflicting interests
The authors declare the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Yasmin Endlich is the current coordinator of the webAIRS publications group.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.